
5675932
5675932
You might also like
- Musculoskeletal Cancer Surgery PDFDocument592 pagesMusculoskeletal Cancer Surgery PDFAdolfoBreaAndrade100% (2)
- Principles of Geriatric Physiotherapy-CDDocument194 pagesPrinciples of Geriatric Physiotherapy-CDkrissh2083% (12)
- Nursing Care Plan - FractureDocument2 pagesNursing Care Plan - Fracturederic95% (20)
- Anesthesia For Open Abdominal Aortic SurgeryDocument18 pagesAnesthesia For Open Abdominal Aortic SurgeryAurora TrifaNo ratings yet
- A Rare Case of Pyruvate Kinase Deficiency: Presenter: Dr. Harshal WaghDocument32 pagesA Rare Case of Pyruvate Kinase Deficiency: Presenter: Dr. Harshal WaghDrShefali MhatreNo ratings yet
- GlycogenolysisDocument37 pagesGlycogenolysisJasmine Rey QuintoNo ratings yet
- AKI in SepsisDocument45 pagesAKI in SepsisIkeBundaAdellulaNo ratings yet
- Approach To Pale ChildDocument37 pagesApproach To Pale ChildsangheetaNo ratings yet
- 1885 2Document73 pages1885 2JuhiJahan AmanullahNo ratings yet
- Pathophysiology Notes 1-4Document24 pagesPathophysiology Notes 1-4Scotty Banks100% (3)
- Fractura de StresDocument12 pagesFractura de StresGheorghe SebokNo ratings yet
- Mr. Skeleton PDFDocument6 pagesMr. Skeleton PDFniaNo ratings yet
- Hormonal Control of Calcium and Phosphate MetabolismDocument50 pagesHormonal Control of Calcium and Phosphate MetabolismhamidNo ratings yet
- Fluid Therapy and ElectroliteDocument36 pagesFluid Therapy and ElectroliteAriefBudimanHidayatNo ratings yet
- Clinical EnzymologyDocument25 pagesClinical Enzymologyaminata6No ratings yet
- Acid-Base Homeostasis: Dr. Abeer KhurshidDocument42 pagesAcid-Base Homeostasis: Dr. Abeer Khurshidسلة فواكة100% (2)
- Pregnancy in Women With Congenital Heart DiseaseDocument24 pagesPregnancy in Women With Congenital Heart DiseaseGian Alvarado100% (1)
- Anaesthesia For Endovascular Surgery (Tevar and EvarDocument18 pagesAnaesthesia For Endovascular Surgery (Tevar and EvaranaeshklNo ratings yet
- ABG AnalysisDocument21 pagesABG Analysismrs_jrufusNo ratings yet
- Hypocalcemia & HypercalcemiaDocument21 pagesHypocalcemia & HypercalcemiaRomMy WiEn MicKhoNo ratings yet
- Disorder of Potassium MetabolismDocument28 pagesDisorder of Potassium MetabolismSaif AliNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Acid-Base BalanceDocument28 pagesAcid-Base Balanceps4only100% (1)
- Clinical Approach To Metabolic Bone DiseaseDocument12 pagesClinical Approach To Metabolic Bone DiseaseRamez Nagi NicolaNo ratings yet
- BilirubinDocument40 pagesBilirubinAnisetiyowatiNo ratings yet
- Fluid and Electrolyte Therapy - SeblewongelDocument47 pagesFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeNo ratings yet
- LipidsDocument13 pagesLipidsalianaNo ratings yet
- Paeds Case - Ketotic HypoglycaemiaDocument29 pagesPaeds Case - Ketotic HypoglycaemiaDuncan89No ratings yet
- HaematinicsDocument20 pagesHaematinicsGeetika Mehta100% (1)
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- Cardiac Disease in PregnancyDocument19 pagesCardiac Disease in PregnancyCarolina Orjuela Camargo0% (1)
- Birth AsphyxiaDocument16 pagesBirth Asphyxianurul nabillaNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Diabetic Ketoacidosis in PaediatricDocument11 pagesDiabetic Ketoacidosis in PaediatricSana Anam JahanNo ratings yet
- KIDNEY INJURY/Renal Failure: Acute & Chronic: Prof Sampson Antwi Paediatric Nephrologist Sms-Knust/Kath October 2018Document84 pagesKIDNEY INJURY/Renal Failure: Acute & Chronic: Prof Sampson Antwi Paediatric Nephrologist Sms-Knust/Kath October 2018Effah FestusNo ratings yet
- Thompson Score For HIEDocument2 pagesThompson Score For HIEAnantaBenvenuto100% (1)
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- INSULINDocument54 pagesINSULINBalai Pom PaluNo ratings yet
- Approach To Viral Hepatitis andDocument38 pagesApproach To Viral Hepatitis andVijay ShankarNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- 2012-Fluid and ElectrolytesDocument192 pages2012-Fluid and ElectrolytesHarley Justiniani Dela CruzNo ratings yet
- Hyponatremia in Children 03.19.2010Document23 pagesHyponatremia in Children 03.19.2010Emily EresumaNo ratings yet
- Warfarin Therapy Management: ScopeDocument9 pagesWarfarin Therapy Management: ScopesastiraNo ratings yet
- Heart Disease in Pregnancy FinalDocument24 pagesHeart Disease in Pregnancy FinalBhawna JoshiNo ratings yet
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- 12 Neonatal Hypocalcemia, Glycemia and MagnesemiaDocument55 pages12 Neonatal Hypocalcemia, Glycemia and MagnesemiaRana Vandana100% (1)
- Approach To ProteinuriaDocument14 pagesApproach To ProteinuriaRishi ShresthaNo ratings yet
- DiabetesDocument10 pagesDiabetesLyNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 pagesNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaNo ratings yet
- Amino Acid Metabolism DisordersDocument61 pagesAmino Acid Metabolism DisordersNikitha RafeekNo ratings yet
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
- AnaemiaDocument71 pagesAnaemiaREETHUNo ratings yet
- Diabetic KetoacidosisDocument27 pagesDiabetic Ketoacidosisjun sianNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- Alagille Syndrome FinalDocument54 pagesAlagille Syndrome FinalAlabi Victor Olukayode100% (1)
- HypocalcemiaDocument23 pagesHypocalcemiarayrrn00No ratings yet
- Calcium and PhosphorusDocument34 pagesCalcium and Phosphorus075 Keerthighaa SNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Guidelines For Management of Diabetes MellitusDocument1 pageGuidelines For Management of Diabetes MellitusthapanNo ratings yet
- FLUIDS AND ELECTROLYTES MNGTDocument44 pagesFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Sepsis PowerPointDocument49 pagesSepsis PowerPointWonyenghitari GeorgeNo ratings yet
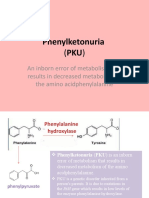
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Endocrine Emergencies in The ICUDocument47 pagesEndocrine Emergencies in The ICUchadchimaNo ratings yet
- Case Presentation: Andreas Crede EM RegistrarDocument15 pagesCase Presentation: Andreas Crede EM RegistrarHeru WahyudiNo ratings yet
- Calicum MetabolismDocument7 pagesCalicum MetabolismDr-Dalya ShakirNo ratings yet
- Metab Ca - PDocument130 pagesMetab Ca - PAndres ValdiviaNo ratings yet
- Lymphatic Research and BiologyDocument6 pagesLymphatic Research and BiologyJuhiJahan AmanullahNo ratings yet
- Bone Tissue24Document79 pagesBone Tissue24JuhiJahan AmanullahNo ratings yet
- Coleman 2Document43 pagesColeman 2JuhiJahan AmanullahNo ratings yet
- Diseasesofboneandhistology 141211233452 Conversion Gate01Document218 pagesDiseasesofboneandhistology 141211233452 Conversion Gate01JuhiJahan AmanullahNo ratings yet
- For The Candidates Admitted From The Academic Year 2013-2014 OnwardsDocument3 pagesFor The Candidates Admitted From The Academic Year 2013-2014 OnwardsJuhiJahan AmanullahNo ratings yet
- March 1990Document11 pagesMarch 1990JuhiJahan AmanullahNo ratings yet
- April 2001Document9 pagesApril 2001JuhiJahan AmanullahNo ratings yet
- Oral Uleration: Thilanka Umesh SugathadasaDocument37 pagesOral Uleration: Thilanka Umesh SugathadasaJuhiJahan AmanullahNo ratings yet
- GPCR 160211124029Document83 pagesGPCR 160211124029JuhiJahan AmanullahNo ratings yet
- Fibrous Dysplasia: A ReviewDocument5 pagesFibrous Dysplasia: A ReviewJuhiJahan AmanullahNo ratings yet
- Usd & MriDocument9 pagesUsd & MriJuhiJahan AmanullahNo ratings yet
- Lester W BurketDocument5 pagesLester W BurketJuhiJahan AmanullahNo ratings yet
- Bli Oumi 2014Document8 pagesBli Oumi 2014JuhiJahan AmanullahNo ratings yet
- Hormonal Regulation of Calcium and Phosphate MetabolismDocument11 pagesHormonal Regulation of Calcium and Phosphate MetabolismpuchioNo ratings yet
- TeriparatideDocument14 pagesTeriparatidecozcozNo ratings yet
- Scientific ArticleDocument260 pagesScientific ArticleDeian MiloieviciNo ratings yet
- Microfracture and Microfracture PlusDocument7 pagesMicrofracture and Microfracture PlusdrjorgewtorresNo ratings yet
- 1.1 Theories of Growth ControlDocument57 pages1.1 Theories of Growth Controlmegha100% (1)
- Adductor-Related Groin Pain Rehab & Return To Sport Progressions With Andrew Wallis HandoutDocument46 pagesAdductor-Related Groin Pain Rehab & Return To Sport Progressions With Andrew Wallis Handoutgemichan26100% (1)
- Course Plan Agreement Anatomy and Physiology (MC-1) : Nueva Ecija University of Science and TechnologyDocument8 pagesCourse Plan Agreement Anatomy and Physiology (MC-1) : Nueva Ecija University of Science and TechnologyMelanie ManuzonNo ratings yet
- What Is The Ewing Family of Tumors?Document43 pagesWhat Is The Ewing Family of Tumors?rantiayefNo ratings yet
- Xray of Bones in OsteomyelitisDocument35 pagesXray of Bones in OsteomyelitisBukola AjokeNo ratings yet
- 8 - DexaDocument26 pages8 - DexascepanNo ratings yet
- Chapter 6 Content Review Questions 1-8Document3 pagesChapter 6 Content Review Questions 1-8Rhonique MorganNo ratings yet
- (P) Behrensmeyer, A. (1978) - Taphonomic and Ecologic Information From Bone WeatheringDocument14 pages(P) Behrensmeyer, A. (1978) - Taphonomic and Ecologic Information From Bone WeatheringSara BrauerNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Plant and Animal TissuesDocument57 pagesPlant and Animal Tissuesclashofclans.suhail3.0No ratings yet
- Janoras, DM (Tissue Mind Map)Document1 pageJanoras, DM (Tissue Mind Map)maxine janorasNo ratings yet
- Fascial Distortion Model (Todd Capistrant Georg Harrer)Document248 pagesFascial Distortion Model (Todd Capistrant Georg Harrer)Katerine Lizeth Alvarez GonzalezNo ratings yet
- Connective Tissue: Dr. Jan Tambayong, PHK Histologi FK-UPHDocument51 pagesConnective Tissue: Dr. Jan Tambayong, PHK Histologi FK-UPHJoshua ObrienNo ratings yet
- My Visit To A Jain Dairy FarmDocument10 pagesMy Visit To A Jain Dairy FarmSant Mat100% (2)
- Intracellular AccumulationsDocument19 pagesIntracellular AccumulationsWajiha106No ratings yet
- Description: SKELETAL SYSTEM-General InformationDocument7 pagesDescription: SKELETAL SYSTEM-General InformationJessica PalacioNo ratings yet
- Biomechanical Implant Fixation of Cocrmo Coating Inferior To Titanium Coating in A Canine Implant ModelDocument7 pagesBiomechanical Implant Fixation of Cocrmo Coating Inferior To Titanium Coating in A Canine Implant ModelAndrew SmithNo ratings yet
- Tov Implant CatalogDocument24 pagesTov Implant CatalogMykolas LukoševičiusNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Basic Elements of A Medical WordDocument92 pagesBasic Elements of A Medical WordJelena Markota100% (1)






































































































Download as ppt, pdf, or txt
You might also like
- Musculoskeletal Cancer Surgery PDFDocument592 pagesMusculoskeletal Cancer Surgery PDFAdolfoBreaAndrade100% (2)
- Principles of Geriatric Physiotherapy-CDDocument194 pagesPrinciples of Geriatric Physiotherapy-CDkrissh2083% (12)
- Nursing Care Plan - FractureDocument2 pagesNursing Care Plan - Fracturederic95% (20)
- Anesthesia For Open Abdominal Aortic SurgeryDocument18 pagesAnesthesia For Open Abdominal Aortic SurgeryAurora TrifaNo ratings yet
- A Rare Case of Pyruvate Kinase Deficiency: Presenter: Dr. Harshal WaghDocument32 pagesA Rare Case of Pyruvate Kinase Deficiency: Presenter: Dr. Harshal WaghDrShefali MhatreNo ratings yet
- GlycogenolysisDocument37 pagesGlycogenolysisJasmine Rey QuintoNo ratings yet
- AKI in SepsisDocument45 pagesAKI in SepsisIkeBundaAdellulaNo ratings yet
- Approach To Pale ChildDocument37 pagesApproach To Pale ChildsangheetaNo ratings yet
- 1885 2Document73 pages1885 2JuhiJahan AmanullahNo ratings yet
- Pathophysiology Notes 1-4Document24 pagesPathophysiology Notes 1-4Scotty Banks100% (3)
- Fractura de StresDocument12 pagesFractura de StresGheorghe SebokNo ratings yet
- Mr. Skeleton PDFDocument6 pagesMr. Skeleton PDFniaNo ratings yet
- Hormonal Control of Calcium and Phosphate MetabolismDocument50 pagesHormonal Control of Calcium and Phosphate MetabolismhamidNo ratings yet
- Fluid Therapy and ElectroliteDocument36 pagesFluid Therapy and ElectroliteAriefBudimanHidayatNo ratings yet
- Clinical EnzymologyDocument25 pagesClinical Enzymologyaminata6No ratings yet
- Acid-Base Homeostasis: Dr. Abeer KhurshidDocument42 pagesAcid-Base Homeostasis: Dr. Abeer Khurshidسلة فواكة100% (2)
- Pregnancy in Women With Congenital Heart DiseaseDocument24 pagesPregnancy in Women With Congenital Heart DiseaseGian Alvarado100% (1)
- Anaesthesia For Endovascular Surgery (Tevar and EvarDocument18 pagesAnaesthesia For Endovascular Surgery (Tevar and EvaranaeshklNo ratings yet
- ABG AnalysisDocument21 pagesABG Analysismrs_jrufusNo ratings yet
- Hypocalcemia & HypercalcemiaDocument21 pagesHypocalcemia & HypercalcemiaRomMy WiEn MicKhoNo ratings yet
- Disorder of Potassium MetabolismDocument28 pagesDisorder of Potassium MetabolismSaif AliNo ratings yet
- ENDO... ElectrolyteDocument44 pagesENDO... ElectrolyteOmar AbdillahiNo ratings yet
- Acid-Base BalanceDocument28 pagesAcid-Base Balanceps4only100% (1)
- Clinical Approach To Metabolic Bone DiseaseDocument12 pagesClinical Approach To Metabolic Bone DiseaseRamez Nagi NicolaNo ratings yet
- BilirubinDocument40 pagesBilirubinAnisetiyowatiNo ratings yet
- Fluid and Electrolyte Therapy - SeblewongelDocument47 pagesFluid and Electrolyte Therapy - SeblewongelSeblewongel AsemeNo ratings yet
- LipidsDocument13 pagesLipidsalianaNo ratings yet
- Paeds Case - Ketotic HypoglycaemiaDocument29 pagesPaeds Case - Ketotic HypoglycaemiaDuncan89No ratings yet
- HaematinicsDocument20 pagesHaematinicsGeetika Mehta100% (1)
- Abg PPT NewDocument69 pagesAbg PPT NewMalaka Atapattu100% (3)
- Cardiac Disease in PregnancyDocument19 pagesCardiac Disease in PregnancyCarolina Orjuela Camargo0% (1)
- Birth AsphyxiaDocument16 pagesBirth Asphyxianurul nabillaNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Diabetic Ketoacidosis in PaediatricDocument11 pagesDiabetic Ketoacidosis in PaediatricSana Anam JahanNo ratings yet
- KIDNEY INJURY/Renal Failure: Acute & Chronic: Prof Sampson Antwi Paediatric Nephrologist Sms-Knust/Kath October 2018Document84 pagesKIDNEY INJURY/Renal Failure: Acute & Chronic: Prof Sampson Antwi Paediatric Nephrologist Sms-Knust/Kath October 2018Effah FestusNo ratings yet
- Thompson Score For HIEDocument2 pagesThompson Score For HIEAnantaBenvenuto100% (1)
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- INSULINDocument54 pagesINSULINBalai Pom PaluNo ratings yet
- Approach To Viral Hepatitis andDocument38 pagesApproach To Viral Hepatitis andVijay ShankarNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- 2012-Fluid and ElectrolytesDocument192 pages2012-Fluid and ElectrolytesHarley Justiniani Dela CruzNo ratings yet
- Hyponatremia in Children 03.19.2010Document23 pagesHyponatremia in Children 03.19.2010Emily EresumaNo ratings yet
- Warfarin Therapy Management: ScopeDocument9 pagesWarfarin Therapy Management: ScopesastiraNo ratings yet
- Heart Disease in Pregnancy FinalDocument24 pagesHeart Disease in Pregnancy FinalBhawna JoshiNo ratings yet
- Final GIT Case PresentationDocument53 pagesFinal GIT Case PresentationRovan100% (1)
- 12 Neonatal Hypocalcemia, Glycemia and MagnesemiaDocument55 pages12 Neonatal Hypocalcemia, Glycemia and MagnesemiaRana Vandana100% (1)
- Approach To ProteinuriaDocument14 pagesApproach To ProteinuriaRishi ShresthaNo ratings yet
- DiabetesDocument10 pagesDiabetesLyNo ratings yet
- Anti Epileptic DrugsDocument89 pagesAnti Epileptic DrugsInderjeet SohalNo ratings yet
- Nonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Document32 pagesNonalcoholic Fatty Liver Disease (NAFLD) : Where Are We Today?Saad MotawéaNo ratings yet
- Amino Acid Metabolism DisordersDocument61 pagesAmino Acid Metabolism DisordersNikitha RafeekNo ratings yet
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
- AnaemiaDocument71 pagesAnaemiaREETHUNo ratings yet
- Diabetic KetoacidosisDocument27 pagesDiabetic Ketoacidosisjun sianNo ratings yet
- Intravenous Fluid Therapy For 2nd Year ConceptDocument83 pagesIntravenous Fluid Therapy For 2nd Year ConceptMay Chelle ErazoNo ratings yet
- Alagille Syndrome FinalDocument54 pagesAlagille Syndrome FinalAlabi Victor Olukayode100% (1)
- HypocalcemiaDocument23 pagesHypocalcemiarayrrn00No ratings yet
- Calcium and PhosphorusDocument34 pagesCalcium and Phosphorus075 Keerthighaa SNo ratings yet
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Guidelines For Management of Diabetes MellitusDocument1 pageGuidelines For Management of Diabetes MellitusthapanNo ratings yet
- FLUIDS AND ELECTROLYTES MNGTDocument44 pagesFLUIDS AND ELECTROLYTES MNGTremerose100% (1)
- Sepsis PowerPointDocument49 pagesSepsis PowerPointWonyenghitari GeorgeNo ratings yet
- Phenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino AcidphenylalanineDocument8 pagesPhenylketonuria: An Inborn Error of Metabolism That Results in Decreased Metabolism of The Amino Acidphenylalanineელენე ბუჩუკურიNo ratings yet
- Endocrine Emergencies in The ICUDocument47 pagesEndocrine Emergencies in The ICUchadchimaNo ratings yet
- Case Presentation: Andreas Crede EM RegistrarDocument15 pagesCase Presentation: Andreas Crede EM RegistrarHeru WahyudiNo ratings yet
- Calicum MetabolismDocument7 pagesCalicum MetabolismDr-Dalya ShakirNo ratings yet
- Metab Ca - PDocument130 pagesMetab Ca - PAndres ValdiviaNo ratings yet
- Lymphatic Research and BiologyDocument6 pagesLymphatic Research and BiologyJuhiJahan AmanullahNo ratings yet
- Bone Tissue24Document79 pagesBone Tissue24JuhiJahan AmanullahNo ratings yet
- Coleman 2Document43 pagesColeman 2JuhiJahan AmanullahNo ratings yet
- Diseasesofboneandhistology 141211233452 Conversion Gate01Document218 pagesDiseasesofboneandhistology 141211233452 Conversion Gate01JuhiJahan AmanullahNo ratings yet
- For The Candidates Admitted From The Academic Year 2013-2014 OnwardsDocument3 pagesFor The Candidates Admitted From The Academic Year 2013-2014 OnwardsJuhiJahan AmanullahNo ratings yet
- March 1990Document11 pagesMarch 1990JuhiJahan AmanullahNo ratings yet
- April 2001Document9 pagesApril 2001JuhiJahan AmanullahNo ratings yet
- Oral Uleration: Thilanka Umesh SugathadasaDocument37 pagesOral Uleration: Thilanka Umesh SugathadasaJuhiJahan AmanullahNo ratings yet
- GPCR 160211124029Document83 pagesGPCR 160211124029JuhiJahan AmanullahNo ratings yet
- Fibrous Dysplasia: A ReviewDocument5 pagesFibrous Dysplasia: A ReviewJuhiJahan AmanullahNo ratings yet
- Usd & MriDocument9 pagesUsd & MriJuhiJahan AmanullahNo ratings yet
- Lester W BurketDocument5 pagesLester W BurketJuhiJahan AmanullahNo ratings yet
- Bli Oumi 2014Document8 pagesBli Oumi 2014JuhiJahan AmanullahNo ratings yet
- Hormonal Regulation of Calcium and Phosphate MetabolismDocument11 pagesHormonal Regulation of Calcium and Phosphate MetabolismpuchioNo ratings yet
- TeriparatideDocument14 pagesTeriparatidecozcozNo ratings yet
- Scientific ArticleDocument260 pagesScientific ArticleDeian MiloieviciNo ratings yet
- Microfracture and Microfracture PlusDocument7 pagesMicrofracture and Microfracture PlusdrjorgewtorresNo ratings yet
- 1.1 Theories of Growth ControlDocument57 pages1.1 Theories of Growth Controlmegha100% (1)
- Adductor-Related Groin Pain Rehab & Return To Sport Progressions With Andrew Wallis HandoutDocument46 pagesAdductor-Related Groin Pain Rehab & Return To Sport Progressions With Andrew Wallis Handoutgemichan26100% (1)
- Course Plan Agreement Anatomy and Physiology (MC-1) : Nueva Ecija University of Science and TechnologyDocument8 pagesCourse Plan Agreement Anatomy and Physiology (MC-1) : Nueva Ecija University of Science and TechnologyMelanie ManuzonNo ratings yet
- What Is The Ewing Family of Tumors?Document43 pagesWhat Is The Ewing Family of Tumors?rantiayefNo ratings yet
- Xray of Bones in OsteomyelitisDocument35 pagesXray of Bones in OsteomyelitisBukola AjokeNo ratings yet
- 8 - DexaDocument26 pages8 - DexascepanNo ratings yet
- Chapter 6 Content Review Questions 1-8Document3 pagesChapter 6 Content Review Questions 1-8Rhonique MorganNo ratings yet
- (P) Behrensmeyer, A. (1978) - Taphonomic and Ecologic Information From Bone WeatheringDocument14 pages(P) Behrensmeyer, A. (1978) - Taphonomic and Ecologic Information From Bone WeatheringSara BrauerNo ratings yet
- Medical Surgical Nursing OrthopedicDocument22 pagesMedical Surgical Nursing Orthopedicroger80% (5)
- Plant and Animal TissuesDocument57 pagesPlant and Animal Tissuesclashofclans.suhail3.0No ratings yet
- Janoras, DM (Tissue Mind Map)Document1 pageJanoras, DM (Tissue Mind Map)maxine janorasNo ratings yet
- Fascial Distortion Model (Todd Capistrant Georg Harrer)Document248 pagesFascial Distortion Model (Todd Capistrant Georg Harrer)Katerine Lizeth Alvarez GonzalezNo ratings yet
- Connective Tissue: Dr. Jan Tambayong, PHK Histologi FK-UPHDocument51 pagesConnective Tissue: Dr. Jan Tambayong, PHK Histologi FK-UPHJoshua ObrienNo ratings yet
- My Visit To A Jain Dairy FarmDocument10 pagesMy Visit To A Jain Dairy FarmSant Mat100% (2)
- Intracellular AccumulationsDocument19 pagesIntracellular AccumulationsWajiha106No ratings yet
- Description: SKELETAL SYSTEM-General InformationDocument7 pagesDescription: SKELETAL SYSTEM-General InformationJessica PalacioNo ratings yet
- Biomechanical Implant Fixation of Cocrmo Coating Inferior To Titanium Coating in A Canine Implant ModelDocument7 pagesBiomechanical Implant Fixation of Cocrmo Coating Inferior To Titanium Coating in A Canine Implant ModelAndrew SmithNo ratings yet
- Tov Implant CatalogDocument24 pagesTov Implant CatalogMykolas LukoševičiusNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Basic Elements of A Medical WordDocument92 pagesBasic Elements of A Medical WordJelena Markota100% (1)