Download as pptx, pdf, or txt
You might also like
- Curvas Parálisis Cerebral Brooks 2011Document36 pagesCurvas Parálisis Cerebral Brooks 2011veronicaNo ratings yet
- The Black Book of Strength - Andy BoltonDocument49 pagesThe Black Book of Strength - Andy BoltonGawen100% (3)
- Stoma OsceDocument8 pagesStoma OsceRadhiyatul Ashiqeen Binti MoktarNo ratings yet
- Unitor MsdsDocument5 pagesUnitor Msdsvakil50% (2)
- Epid Chapt 1 Measurement of Health and DiseaseDocument63 pagesEpid Chapt 1 Measurement of Health and DiseaseAmanuel Maru100% (1)
- Stoma Management: Shankar ZanwarDocument33 pagesStoma Management: Shankar Zanwarpradeep nair100% (1)
- Intestinal Stomas - AKTDocument49 pagesIntestinal Stomas - AKTTammie YoungNo ratings yet
- StomaDocument37 pagesStomaAndryHarisNo ratings yet
- ColostomyDocument60 pagesColostomymathisync100% (1)
- ColostomyDocument13 pagesColostomyKetali JambhavdekarNo ratings yet
- Anatomy and PhysiologyDocument42 pagesAnatomy and Physiologysushma shresthaNo ratings yet
- ColostomyDocument23 pagesColostomySheene Ainasthazia Diego AngNo ratings yet
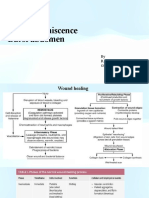
- Wound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V UnitDocument25 pagesWound Dehiscence Burst Abdomen: by R.V.Kalyani Gen Surgery V Unitvinitha kattaNo ratings yet
- StomasDocument4 pagesStomasSaravanan Sridharan100% (1)
- Types and Complication of C-SectionDocument13 pagesTypes and Complication of C-SectionMeghaUnniNo ratings yet
- Diverticular Diseases of ColonDocument22 pagesDiverticular Diseases of ColonGyan Prakash BhartiNo ratings yet
- End Colostomy's: An Overview of The Procedure, Indications, and AftercareDocument15 pagesEnd Colostomy's: An Overview of The Procedure, Indications, and AftercareRichard JohnsonNo ratings yet
- ColonDocument7 pagesColonch3zk4No ratings yet
- Management of Stoma, Cut and WoundsDocument40 pagesManagement of Stoma, Cut and WoundsLalita KumariNo ratings yet
- MastoidectomyDocument110 pagesMastoidectomySangam AdhikariNo ratings yet
- Management of Stomas, Catheters and TubesDocument25 pagesManagement of Stomas, Catheters and TubesElishiba Mire100% (6)
- Burst Abdomen: by DR - SuhaibDocument15 pagesBurst Abdomen: by DR - Suhaibsuhaibrehaman100% (1)
- ColostomyDocument30 pagesColostomyGlen DaleNo ratings yet
- Burstabdomen 151223101029Document24 pagesBurstabdomen 151223101029ArifHidayatNo ratings yet
- Colostomy Closure: How To Avoid Complication: Journal ReadingDocument34 pagesColostomy Closure: How To Avoid Complication: Journal ReadingAndi Rizki CaprianusNo ratings yet
- Meckels DiveritulumDocument30 pagesMeckels DiveritulumFrancis Adrian O. LadoresNo ratings yet
- Study Guide OstomyDocument6 pagesStudy Guide OstomyKennard Aristo ArifinNo ratings yet
- Colostomy Wps OfficeDocument19 pagesColostomy Wps Officehealthseeker159No ratings yet
- ColostomyDocument45 pagesColostomydrqiekiNo ratings yet
- Operative Obstetrics: Madira Emmanuel Lira UniversityDocument27 pagesOperative Obstetrics: Madira Emmanuel Lira Universityvictor onapaNo ratings yet
- Colostomy CareDocument8 pagesColostomy CareAhmed Hamed100% (2)
- Colostomy CareDocument35 pagesColostomy CareRashmita DahalNo ratings yet
- Stoma / OstomyDocument55 pagesStoma / OstomyDPM FK Untar100% (1)
- Maternal Injuries During Vaginal Delivery and Its ManagementDocument51 pagesMaternal Injuries During Vaginal Delivery and Its ManagementJay Seetohul100% (1)
- Colostomy by PHLLPDocument68 pagesColostomy by PHLLPkiyermsangi00No ratings yet
- Stomacolostomy 161108133919Document3 pagesStomacolostomy 161108133919drng48100% (1)
- Intestinal Stomas PDFDocument10 pagesIntestinal Stomas PDFAmyandNo ratings yet
- COLOSTOMYDocument2 pagesCOLOSTOMYjennivelempaynado78No ratings yet
- Reasons For Having An Ileostomy: Surgical Opening Small Intestine Ileum Pouching System Groin AbdomenDocument7 pagesReasons For Having An Ileostomy: Surgical Opening Small Intestine Ileum Pouching System Groin AbdomenContented LinganNo ratings yet
- By Abayneh Ayele (Ieso Student) Wollo UniversityDocument68 pagesBy Abayneh Ayele (Ieso Student) Wollo UniversitydenekeNo ratings yet
- ColostomyDocument2 pagesColostomyFenelie AblazaNo ratings yet
- ColostomyDocument3 pagesColostomyDr. Ikwuakor ChikezieNo ratings yet
- Types and Management of Intestinal StomasDocument62 pagesTypes and Management of Intestinal Stomasminnalesri100% (6)
- Hernia UmbilicalisDocument24 pagesHernia UmbilicalisFajar TriwibawaNo ratings yet
- Stoma ComplicationsDocument35 pagesStoma ComplicationsAlex Ciorogar100% (1)
- Umbilical HerniaDocument15 pagesUmbilical Herniatsega tilahunNo ratings yet
- Suture MaterialsDocument42 pagesSuture MaterialsAmirudin SanipNo ratings yet
- 3.radiation InjDocument9 pages3.radiation Injapi-3829364No ratings yet
- Genital Tract InjuriesDocument23 pagesGenital Tract InjuriesdammmnNo ratings yet
- DIVERTIKULOSISDocument28 pagesDIVERTIKULOSISAndrie WigunaNo ratings yet
- TP3 QX Cadenas ValentinaDocument7 pagesTP3 QX Cadenas ValentinaValen CadenasNo ratings yet
- Updates in Management of Enterocutaneous FistulaDocument35 pagesUpdates in Management of Enterocutaneous Fistulabashiru100% (1)
- Burst AbdomenDocument24 pagesBurst AbdomenKarishma ManghaniNo ratings yet
- Common Abdominal Surgeries: Prof. (DR.) Md. Jawed AktherDocument21 pagesCommon Abdominal Surgeries: Prof. (DR.) Md. Jawed AkthervarunNo ratings yet
- Abdominal StomasDocument3 pagesAbdominal Stomashelangen100% (1)
- Colostomy NayanaDocument15 pagesColostomy NayanaMariam AntonyNo ratings yet
- Colostomy CareDocument35 pagesColostomy CareRoyster CabralNo ratings yet
- Abdominal Wound Dehiscence: DR - Nazmoon Nahar Honorary Medical Officer Surgery Unit IIIDocument18 pagesAbdominal Wound Dehiscence: DR - Nazmoon Nahar Honorary Medical Officer Surgery Unit IIIMashrufNo ratings yet
- EPISIOTOMYDocument9 pagesEPISIOTOMYkailash chand atal100% (1)
- Malignant Growth of Tumor That Begins From The Inner Wall of The Colon or Rectum. Can Also Involve The Anal CanalDocument55 pagesMalignant Growth of Tumor That Begins From The Inner Wall of The Colon or Rectum. Can Also Involve The Anal CanalJojo JustoNo ratings yet
- Which Conditions Can Be Treated? Under Local Anesthesia: The Excision of The Foreskin (Prepuce)Document9 pagesWhich Conditions Can Be Treated? Under Local Anesthesia: The Excision of The Foreskin (Prepuce)John Jose Sy GalauranNo ratings yet
- Intestinal Obstruction AditiDocument67 pagesIntestinal Obstruction Aditiaditi BahugunaNo ratings yet
- The Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingFrom EverandThe Ileoanal Pouch: A Practical Guide for Surgery, Management and TroubleshootingJanindra WarusavitarneNo ratings yet
- Introduction To Medical Surgical NursingDocument42 pagesIntroduction To Medical Surgical NursingAmanuel Maru100% (1)
- Pleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Document61 pagesPleural Disorders: 5/29/2018 1 by Shegaw Z (MSC in Ahn)Amanuel MaruNo ratings yet
- MicrobiologyDocument81 pagesMicrobiologyAmanuel MaruNo ratings yet
- 2 Cholinergic BlockersDocument49 pages2 Cholinergic BlockersAmanuel MaruNo ratings yet
- Laboratory Diagnosis of Parasitic DiseasesDocument57 pagesLaboratory Diagnosis of Parasitic DiseasesAmanuel MaruNo ratings yet
- Health & Human BehaviorDocument56 pagesHealth & Human BehaviorAmanuel Maru100% (2)
- 1.household Water Supply and Basic SanitationDocument8 pages1.household Water Supply and Basic SanitationAmanuel MaruNo ratings yet
- For PC-I Medicine Students By: Zelalem ADocument39 pagesFor PC-I Medicine Students By: Zelalem AAmanuel MaruNo ratings yet
- Revision Resources s4-6Document11 pagesRevision Resources s4-6Amanuel MaruNo ratings yet
- Biochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananDocument80 pagesBiochemistry of Red Blood Cells (Erythrocytes) - : Rajesh.P. NarayananAmanuel MaruNo ratings yet
- Hema II Chapter11 - QA in HematologyDocument29 pagesHema II Chapter11 - QA in HematologyAmanuel MaruNo ratings yet
- Day 4Document55 pagesDay 4Amanuel MaruNo ratings yet
- Renal PhysiologyDocument75 pagesRenal PhysiologyAmanuel Maru100% (1)
- Human Vitamin and Mineral RequirementsDocument303 pagesHuman Vitamin and Mineral RequirementsHector100% (6)
- Li Endocrine GlandsDocument32 pagesLi Endocrine GlandsAmanuel MaruNo ratings yet
- Action of Hormones PDFDocument8 pagesAction of Hormones PDFAmanuel MaruNo ratings yet
- DR - Haroon RashidDocument21 pagesDR - Haroon RashidAmanuel MaruNo ratings yet
- Sede Torre Arequipa Facultad Ingenieria:) Take Photos For A Magazine. He Is A Fashion PhotographerDocument4 pagesSede Torre Arequipa Facultad Ingenieria:) Take Photos For A Magazine. He Is A Fashion PhotographerroosbelNo ratings yet
- Characteristics of Narcissistic MothersDocument11 pagesCharacteristics of Narcissistic Mothersapi-325904642No ratings yet
- Aerial Lift TrainingDocument81 pagesAerial Lift TrainingCesar Augusto Vera JaimesNo ratings yet
- Research PaperDocument8 pagesResearch Paperapi-366464825No ratings yet
- CapstoneDocument27 pagesCapstoneapi-306133503No ratings yet
- Bsiec2019 ResearchDocument28 pagesBsiec2019 ResearchRosendo Dizon NualNo ratings yet
- Detailed System Design: 4.1. Use Case DiagramDocument4 pagesDetailed System Design: 4.1. Use Case DiagramammaraNo ratings yet
- MSDS WMO KaydolDocument8 pagesMSDS WMO Kaydoljaya sukmanaNo ratings yet
- Fitness Tracker Website Mini ProjectDocument9 pagesFitness Tracker Website Mini ProjectSrinAdh YadavNo ratings yet
- Non Members Comments ListDocument16 pagesNon Members Comments ListMostafa Omran100% (1)
- Women's SHG Poverty Alleviation and EmpowermentDocument11 pagesWomen's SHG Poverty Alleviation and EmpowermentRuthi GuiteNo ratings yet
- Laser Patient BrochureDocument2 pagesLaser Patient BrochureMiles Herman FlikkeNo ratings yet
- Post-Traumatic Frontal Mucocele Exceptional Cause and Frequent RecurrenceDocument3 pagesPost-Traumatic Frontal Mucocele Exceptional Cause and Frequent RecurrenceInternational Journal of Innovative Science and Research Technology100% (1)
- Evaluating Surface Cleanliness Using A Risk-Based ApproachDocument16 pagesEvaluating Surface Cleanliness Using A Risk-Based Approachqac gmpNo ratings yet
- Laminine TestimonialsDocument13 pagesLaminine TestimonialsTshnet NetNo ratings yet
- The Preanalytical PhaseDocument24 pagesThe Preanalytical PhaseArturo Eduardo Huarcaya OntiverosNo ratings yet
- Case Lâm SàngDocument39 pagesCase Lâm SàngHungNo ratings yet
- Brochure For MapehDocument4 pagesBrochure For MapehKarl Anthony SuarezNo ratings yet
- Perspective Essay TopicsDocument4 pagesPerspective Essay Topicsb725c62j100% (2)
- BowTieXP What Is A BowTieDocument18 pagesBowTieXP What Is A BowTieJoseph Markham100% (2)
- Model Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentDocument5 pagesModel Test 4 Reading Passage 1 One Hundred Days of Reform: Reformer in Control of The GovernmentphuongthaospkNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- HB1229Document3 pagesHB1229Rob PortNo ratings yet
- Edited PPT HEALTH 4th (Autosaved)Document23 pagesEdited PPT HEALTH 4th (Autosaved)Chloe Belamare JaplitNo ratings yet
- Clinical Evidence Requirements According To The IVDocument8 pagesClinical Evidence Requirements According To The IVDr.Sivakumar SelvarajNo ratings yet
- Dysrhythmia Advance Content Outline A1 - 2020.1.2Document3 pagesDysrhythmia Advance Content Outline A1 - 2020.1.2Kimberly Whiteside50% (2)