Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Handle Large Messages in Apache KafkaDocument59 pagesHandle Large Messages in Apache KafkaBùi Văn KiênNo ratings yet
- Leaflet Infection ControlDocument2 pagesLeaflet Infection ControlMin MinNo ratings yet
- New Stats On DrugDocument2 pagesNew Stats On DrugMin MinNo ratings yet
- Our Undertaking Is To ProvideDocument7 pagesOur Undertaking Is To ProvideMin MinNo ratings yet
- CJ400 02Document26 pagesCJ400 02Min MinNo ratings yet
- Surgical Site Infection (SSI) Event: Table 1 CDC 57.106Document27 pagesSurgical Site Infection (SSI) Event: Table 1 CDC 57.106Min MinNo ratings yet
- Event Proposal FullDocument4 pagesEvent Proposal FullDarren Kate LicupaNo ratings yet
- Control of Power System OscillationsDocument9 pagesControl of Power System OscillationsgabriveragNo ratings yet
- EDA VHDL SimulationDocument19 pagesEDA VHDL SimulationYQ WNo ratings yet
- Electrical Test Procedures For Armatures, Stators and MotorsDocument7 pagesElectrical Test Procedures For Armatures, Stators and MotorsCarlosNo ratings yet
- Solar PV Survey FormDocument6 pagesSolar PV Survey FormDigital designsNo ratings yet
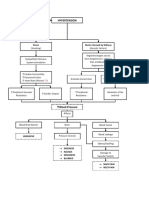
- Hypertension Concept MapDocument1 pageHypertension Concept Mapjyd parreñoNo ratings yet
- MidTerm K64 1Document1 pageMidTerm K64 1lion meo meoNo ratings yet
- AV UWorld EOs (Rough Draft) - Data - Repeat LandscapeDocument139 pagesAV UWorld EOs (Rough Draft) - Data - Repeat LandscapeJonathan AiresNo ratings yet
- 1 - Norovirus Care Home Poster 2018Document1 page1 - Norovirus Care Home Poster 2018GarryNo ratings yet
- SH SingleDocument52 pagesSH SingleNivaldoNo ratings yet
- Egypt: Gec08-Science, Technology & Society Modern AgesDocument7 pagesEgypt: Gec08-Science, Technology & Society Modern AgesNo NameNo ratings yet
- En 2014-03-17 RTU500 Series Product Catalogue OnlineDocument78 pagesEn 2014-03-17 RTU500 Series Product Catalogue OnlineЖорж КаназирскиNo ratings yet
- Robson - Tradition 1 MW 1951Document12 pagesRobson - Tradition 1 MW 1951Arputharaj SamuelNo ratings yet
- Civil Measeurement FSIPLDocument12 pagesCivil Measeurement FSIPLAnupNo ratings yet
- Antibiogram of Bacterial Isolates From Cervico-Vaginal Mucus (CVM) of Endometritic CowsDocument5 pagesAntibiogram of Bacterial Isolates From Cervico-Vaginal Mucus (CVM) of Endometritic CowsY.rajuNo ratings yet
- O-Ring Material Offering Guide: ORD 5712 Effective September 2004Document84 pagesO-Ring Material Offering Guide: ORD 5712 Effective September 2004Samir FerreiraNo ratings yet
- Analysis and Design of A Charge Pump Circuit For High CurrentDocument4 pagesAnalysis and Design of A Charge Pump Circuit For High CurrenthsharghiNo ratings yet
- MCDonald's StrategyDocument3 pagesMCDonald's StrategyShaukat HasanNo ratings yet
- in Outcomes-Based Education, Which of The Following Are Not Considered Outcomes? A. Products B. Procedures C. Portfolios D. PerformancesDocument50 pagesin Outcomes-Based Education, Which of The Following Are Not Considered Outcomes? A. Products B. Procedures C. Portfolios D. PerformancesClarissa TorrelinoNo ratings yet
- IcrmnDocument26 pagesIcrmnAbhishek ThakurNo ratings yet
- Femto SONDocument19 pagesFemto SONIlya KryuchkovNo ratings yet
- AFI - 10-248 - Fitness ProgramDocument89 pagesAFI - 10-248 - Fitness ProgramDongelxNo ratings yet
- Customer Satisfaction and Employee InvolvementDocument36 pagesCustomer Satisfaction and Employee InvolvementMaria Rebecca Toledo SalarNo ratings yet
- HOA5 Question PapersDocument5 pagesHOA5 Question Papersrevathi hariharanNo ratings yet
- LAS 1A The Magic PomegranateDocument2 pagesLAS 1A The Magic PomegranateCherry Maravilla Basa MingoaNo ratings yet
- Stanford - Discrete Time Markov Chains PDFDocument23 pagesStanford - Discrete Time Markov Chains PDFSofoklisNo ratings yet
- ASUS RT-AC58U ManualDocument122 pagesASUS RT-AC58U ManualSeungpyo HongNo ratings yet
- Republic Act No. 7722: Higher Education Act of 1994Document45 pagesRepublic Act No. 7722: Higher Education Act of 1994belle100% (2)
- Creation, Torah, and Revealed Wisdom in Some Second Temple Sapiential Texts (Sirach, 4qinstruction, 4Q185, and 4Q525) : A Response To John KampenDocument24 pagesCreation, Torah, and Revealed Wisdom in Some Second Temple Sapiential Texts (Sirach, 4qinstruction, 4Q185, and 4Q525) : A Response To John KampenKent Jerson CasianoNo ratings yet