Download as ppt, pdf, or txt
You might also like
- Compartment SyndromeDocument24 pagesCompartment SyndromeDexter BluesNo ratings yet
- Cephalopelvic Disproportion (CPD)Document20 pagesCephalopelvic Disproportion (CPD)Natukunda Dianah100% (4)
- Management Acute PainDocument110 pagesManagement Acute PainjohannesNo ratings yet
- Pain Pathways & Pain ManagementDocument82 pagesPain Pathways & Pain ManagementAarthiNo ratings yet
- Physiology of Pain Pathways and Its Modulation: DR HassanDocument79 pagesPhysiology of Pain Pathways and Its Modulation: DR HassanvaishnaviNo ratings yet
- Day 1 - Doc Session 1 - Patho Physiology of Pain - DR BijiDocument69 pagesDay 1 - Doc Session 1 - Patho Physiology of Pain - DR Bijim debNo ratings yet
- Manajemen Nyeri Dengan DexketoprofenDocument27 pagesManajemen Nyeri Dengan Dexketoprofenmaya santiNo ratings yet
- Iapc November 2016 Pain PathophysiologyDocument45 pagesIapc November 2016 Pain PathophysiologypradeepNo ratings yet
- Mechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDocument49 pagesMechanisms, Classification and Assesment: Departemen Neurologi Fakutas Kedokteran Universitas Islam Sumatera UtaraDea indah damayantiNo ratings yet
- Peran Akupunktur Medik Pada Kasus NyeriDocument155 pagesPeran Akupunktur Medik Pada Kasus NyeriSilvia HandikaNo ratings yet
- Assessin G: Karelle Custodia Theresa GalivoDocument23 pagesAssessin G: Karelle Custodia Theresa GalivoKarelle CustodiaNo ratings yet
- The Biology of Chronic Pain - May 2005 (No Pictures)Document40 pagesThe Biology of Chronic Pain - May 2005 (No Pictures)Mike SheatNo ratings yet
- MOD014 Nyeri KankerDocument23 pagesMOD014 Nyeri KankerMien Dwi CahyaniNo ratings yet
- Step Ladder in Pain Management (Dr. YNS)Document39 pagesStep Ladder in Pain Management (Dr. YNS)Erick Rangga JuniorNo ratings yet
- Chronic Pain Management: Dr. Ankit GajjarDocument74 pagesChronic Pain Management: Dr. Ankit GajjarDivya Rekha KolliNo ratings yet
- Acute Pain Management FDK RSUD KLDocument36 pagesAcute Pain Management FDK RSUD KLAgoenk PrabowoNo ratings yet
- Pain and NeuralgiaDocument51 pagesPain and NeuralgiaAndika WigunaNo ratings yet
- Pain Pathophysiology: by DR Azmath Begum Unit Chief:Dr KondalreddyDocument34 pagesPain Pathophysiology: by DR Azmath Begum Unit Chief:Dr KondalreddyNimath Unnisa BegumNo ratings yet
- PAIN IN ORTHOPAEDIC DR - ASP EditDocument50 pagesPAIN IN ORTHOPAEDIC DR - ASP EditElisabeth Permatasari SidabutarNo ratings yet
- Manajemen Nyeri: Nella Harisa NovianiDocument30 pagesManajemen Nyeri: Nella Harisa NovianiCitra AnggrainiNo ratings yet
- Patofisiologi NyeriDocument99 pagesPatofisiologi NyeriWandi WDNo ratings yet
- Pain PathwaysDocument45 pagesPain PathwaysKabirNo ratings yet
- 3 DR Hery - Pain Management 2018Document58 pages3 DR Hery - Pain Management 2018SATIYO SATIYONo ratings yet
- Assessing Pain As The Fifth Vital SignsDocument20 pagesAssessing Pain As The Fifth Vital SignsEricka LiwanagNo ratings yet
- DR Yuneldi Anwar Sps (K) Bagian Neurologi Fk-Usu/ Rsup H. Adam Malik MedanDocument59 pagesDR Yuneldi Anwar Sps (K) Bagian Neurologi Fk-Usu/ Rsup H. Adam Malik MedanZikri Putra Lan LubisNo ratings yet
- Tatalaksana NyeriDocument82 pagesTatalaksana NyerimuchlaspraNo ratings yet
- Management of Acute PainDocument76 pagesManagement of Acute PainAnonymous nruHyuwtJ100% (1)
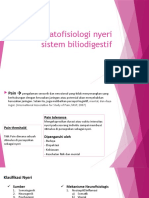
- Patofisiologi Nyeri Sistem BiliodigestifDocument22 pagesPatofisiologi Nyeri Sistem BiliodigestifNathaniaNo ratings yet
- Manajemen Nyeri Motik RS BhinaDocument36 pagesManajemen Nyeri Motik RS Bhinayn_faisalNo ratings yet
- Pain Assessment & ManagementDocument36 pagesPain Assessment & ManagementremeroseNo ratings yet
- Our Lady of Fatima University: By: Mnpargallon, RN, ManDocument37 pagesOur Lady of Fatima University: By: Mnpargallon, RN, ManMaria Jenina CervantesNo ratings yet
- Pain Dr. HenryDocument36 pagesPain Dr. Henryreagan setiawanNo ratings yet
- Pain in The Elderly (Dr. Ann Berger)Document41 pagesPain in The Elderly (Dr. Ann Berger)National Press Foundation100% (1)
- Pain ManagementDocument31 pagesPain ManagementNikki Sharmaine VillahermosaNo ratings yet
- Pain Hand OutsDocument9 pagesPain Hand OutsAnonymous BBs1xxk96V100% (1)
- Manajemen NyeriDocument27 pagesManajemen Nyerivera100% (1)
- 5 Pain ManagementDocument28 pages5 Pain ManagementJANINE SEBASTIANNo ratings yet
- Pappagallo 01Document27 pagesPappagallo 01Steven GodelmanNo ratings yet
- Mod08 Pain Class1 PivotDocument52 pagesMod08 Pain Class1 PivotRafaelNo ratings yet
- Tatalaksana Penanganan Nyeri: Bagian Anestesiologi Dan Perawatan Intensif RSUD Undata / FKIK Untad PaluDocument82 pagesTatalaksana Penanganan Nyeri: Bagian Anestesiologi Dan Perawatan Intensif RSUD Undata / FKIK Untad PaluLiaAswikaViaKostaNo ratings yet
- Gastrits PDFDocument47 pagesGastrits PDFAnas kareemNo ratings yet
- 4.opioids - CC - 28.10.21, 5.11.21Document70 pages4.opioids - CC - 28.10.21, 5.11.217qjyn4jtc6No ratings yet
- Bio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuDocument64 pagesBio-Psycho-Social Aspect of Pain: Madonna Damayanthie DatuRey AlwiwikhNo ratings yet
- Opioid AnalgesicsDocument25 pagesOpioid AnalgesicscchatrumaNo ratings yet
- 1 Pain Sensation Physiology DR Ambreen TauseefDocument73 pages1 Pain Sensation Physiology DR Ambreen TauseefbilalNo ratings yet
- Pain Mechanism Summary TableDocument1 pagePain Mechanism Summary Table27189No ratings yet
- Pain Control in Operative DentistryDocument174 pagesPain Control in Operative DentistryNADEEM SHAIKNo ratings yet
- PainDocument29 pagesPainjolilarmatarNo ratings yet
- Manajemen NyeriDocument30 pagesManajemen NyericlvpratamaNo ratings yet
- Predavanje BOL-stomatologija, 2008Document49 pagesPredavanje BOL-stomatologija, 2008Vukashin.meNo ratings yet
- Nyeri Nosiseptif Sup - XIDocument82 pagesNyeri Nosiseptif Sup - XIDiana SariNo ratings yet
- Alur Manajemen Nyeri Rumah SakitDocument45 pagesAlur Manajemen Nyeri Rumah SakitRadit NasillaNo ratings yet
- Health Assessment in Nursing (LEC)Document50 pagesHealth Assessment in Nursing (LEC)Cj MayoyoNo ratings yet
- Pain AssessmentDocument5 pagesPain AssessmentLuance FabruadaNo ratings yet
- Assessing Pain: Fifth Vital SignDocument10 pagesAssessing Pain: Fifth Vital SignShaira Dawn D. PLANCONo ratings yet
- Pathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiDocument86 pagesPathophysiology and Managemement of Pain: Dr. Subodh Kumar Mahto, Dept. of Medicine Pgimer, DR - RML Hospital. NEW DelhiMarcelo GutiérrezNo ratings yet
- Anes 8 Introduction To Pain ManagementDocument4 pagesAnes 8 Introduction To Pain ManagementJanica Marie RagsacNo ratings yet
- Health Assessment - PainDocument25 pagesHealth Assessment - PainVicencio, JhezelNo ratings yet
- Pain PDFDocument46 pagesPain PDFwokorowNo ratings yet
- Penatalaksanaan Nyeri DLL 2018Document14 pagesPenatalaksanaan Nyeri DLL 2018Silvia HandikaNo ratings yet
- Valvular Heart Disease: Mitral RegurgitationDocument33 pagesValvular Heart Disease: Mitral RegurgitationjihyooniNo ratings yet
- 5 Types of EPI-GDV ImagesDocument5 pages5 Types of EPI-GDV ImagesManagerNo ratings yet
- Casey Infectious Disease PamphletDocument2 pagesCasey Infectious Disease Pamphletapi-552547083No ratings yet
- Hema Nclex Q'SDocument6 pagesHema Nclex Q'SFarmisa MannanNo ratings yet
- Unit Fifteen Alternative TreatmentsDocument3 pagesUnit Fifteen Alternative TreatmentsRoly PadutNo ratings yet
- NHS Pan London Follicular Lymphoma 2018Document18 pagesNHS Pan London Follicular Lymphoma 2018Syed Touseef AhmedNo ratings yet
- Disorders of SodiumDocument13 pagesDisorders of SodiumteranrobleswaltergabrielNo ratings yet
- Types of DiagnosisDocument22 pagesTypes of Diagnosisburraahhhh100% (1)
- Journal ReviewDocument16 pagesJournal Reviewnur ulfahNo ratings yet
- OET Test 1 Listening Answers - Part A and BDocument6 pagesOET Test 1 Listening Answers - Part A and Bjeet meharNo ratings yet
- Clinical Presentation of Abdominal TuberculosisDocument4 pagesClinical Presentation of Abdominal TuberculosisRizky AmaliahNo ratings yet
- CBT Mental Health Print NowDocument17 pagesCBT Mental Health Print Nowchristy INo ratings yet
- NTP Annual Report 2021 v082221Document140 pagesNTP Annual Report 2021 v082221ChrisNo ratings yet
- S1 2022 429533 BibliographyDocument7 pagesS1 2022 429533 BibliographyNur WahyuniNo ratings yet
- Guidline of Management of Porta CathDocument8 pagesGuidline of Management of Porta CathroncekeyNo ratings yet
- Emergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Document5 pagesEmergency Room Nursing Care Plan: Saint Louis University Baguio City School of Nursing S.Y. 2019-2020Wyen CabatbatNo ratings yet
- ImmunizationDocument1 pageImmunizationMicah Lou CalambaNo ratings yet
- Neonatalseizureclinicalguideline PDFDocument15 pagesNeonatalseizureclinicalguideline PDFNURUL NADIA BINTI MOHD NAZIR / UPMNo ratings yet
- Guidelines in Conducting Health AssessmentDocument40 pagesGuidelines in Conducting Health AssessmentHAZEL RODA ESTORQUE100% (2)
- APA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFDocument3 pagesAPA - DSM5 - Severity Measure For Separation Anxiety Disorder Adult PDFMelissandreNo ratings yet
- Neurosurgery of The Visual PathwayDocument33 pagesNeurosurgery of The Visual PathwaysoitaNo ratings yet
- 1 SMDocument15 pages1 SMemmanuellagrace06No ratings yet
- Headaches - Ira RahmawatiDocument20 pagesHeadaches - Ira RahmawatiPutri NaylaaNo ratings yet
- Anorexia NervosaDocument5 pagesAnorexia NervosaPoonam RanaNo ratings yet
- Head and Neck Seminal Papers From Tata HospitalDocument29 pagesHead and Neck Seminal Papers From Tata HospitalSudhir NairNo ratings yet
- Drug-Induced Pigmentation: BackgroundDocument4 pagesDrug-Induced Pigmentation: BackgroundHiedajatNo ratings yet
- Meningismus Vs MeningitisDocument19 pagesMeningismus Vs MeningitisRanna HertenizaNo ratings yet
- Government of Rajasthan Finance Department Rules DivisionDocument2 pagesGovernment of Rajasthan Finance Department Rules DivisionSadanand PariharNo ratings yet