Download as pptx, pdf, or txt
You might also like
- Child Health Nursing: Unit-V Nursing Management in Common Childhood Disorders Communicable Diseases in ChildhoodDocument41 pagesChild Health Nursing: Unit-V Nursing Management in Common Childhood Disorders Communicable Diseases in ChildhoodEllen AngelNo ratings yet
- MeaslesDocument20 pagesMeaslesTinde KumarNo ratings yet
- MeaslesDocument33 pagesMeaslesObi EmereuwaNo ratings yet
- 33a. Rickettsial, Coxiella & BatonellaDocument41 pages33a. Rickettsial, Coxiella & Batonellaalicerugaibula123No ratings yet
- MeaslesDocument58 pagesMeaslesDr.P.NatarajanNo ratings yet
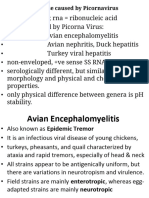
- PICORNAVIRUSDocument20 pagesPICORNAVIRUStejasbhukal567No ratings yet
- Paediatric Rashes: Ali Faisal SaleemDocument51 pagesPaediatric Rashes: Ali Faisal Saleemarjumand100% (3)
- Public Health Officers C1: TetanusDocument64 pagesPublic Health Officers C1: Tetanusmamaru bantieNo ratings yet
- DudeDocument38 pagesDudeGustavo VasquezNo ratings yet
- Basic Information RabiesDocument32 pagesBasic Information RabiesdrkhalidfcpsNo ratings yet
- Viral Infections Part 1 by Nicolle Ann Pancho (Pediatrics Rotation)Document67 pagesViral Infections Part 1 by Nicolle Ann Pancho (Pediatrics Rotation)Nicolle PanchoNo ratings yet
- Fever and RashDocument120 pagesFever and RashsamaNo ratings yet
- 1-Measles (Rubeola) PDFDocument37 pages1-Measles (Rubeola) PDFمصطفى رسول هاديNo ratings yet
- Leptospirosis UPH 2Document33 pagesLeptospirosis UPH 2Joshua ObrienNo ratings yet
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- BrucellosisDocument38 pagesBrucellosisEslam HamadaNo ratings yet
- LeptospirosisDocument40 pagesLeptospirosistummalapalli venkateswara rao86% (7)
- DPT Hib 2015Document42 pagesDPT Hib 2015Hannan AliNo ratings yet
- Anthrax Infction and BruccellaDocument46 pagesAnthrax Infction and BruccellaRohan TejaNo ratings yet
- Viral Gastroenteritis: Submitted byDocument20 pagesViral Gastroenteritis: Submitted byRavi PrakashNo ratings yet
- Case Presentation-ChickenpoxDocument41 pagesCase Presentation-ChickenpoxShalini100% (1)
- Leptospirosis Smt7Document34 pagesLeptospirosis Smt7hendra_darmawan_4No ratings yet
- Herpes, Pox, Rhabdo, Arena VIRUSDocument7 pagesHerpes, Pox, Rhabdo, Arena VIRUSErnie G. Bautista II, RN, MDNo ratings yet
- DIPHTHERIADocument12 pagesDIPHTHERIANununNo ratings yet
- MMR лекцияDocument37 pagesMMR лекцияsaurabhdhakedgNo ratings yet
- Communicable Disease (MMR) (Autosaved)Document65 pagesCommunicable Disease (MMR) (Autosaved)Ellen AngelNo ratings yet
- SGD Case Presentation 8Document34 pagesSGD Case Presentation 8Karen C. Del Rosario100% (1)
- Opportunistic Parasitic InfectionsDocument57 pagesOpportunistic Parasitic Infectionstummalapalli venkateswara raoNo ratings yet
- Zoonoses and Arthropod-Borne Diseases - AyaDocument22 pagesZoonoses and Arthropod-Borne Diseases - Aya180045No ratings yet
- Viral Infections of The GI SystemDocument76 pagesViral Infections of The GI SystemKer YehunNo ratings yet
- Communicable DisesaseDocument111 pagesCommunicable Disesasebrillaboy266No ratings yet
- Virus PDFDocument60 pagesVirus PDFrenz bartolomeNo ratings yet
- Lepto Dan RabiesDocument69 pagesLepto Dan RabiesHiszom AsyhariNo ratings yet
- Enteric Fever in NepalDocument51 pagesEnteric Fever in NepalBinayaNo ratings yet
- Rubella Virus: Upendo Kibwana Microbiology and Immunology Department MuhasDocument13 pagesRubella Virus: Upendo Kibwana Microbiology and Immunology Department MuhasMusa yohanaNo ratings yet
- What Is Anthropod and Vector Borne Disease What Is Anthropod and Vector Borne DiseaseDocument59 pagesWhat Is Anthropod and Vector Borne Disease What Is Anthropod and Vector Borne DiseaseNessa Layos MorilloNo ratings yet
- Protozoal InfectionDocument66 pagesProtozoal InfectionGEM SCANNo ratings yet
- Respiratory Infections: - Small Pox - Chicken Pox - TuberculosisDocument45 pagesRespiratory Infections: - Small Pox - Chicken Pox - TuberculosisNamrata SharmaNo ratings yet
- Varicella (Chickenpox) Disease: Chananart Yuakyen: IcnDocument28 pagesVaricella (Chickenpox) Disease: Chananart Yuakyen: IcnKana FajarNo ratings yet
- Small Animal MedicineDocument262 pagesSmall Animal Medicinelijyohannesmekonnen7No ratings yet
- P 1 InfectiousDocument73 pagesP 1 InfectiousHIMANSHU GUPTANo ratings yet
- Infectious OralsDocument164 pagesInfectious OralsHIMANSHU GUPTANo ratings yet
- Monkey PoxDocument29 pagesMonkey PoxMalavika A GNo ratings yet
- DR Anil Sabharwal MDDocument57 pagesDR Anil Sabharwal MDsaump3No ratings yet
- Abdelfattah Monged Selim - Tetanus 2Document25 pagesAbdelfattah Monged Selim - Tetanus 2Saja MaraqaNo ratings yet
- Arboviral Diseases and Dengue FinalDocument73 pagesArboviral Diseases and Dengue FinalBinayaNo ratings yet
- MeaslesDocument8 pagesMeaslesDave ComstockNo ratings yet
- MD PPTDocument105 pagesMD PPTtoxiczarrar.pubgNo ratings yet
- Dengue FeverDocument31 pagesDengue FeverAditya Agarwal100% (1)
- Scrub TyphusDocument18 pagesScrub Typhusashirwad sharma iiNo ratings yet
- Salmonella Infections: (Salmonelloses)Document56 pagesSalmonella Infections: (Salmonelloses)andualemNo ratings yet
- Typhoid Fever: By, Arathy DarvinDocument35 pagesTyphoid Fever: By, Arathy DarvinJaina JoseNo ratings yet
- 3) Typhoid FeverDocument36 pages3) Typhoid FeversmrutuNo ratings yet
- MEASLESDocument26 pagesMEASLESprasanna lamaNo ratings yet
- Monkey Pox-FinalDocument23 pagesMonkey Pox-FinalnirmalaspandagaleNo ratings yet
- Zika and PlagueDocument30 pagesZika and PlagueRupali Verma BaggaNo ratings yet
- Viral InfectionsDocument34 pagesViral InfectionsAlaa MadmoujNo ratings yet
- Microfinance For Sanitation. Indonesia Water Supply and Sanitation Magazine PERCIK July 2005.Document60 pagesMicrofinance For Sanitation. Indonesia Water Supply and Sanitation Magazine PERCIK July 2005.Oswar MungkasaNo ratings yet
- Rothblum, Solomon, Murakami 1986 - Diferencias Cognitivas, Afectivas y Conductuales Entre Procrastinadores Altos y Bajos PDFDocument8 pagesRothblum, Solomon, Murakami 1986 - Diferencias Cognitivas, Afectivas y Conductuales Entre Procrastinadores Altos y Bajos PDFMartin RuízNo ratings yet
- Danfoss VLT2800 Manual PDFDocument124 pagesDanfoss VLT2800 Manual PDFSP Rajput100% (1)
- 15 User ManualDocument3 pages15 User ManualPablo CzNo ratings yet
- Ansulite Afc3B-Fp29 3% Freeze-Protected AFFF Concentrate: DescriptionDocument2 pagesAnsulite Afc3B-Fp29 3% Freeze-Protected AFFF Concentrate: DescriptionDavid CubaNo ratings yet
- Caterpillar C280 Series Engine Product GuideDocument221 pagesCaterpillar C280 Series Engine Product GuideIvan Aditya100% (1)
- Operating Manual: Continuous Band Sealer (Horizontal Orientation) Model No: FR-900SDocument5 pagesOperating Manual: Continuous Band Sealer (Horizontal Orientation) Model No: FR-900SRishi RaghaniNo ratings yet
- Human Resource Management - 1 Prof. Kalyan Chakravarti Department of Basic Courses Indian Institute of Technology, KharagpurDocument35 pagesHuman Resource Management - 1 Prof. Kalyan Chakravarti Department of Basic Courses Indian Institute of Technology, KharagpurIvani KatalNo ratings yet
- Jeppview For Windows: General Information General InformationDocument39 pagesJeppview For Windows: General Information General Informationbooba100% (1)
- Antonin Artaud - Poetry Madness Self-LibreDocument216 pagesAntonin Artaud - Poetry Madness Self-LibreDouglas Hudson100% (5)
- Control Valve Sourcebook (Refining) PDFDocument198 pagesControl Valve Sourcebook (Refining) PDFnaraNJORNo ratings yet
- C DAC Winter Project Report 7 PDFDocument29 pagesC DAC Winter Project Report 7 PDFAbhinav TayadeNo ratings yet
- Compositional SimulationDocument35 pagesCompositional SimulationKellen Sanchez100% (1)
- 100 TOP WATER SUPPLY Engineering Objective Questions and Answers WATER SUPPLY Engineering Mcqs PDFDocument8 pages100 TOP WATER SUPPLY Engineering Objective Questions and Answers WATER SUPPLY Engineering Mcqs PDFMV chandan50% (2)
- CLC 18-10Nb: A NB Stabilized 18Cr-10Ni Austenitic Stainless Steel (347 Grade)Document4 pagesCLC 18-10Nb: A NB Stabilized 18Cr-10Ni Austenitic Stainless Steel (347 Grade)PeterWayNo ratings yet
- Course Syllabus in SuccessionDocument16 pagesCourse Syllabus in SuccessionCharina BalunsoNo ratings yet
- Denward Eng PatriciaDocument2 pagesDenward Eng PatriciaMary Angelica Gabayan LitobNo ratings yet
- Montesano Ness LacartarelacionalenterapiadeparejaDocument23 pagesMontesano Ness LacartarelacionalenterapiadeparejaEncuentros y DiálogosNo ratings yet
- 21-Post-Term Pregnancy and Induction of LabourDocument4 pages21-Post-Term Pregnancy and Induction of LabourAmalNo ratings yet
- Impco 425 CarburetorDocument6 pagesImpco 425 Carburetors_boots100% (2)
- SAMAP 15 ProceedingsDocument84 pagesSAMAP 15 ProceedingsOm Parkash SharmaNo ratings yet
- Universiti Teknologi Mara Final Examination: Confidential AS/MAR2012/PHY310Document9 pagesUniversiti Teknologi Mara Final Examination: Confidential AS/MAR2012/PHY310luminousspaceNo ratings yet
- Biology CH 7 Practice TestDocument6 pagesBiology CH 7 Practice Testvaleria100% (2)
- Click Here For A Video Demonstration: UnresponsivenessDocument3 pagesClick Here For A Video Demonstration: UnresponsivenessJnana YumnaNo ratings yet
- Activity Worksheet 2 T TestDocument1 pageActivity Worksheet 2 T TestKit Augustine TantoyNo ratings yet
- Elements and Problems ICECH11Document13 pagesElements and Problems ICECH11Nobel Engzen Du BermoyNo ratings yet
- Tenp DPT Biochemistry: DR Pius KiptemburDocument13 pagesTenp DPT Biochemistry: DR Pius KiptemburGerald Limo Arap ChebiiNo ratings yet
- Turkish Airlines Inc. A320 / B737 First Officer Minimum RequirementsDocument5 pagesTurkish Airlines Inc. A320 / B737 First Officer Minimum RequirementsLin CYNo ratings yet
- FirmwareUpgradeInstructionsRx3iCPEs v1Document4 pagesFirmwareUpgradeInstructionsRx3iCPEs v1Wilson KnuppNo ratings yet
- Commorbidity (NCP)Document15 pagesCommorbidity (NCP)Stephanie Libo-onNo ratings yet