Download as ppt, pdf, or txt
You might also like
- 2 Acute Rheumatic FeverDocument28 pages2 Acute Rheumatic FeverDammaqsaa W BiyyanaaNo ratings yet
- Acquired Heart Disease in PediatricsDocument130 pagesAcquired Heart Disease in Pediatricsณัช เกษมNo ratings yet
- Test Questions For A Lecture On Acute Rheumatic FeverDocument6 pagesTest Questions For A Lecture On Acute Rheumatic FeverFiona CoutinhoNo ratings yet
- Valvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityDocument46 pagesValvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityChacha TasyaNo ratings yet
- Acute Rheumatic FeverDocument51 pagesAcute Rheumatic FeverFaedil Ichsan CiremaiNo ratings yet
- Rheumatic FeverDocument21 pagesRheumatic FeverUmar Azlan50% (2)
- Rheumatic HeartDocument47 pagesRheumatic HeartsmrutuNo ratings yet
- Rheumatic Fever: DR: Kaem Shir AliDocument24 pagesRheumatic Fever: DR: Kaem Shir AliMwanja Moses100% (1)
- Rheumatic Fever and Heart DiseaseDocument37 pagesRheumatic Fever and Heart Diseasejiregna eticha dakoNo ratings yet
- Rheumatic Heart DiseaseDocument39 pagesRheumatic Heart DiseaseSamarjeet KaurNo ratings yet
- Rheumatic FeverDocument39 pagesRheumatic FeverDharaneedhar AdepuNo ratings yet
- Rheumatic-FeverDocument35 pagesRheumatic-FeverHasan Diab0% (2)
- ARF PresentationDocument39 pagesARF PresentationRichard SsenyondoNo ratings yet
- Rheumatic Heart DiseaseDocument37 pagesRheumatic Heart Diseasesalman hNo ratings yet
- Rheumatic Heart DiseaseDocument22 pagesRheumatic Heart DiseasemajdNo ratings yet
- The Prevention of Rheumatic Fever and Rheumatic Heart DiseaseDocument56 pagesThe Prevention of Rheumatic Fever and Rheumatic Heart DiseaseSameer KulkarniNo ratings yet
- Rheumatc Heart: DiseaseDocument29 pagesRheumatc Heart: DiseaseMohamed BamashmoosNo ratings yet
- Rheumatic Heart Disease Msc23Document65 pagesRheumatic Heart Disease Msc23Manaswi DebbermaNo ratings yet
- Rheumatic Heart DiseaseDocument5 pagesRheumatic Heart DiseasejessyNo ratings yet
- Rheumatic Heart DiseaseDocument21 pagesRheumatic Heart Diseasemedzmedina2No ratings yet
- KawasakiDocument28 pagesKawasakiLaith DmourNo ratings yet
- Pediatric Cardiology: Ruby Ann L. Punongbayan, MDDocument51 pagesPediatric Cardiology: Ruby Ann L. Punongbayan, MDsarguss14100% (3)
- Pericardial DiseaseDocument59 pagesPericardial DiseaseGunawan Yoga100% (1)
- Heart Disease Complicating PregnancyDocument169 pagesHeart Disease Complicating PregnancyRajeev Sood100% (2)
- Presented By,: A.Priyadharshini M.SC (N) Lecturer, Dept - of Paediatrics, Jai Institute of Nursing A N D Research, GwaliorDocument24 pagesPresented By,: A.Priyadharshini M.SC (N) Lecturer, Dept - of Paediatrics, Jai Institute of Nursing A N D Research, GwaliorPrince MahyavanshiNo ratings yet
- Acute Rheumatic FeverDocument20 pagesAcute Rheumatic Feverfaizal samadNo ratings yet
- Acute Rheumatic Fever and Rheumatic Heart Disease: Ria NovaDocument36 pagesAcute Rheumatic Fever and Rheumatic Heart Disease: Ria NovaaisyahNo ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseaseABREHAM BUKULONo ratings yet
- 21 - Pericardial DiseasesDocument50 pages21 - Pericardial DiseasesMariana CabralNo ratings yet
- Hypertension in Geriatrics 2010Document51 pagesHypertension in Geriatrics 2010Andre HawkNo ratings yet
- Acquired RHD BestDocument95 pagesAcquired RHD BestauNo ratings yet
- Mudassar Ali Jaffri Mudassar Ali JaffriDocument27 pagesMudassar Ali Jaffri Mudassar Ali JaffriYahya KhanNo ratings yet
- 2lecture RF IE - 070617Document69 pages2lecture RF IE - 070617christomlinNo ratings yet
- Rheumatic Fever: Prof. A K M MohibullahDocument42 pagesRheumatic Fever: Prof. A K M MohibullahNavojit ChowdhuryNo ratings yet
- جاهز للعرضDocument38 pagesجاهز للعرضshamaamo19No ratings yet
- Rheumatic FeverDocument21 pagesRheumatic FeverSaddam HusainNo ratings yet
- Infectious Diseases of The HeartDocument84 pagesInfectious Diseases of The HeartHarold DiasanaNo ratings yet
- Rheumatic FeverDocument56 pagesRheumatic Feveralmawang100% (1)
- Coronary Artery Disease: Aleson Claire A. Llanes, MDDocument94 pagesCoronary Artery Disease: Aleson Claire A. Llanes, MDFly LlanesNo ratings yet
- Endocarditis Blok 10Document50 pagesEndocarditis Blok 10Dena Paramita RustandiNo ratings yet
- Cardiology: Crash Revision Omar K. MRCP IrelandDocument53 pagesCardiology: Crash Revision Omar K. MRCP IrelandManmeet SNo ratings yet
- Penyakit KawasakiDocument30 pagesPenyakit Kawasakimuhammad hidayahNo ratings yet
- Peripheral Vascular Disease: Dr. Fouzal Aswad, SPJPDocument46 pagesPeripheral Vascular Disease: Dr. Fouzal Aswad, SPJPRudy LusmiandaNo ratings yet
- Rheumatic FeverDocument24 pagesRheumatic FeverrameshbmcNo ratings yet
- Preoperative Assessment of Patients With Cardiac Disease Undergoing Noncardiac SurgeryDocument13 pagesPreoperative Assessment of Patients With Cardiac Disease Undergoing Noncardiac SurgeryMădălina RădulescuNo ratings yet
- Transplant Registrar BookletDocument9 pagesTransplant Registrar BookletSamiaNazNo ratings yet
- Rheumatic Fever: DR: Yousif Adam AliDocument20 pagesRheumatic Fever: DR: Yousif Adam AliÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Fever: &knee PainDocument49 pagesFever: &knee PainJohn Christopher LucesNo ratings yet
- Rheumatic - Fever - Internal Medicine 15 MarchDocument35 pagesRheumatic - Fever - Internal Medicine 15 MarchLedia EssamNo ratings yet
- Patent Ductus Arteriosus - Most Common Congenital Heart Defect Symptoms DependDocument5 pagesPatent Ductus Arteriosus - Most Common Congenital Heart Defect Symptoms DependANNENo ratings yet
- Rheumatic Heart DiseaseDocument22 pagesRheumatic Heart Diseasenicholasacquah680No ratings yet
- Acute Rheumatic FeverDocument26 pagesAcute Rheumatic FeverkapilNo ratings yet
- Deep Vein ThrombosisDocument33 pagesDeep Vein ThrombosisWisnu Cahyo100% (1)
- Rheumatic FeverDocument46 pagesRheumatic FeverAbinaya RanganathanNo ratings yet
- 12lec Cardiac InfectionsDocument93 pages12lec Cardiac Infectionsmonica leeNo ratings yet
- Acute Rhuem FeverDocument81 pagesAcute Rhuem FeverchristyNo ratings yet
- Acute Coronary Syndrome EditedDocument38 pagesAcute Coronary Syndrome EditedSurgicalgownNo ratings yet
- Chapter 3 Decision TreesDocument12 pagesChapter 3 Decision TreesMark MagumbaNo ratings yet
- Analysis of GATE 2010Document25 pagesAnalysis of GATE 2010aloo_12345No ratings yet
- Human Rights Term PaperDocument18 pagesHuman Rights Term Papersanjog DewanNo ratings yet
- Japan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk ManagementDocument12 pagesJapan's Jishu-Bosai-Soshiki Community Activities: Analysis of Its Role in Participatory Community Disaster Risk Managementannette_henderson123No ratings yet
- Seizures and EpilepsyDocument54 pagesSeizures and Epilepsyจีทีเอส สุรเชษฐNo ratings yet
- Btap TCQTDocument35 pagesBtap TCQTMai Phạm Hà ThanhNo ratings yet
- Tax Reporter Guide - 2009Document90 pagesTax Reporter Guide - 2009bpathri0% (1)
- Korando 2012Document1,082 pagesKorando 2012mirrahel paim67% (3)
- Taxation: Bmbes 2020 Barangay Micro Business Enterprise BMBE Law's ObjectiveDocument3 pagesTaxation: Bmbes 2020 Barangay Micro Business Enterprise BMBE Law's Objectivekris mNo ratings yet
- Finance Exam Questions #2Document21 pagesFinance Exam Questions #2Cody Chivas100% (1)
- LNM Dow Inspirage 2021 Aug 04 FinalDocument25 pagesLNM Dow Inspirage 2021 Aug 04 FinalJoshua LimNo ratings yet
- 2018 Annual Public Debt ReportDocument79 pages2018 Annual Public Debt ReportDr. Ọbádélé KambonNo ratings yet
- RCC Teen - Task 5 - BandwidthDocument2 pagesRCC Teen - Task 5 - BandwidthRares AndreiNo ratings yet
- DAS-000010revA - Osprey-UVX Customer DatasheetDocument2 pagesDAS-000010revA - Osprey-UVX Customer DatasheetEduardo DmgzNo ratings yet
- CS Form No. 6 Revised 2020 Application For LeaveDocument6 pagesCS Form No. 6 Revised 2020 Application For LeaveMARILYN MALIMBAGNo ratings yet
- Geocentric MoonDocument7 pagesGeocentric MoonBob McDonaldNo ratings yet
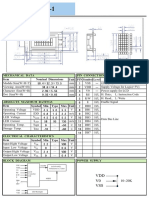
- V0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemDocument1 pageV0 VSS VDD: Unit PIN Symbol Level Nominal Dimensions Pin Connections Function Mechanical Data ItemBasir Ahmad NooriNo ratings yet
- Alcatel-Lucent Omniswitch 6360: Stackable Gigabit Ethernet Lan Switch FamilyDocument9 pagesAlcatel-Lucent Omniswitch 6360: Stackable Gigabit Ethernet Lan Switch FamilyredNo ratings yet
- Name: Aldrich Fernandes Roll No: 06 Subject: Business Ethics and Corporate Governance Purpose: Assignment On Question & AnswersDocument5 pagesName: Aldrich Fernandes Roll No: 06 Subject: Business Ethics and Corporate Governance Purpose: Assignment On Question & AnswersAldrich FernandesNo ratings yet
- 375ElectricalSchematicVNVHDVersion2 6dec2004 A 31 May2005 PV776-20040447Document208 pages375ElectricalSchematicVNVHDVersion2 6dec2004 A 31 May2005 PV776-20040447Gustavo Vargas100% (1)
- Cable - Datasheet - (En) NSSHCÖU, Prysmian - 2013-06-10 - Screened-Power-CableDocument4 pagesCable - Datasheet - (En) NSSHCÖU, Prysmian - 2013-06-10 - Screened-Power-CableA. Muhsin PamungkasNo ratings yet
- SpecsDocument20 pagesSpecscivilISMAEELNo ratings yet
- Deutz 2008 SpecsDocument4 pagesDeutz 2008 SpecsaaasNo ratings yet
- C9 Nazism+and+the+Rise+of+Hitler+ S1Document49 pagesC9 Nazism+and+the+Rise+of+Hitler+ S1raj kumarNo ratings yet
- Choosing An Ecommerce Platform GuideDocument40 pagesChoosing An Ecommerce Platform GuidejeetNo ratings yet
- Bike Booking System FinalDocument29 pagesBike Booking System FinalThe WatcherNo ratings yet
- GeographicRouting WSNDocument22 pagesGeographicRouting WSNJASPER WESSLYNo ratings yet
- Stack-1531324837281 STKDocument4 pagesStack-1531324837281 STKRizalNo ratings yet
- Cellphone SafetyDocument18 pagesCellphone Safetyva4avNo ratings yet
- The Perfect Site GuideDocument59 pagesThe Perfect Site GuideconstantrazNo ratings yet