Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Bruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)Document306 pagesBruce Ecker, Laurel Hulley - Depth Oriented Brief Therapy - How To Be Brief When You Were Trained To Be Deep and Vice Versa-Jossey-Bass (1995)John Smith85% (13)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- UNIT 04 TV Activity Worksheets PDFDocument3 pagesUNIT 04 TV Activity Worksheets PDFCristina33% (6)
- ANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFDocument11 pagesANALISIS PENERAPAN SISTEM LOCKOUTTAGOUT (LOTO) PADA BAGIAN OPERASI DAN PEMELIHARAAN DI PT. X TANJUNG EMAS KOTA SEMARANG (Berdasarkan Standar OSHA 29 CFR Part 1910.147 Dan Part 1910.333) PDFAfif Fayadh VictoryNo ratings yet
- Department of Labor: Bct-Fy01Document101 pagesDepartment of Labor: Bct-Fy01USA_DepartmentOfLabor100% (1)
- An Appraisal On Occlusal Philosophies in Full-Mouth Rehabilitation A Literature ReviewDocument4 pagesAn Appraisal On Occlusal Philosophies in Full-Mouth Rehabilitation A Literature ReviewaggrolNo ratings yet
- Brain Workshop - a Dual N-Back game - نسخةDocument4 pagesBrain Workshop - a Dual N-Back game - نسخةBTQNo ratings yet
- Aim Global TieupsDocument84 pagesAim Global Tieupsjhorgecruz18No ratings yet
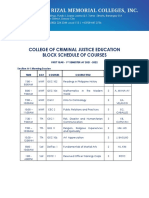
- College of Criminal Justice Education Block Schedule of CoursesDocument12 pagesCollege of Criminal Justice Education Block Schedule of CoursesKristel Ann ManlangitNo ratings yet
- Speed ManagementDocument284 pagesSpeed ManagementAdel AhmedNo ratings yet
- Masterclass in MatchaDocument39 pagesMasterclass in MatchatomasiskoNo ratings yet
- Language Disorders - 5Document27 pagesLanguage Disorders - 5Marta Sampedro GonzalezNo ratings yet
- The Pathophysiology and Genetics of OCDDocument12 pagesThe Pathophysiology and Genetics of OCDCrescent FangNo ratings yet
- For DissertationDocument13 pagesFor DissertationRegi viniciyaNo ratings yet
- Swimming Pools and Spa Pools: Standard For The Operation ofDocument40 pagesSwimming Pools and Spa Pools: Standard For The Operation ofakramNo ratings yet
- Analisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihDocument12 pagesAnalisis Penerapan Metode Activity Based Costing (ABC) Dalam Menentukan Tarif Jasa Rawat Inap Di RSUD Kota PrabumulihAffira AfriNo ratings yet
- 10besar Kode PenyakitDocument5 pages10besar Kode PenyakitDEWINo ratings yet
- Clinical AssignmentDocument9 pagesClinical AssignmentkomalNo ratings yet
- Factor Affecting The Development of FetusDocument8 pagesFactor Affecting The Development of FetusWhye Jun CheongNo ratings yet
- Future Biotechnology: The Eurobiotech JournalDocument4 pagesFuture Biotechnology: The Eurobiotech JournalsaraNo ratings yet
- "After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghDocument38 pages"After All, There Is Nothing As Interesting As People, and One Can Never Study Them Enough" Vincent Van GoghAnonymous 1gH7ra9ANo ratings yet
- CONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2ADocument11 pagesCONDUCTING FAMILY HEALTH ASSESSMENT TOOL Geno Adrian T. Pampanga BSN-2AGeno Adrian T PampangaNo ratings yet
- One Health Concepts and Knowledge Presentation SlidesDocument48 pagesOne Health Concepts and Knowledge Presentation Slideskarunia nihaya100% (1)
- 4.4.3.3 Data and Trend AnalysisDocument6 pages4.4.3.3 Data and Trend AnalysisIndermohan MehtaNo ratings yet
- 1574-Article Text-2641-1-10-20181107Document5 pages1574-Article Text-2641-1-10-20181107Faraz HaiderNo ratings yet
- Microbial PathogenesisDocument8 pagesMicrobial PathogenesisRachelleNo ratings yet
- Chemical and Nutritional Changes in Food During ExtrusionDocument30 pagesChemical and Nutritional Changes in Food During ExtrusionZubi BaigNo ratings yet
- Journal Medicine: The New EnglandDocument7 pagesJournal Medicine: The New EnglandTony RamirezNo ratings yet
- ELIGIBILITY BKPDocument1 pageELIGIBILITY BKPLydia FrederickNo ratings yet
- "ERC" Elite Recruitment CompanyDocument11 pages"ERC" Elite Recruitment CompanyJenniferNo ratings yet
- Ing GrisDocument4 pagesIng GrisaniNo ratings yet