Download as ppt, pdf, or txt
You might also like
- Diagnosis in OrthopaedicsDocument48 pagesDiagnosis in OrthopaedicsBakta Giri50% (2)
- General Principles of Fracture ManagmentDocument55 pagesGeneral Principles of Fracture ManagmentkylieverNo ratings yet
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- 20090204-Clinical Enzymology Questions and Answers Final For WebsiteDocument6 pages20090204-Clinical Enzymology Questions and Answers Final For WebsiteMohanad Jawad67% (6)
- Prato 1999Document3 pagesPrato 1999Paola LoloNo ratings yet
- Benign Bone TumoursDocument106 pagesBenign Bone TumoursBharath NarasimhaNo ratings yet
- Bone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaDocument85 pagesBone Tumours: Natasha Eleena Nor Maghfirah Hani Farhana Nur FadhilaWan Nur AdilahNo ratings yet
- Technique of Reduction and Fixation of Unicondylar Medial Hoffa FracturDocument5 pagesTechnique of Reduction and Fixation of Unicondylar Medial Hoffa Fracturaesculapius100% (1)
- Benign Bone TumorDocument42 pagesBenign Bone Tumorsaqrukuraish2187No ratings yet
- Syllabus Ms OrthoDocument8 pagesSyllabus Ms OrthoMuthu KumarNo ratings yet
- Mallet Finger Suturing TechniqueDocument5 pagesMallet Finger Suturing TechniqueSivaprasath JaganathanNo ratings yet
- David Warwick (Editor), Ashley Blom (Editor), Michael Whitehouse (Editor) - Apley and Solomon - S Concise System of Orthopaedics and Trauma-CRC Press (2022)Document763 pagesDavid Warwick (Editor), Ashley Blom (Editor), Michael Whitehouse (Editor) - Apley and Solomon - S Concise System of Orthopaedics and Trauma-CRC Press (2022)filip100% (1)
- Giant Cell TumorDocument22 pagesGiant Cell TumorMaxmillian Alexander KawilarangNo ratings yet
- 2007 JBJS External Fixation How To Make It Work PDFDocument15 pages2007 JBJS External Fixation How To Make It Work PDFsuad5stambulieNo ratings yet
- Club FootDocument19 pagesClub FootJonggi Mathias TambaNo ratings yet
- Gas Gangrene in Orthopaedic PatientsDocument18 pagesGas Gangrene in Orthopaedic PatientsdennyefendiNo ratings yet
- Antibiotic Classification & Mechanism - Basic Science - OrthobulletsDocument7 pagesAntibiotic Classification & Mechanism - Basic Science - OrthobulletsYuttapol PimpisonNo ratings yet
- Fracture of Shaft Tibia FibulaDocument26 pagesFracture of Shaft Tibia Fibulagalih widodoNo ratings yet
- Femoral Neck FracturesDocument8 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
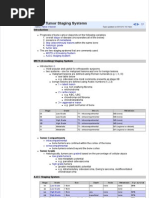
- Bone Tumour Staging - PathologyDocument2 pagesBone Tumour Staging - Pathologyo7113No ratings yet
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDocument8 pagesNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNo ratings yet
- Principles of External FixationDocument68 pagesPrinciples of External Fixationvaibhav gowda100% (1)
- WEBINAR On PEDIATRIC TRAUMADocument44 pagesWEBINAR On PEDIATRIC TRAUMAGovindarajan Hariharan100% (1)
- Approach To Fracture BoneDocument46 pagesApproach To Fracture BoneMuhaimin Noor AzharNo ratings yet
- Acetabular Fracture PostgraduateDocument47 pagesAcetabular Fracture Postgraduatekhalidelsir5100% (1)
- Extracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Document17 pagesExtracted Pages From Cervical Spine Minimally Invasive and Open Surgery 2ED 2022Carlos Miglietti100% (1)
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Document59 pagesTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNo ratings yet
- DDHDocument38 pagesDDHSanjiv GoyalNo ratings yet
- Resource Unit Wound Care EnglishDocument5 pagesResource Unit Wound Care EnglishPeterOrlinoNo ratings yet
- Master Techniques OrthopedicsDocument378 pagesMaster Techniques OrthopedicsFabio Sales VieiraNo ratings yet
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument65 pagesFractures and Dislocations About The Elbow in The Pediatric PatientPeter HubkaNo ratings yet
- Fixation Methods in OrthopaedicsDocument39 pagesFixation Methods in OrthopaedicsBhaskar BorgohainNo ratings yet
- Bone Tumours: - Jeffrey Pradeep RajDocument42 pagesBone Tumours: - Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Traumatology Orthopaedic EXAMDocument219 pagesTraumatology Orthopaedic EXAMElo GonçalvesNo ratings yet
- Basic Principles and Techniques of Internal Fixation of FracturesDocument56 pagesBasic Principles and Techniques of Internal Fixation of FracturesRudi haris munandarNo ratings yet
- Shoulder DislocationDocument29 pagesShoulder DislocationAndaleeb ZehraNo ratings yet
- AU 2017 Hip, Knee & Shoulder Arthroplasty PDFDocument380 pagesAU 2017 Hip, Knee & Shoulder Arthroplasty PDFbá anh ngôNo ratings yet
- Fractures and Dislocations About The Elbow in The Pediatric PatientDocument90 pagesFractures and Dislocations About The Elbow in The Pediatric PatientCezara TimofteNo ratings yet
- FR Distal HumerusDocument55 pagesFR Distal Humerusiisscribd100% (1)
- Classification of Bone Tumors NewDocument38 pagesClassification of Bone Tumors NewSyed WahajNo ratings yet
- Juvenile Hallux Valgus PDFDocument14 pagesJuvenile Hallux Valgus PDFŞtefaniuc IulianNo ratings yet
- Adult Pyogenic Vertebral Osteomyelitis - SpineDocument6 pagesAdult Pyogenic Vertebral Osteomyelitis - SpineL Yudhantoro YudhaNo ratings yet
- Malunions of The Distal RadiusDocument14 pagesMalunions of The Distal RadiusSivaprasath JaganathanNo ratings yet
- Damage Control Orthopedic - ASWDocument32 pagesDamage Control Orthopedic - ASWAisyah KhumairahNo ratings yet
- Classification of Bone Tumors PDFDocument5 pagesClassification of Bone Tumors PDFnmahpbooksNo ratings yet
- Classification AO PediatricDocument36 pagesClassification AO PediatricdvcmartinsNo ratings yet
- The Ortho PodDocument60 pagesThe Ortho PodxyequusNo ratings yet
- Femur Fxby TahirDocument77 pagesFemur Fxby Tahirtahir mahmood100% (1)
- Orthopaedic InstrumentsDocument19 pagesOrthopaedic Instrumentsmob3No ratings yet
- Charnley Ankle ArthrodesisDocument12 pagesCharnley Ankle Arthrodesisdr_s_ganeshNo ratings yet
- SJAMS 43B 750 754 Thesis Tibial PlateauDocument5 pagesSJAMS 43B 750 754 Thesis Tibial PlateauNisheshJainNo ratings yet
- External Fixation Principles and Applications.5Document8 pagesExternal Fixation Principles and Applications.5Leonardo Rocha100% (1)
- OsteomyelitisDocument29 pagesOsteomyelitisPramod N KNo ratings yet
- Coxitis TB Hip KneeDocument26 pagesCoxitis TB Hip KneefajarvicNo ratings yet
- Orthopedic SlidesDocument78 pagesOrthopedic SlidesAzry Mustapa100% (1)
- Orthopaedics PunchDocument6 pagesOrthopaedics PunchHicham GawishNo ratings yet
- All Papers Topic WiseDocument55 pagesAll Papers Topic WiseZ TariqNo ratings yet
- Principles of ImmobilizationDocument27 pagesPrinciples of ImmobilizationSivaneasan KandiahNo ratings yet
- Orthopedics BookDocument31 pagesOrthopedics BookAravindh Sella100% (2)
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderFrom EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderNo ratings yet
- Cognitive Rehabilitation: Model For Occupational Therapy: Beatriz Colon Abreu, Joan Pascale TogliaDocument10 pagesCognitive Rehabilitation: Model For Occupational Therapy: Beatriz Colon Abreu, Joan Pascale Togliavandrade_635870No ratings yet
- Introduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologyDocument26 pagesIntroduction To Anaesthesia: Fatiş Altındaş Department of AnesthesiologymochkurniawanNo ratings yet
- Mirizzi SyndromeDocument18 pagesMirizzi Syndromedrhiwaomer100% (6)
- Out 9Document12 pagesOut 9rezkyprayogiNo ratings yet
- Acute Gastroenteritis With Some DehydrationDocument6 pagesAcute Gastroenteritis With Some DehydrationKiyla920% (1)
- 07 UuDocument7 pages07 UuMela WatiNo ratings yet
- Brief Note On Child HealthDocument6 pagesBrief Note On Child HealthSivakumar Reddy JeevanNo ratings yet
- ARTICLESDocument20 pagesARTICLESJenish Panchal100% (1)
- Plastic Surgery Training in SaudiDocument22 pagesPlastic Surgery Training in SaudiAnonymous 8hVpaQdCtrNo ratings yet
- Tracheal Deviation - Causes and TreatmentDocument5 pagesTracheal Deviation - Causes and TreatmenthaneefmdfNo ratings yet
- GeroDocument7 pagesGeroJehanie LukmanNo ratings yet
- Angina Pectoris: Akshay AgrawalDocument22 pagesAngina Pectoris: Akshay AgrawalBheru LalNo ratings yet
- CT BTDocument20 pagesCT BTZainMalikNo ratings yet
- Common Conversation in Emergency DepartmentDocument3 pagesCommon Conversation in Emergency DepartmentBisturi 2022No ratings yet
- Pakistan Medical & Dental Council (PM&DC) - 1Document32 pagesPakistan Medical & Dental Council (PM&DC) - 1Cricket LoverNo ratings yet
- November 2008 NLE Practice VDocument19 pagesNovember 2008 NLE Practice VEJ Cubero, R☤N100% (2)
- Autism DyslexiaDocument2 pagesAutism DyslexiaAutismDyslexiaNo ratings yet
- Argumentative EssayDocument3 pagesArgumentative EssaypurpleismNo ratings yet
- 58 60Document28 pages58 60Romina ReidNo ratings yet
- Hpia Version 6.0 PDFDocument48 pagesHpia Version 6.0 PDFAl- ImanuddinNo ratings yet
- Kelompok 1Document22 pagesKelompok 1teguhNo ratings yet
- Guidelines For Field Triage of Injured PatientsDocument43 pagesGuidelines For Field Triage of Injured PatientsAlberto J. Rodríguez SolerNo ratings yet
- Clin Infect Dis. 2015 Pappas Cid Civ933Document50 pagesClin Infect Dis. 2015 Pappas Cid Civ933Panos ZarogoulidisNo ratings yet
- Cleft Lip and PalateDocument4 pagesCleft Lip and PalateAnonymous aXExak6u100% (1)
- Laser Treatment Postacne Scars1Document14 pagesLaser Treatment Postacne Scars1Stanca NicolaeNo ratings yet
- Shalonda Wright: Professional ExperienceDocument2 pagesShalonda Wright: Professional Experienceapi-242764074No ratings yet
- Sample Professional CV.Document8 pagesSample Professional CV.HussanAliNo ratings yet
- Acetazolamide/diamoxDocument3 pagesAcetazolamide/diamoxjedisay1100% (1)