Download as pptx, pdf, or txt
You might also like
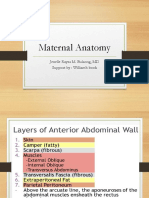
- Maternal Anatomy WilliamsDocument60 pagesMaternal Anatomy WilliamsZari Novela100% (2)
- ProbabilityArea Model Activity CompanionDocument2 pagesProbabilityArea Model Activity CompanionZari Novela0% (1)
- Student Doctor MethodDocument46 pagesStudent Doctor MethodSubianand100% (2)
- MalpresentationDocument37 pagesMalpresentationLovely SarangiNo ratings yet
- OB-Gyn Case Presentation - BicornuateDocument53 pagesOB-Gyn Case Presentation - BicornuateZari Novela100% (1)
- Dystocia: DR - Selvaraj, Chinnasamy M.DDocument54 pagesDystocia: DR - Selvaraj, Chinnasamy M.DSelvaraj ChinnasamyNo ratings yet
- Abnormal Labor and Dystocia: By: Norliana Binti JaafarDocument50 pagesAbnormal Labor and Dystocia: By: Norliana Binti JaafarNorliana Jaafar0% (1)
- Skills Delivery TeachingDocument84 pagesSkills Delivery TeachingRandyNo ratings yet
- Stages of Fetal DevelopmentDocument92 pagesStages of Fetal DevelopmentMelissa Diego-sarmiento100% (1)
- MalpresentationDocument19 pagesMalpresentationHanelie B. AldeaNo ratings yet
- Immediate Care in PostnatalDocument12 pagesImmediate Care in Postnatalvarshasharma05No ratings yet
- Nursing Care During Normal Pregnancy & Care of Developing FetusDocument15 pagesNursing Care During Normal Pregnancy & Care of Developing FetusLuna Sang-an100% (1)
- Final Ob1Document14 pagesFinal Ob1crix crixNo ratings yet
- Fetal MalpresentationDocument83 pagesFetal MalpresentationArianJubaneNo ratings yet
- Postpartum 08Document49 pagesPostpartum 08Quolette ConstanteNo ratings yet
- Fetal Malpresentations: Abundo, Esther Ellise Espinol, Hazel AnnDocument21 pagesFetal Malpresentations: Abundo, Esther Ellise Espinol, Hazel AnnEsther Ellise Abundo100% (1)
- Obsteric EmergenciesDocument48 pagesObsteric EmergenciesNurul AshikinNo ratings yet
- Ps of LaborDocument28 pagesPs of LaborErvina Luisa Delias CampusNo ratings yet
- Labor and Delivery TopicsDocument44 pagesLabor and Delivery TopicsAngela Joy AmparadoNo ratings yet
- Shoulder Face PresentationDocument37 pagesShoulder Face PresentationOmar mohamedNo ratings yet
- Normal and Abnormal Present IonDocument31 pagesNormal and Abnormal Present IondeemNo ratings yet
- Introduction To Maternal NursingDocument128 pagesIntroduction To Maternal NursingNathalina DeepikaNo ratings yet
- Fetal MalpresentationDocument33 pagesFetal MalpresentationMichael Angelo Seña100% (1)
- Obstetrical Emergency & ManagementDocument38 pagesObstetrical Emergency & ManagementDrPreeti Thakur ChouhanNo ratings yet
- Obstructed Labor & Prolonged LaburDocument22 pagesObstructed Labor & Prolonged LaburOmari Kabelwa100% (1)
- Normal Labour in Obstetric2Document17 pagesNormal Labour in Obstetric2Tejasvi ChavdaNo ratings yet
- PostpartumDocument3 pagesPostpartumMuhammad RifaiNo ratings yet
- Normal Conduct of LaborDocument62 pagesNormal Conduct of LaborFaye Cabotaje LinganNo ratings yet
- Anatomical and Physiological Changes During PregnancyDocument25 pagesAnatomical and Physiological Changes During Pregnancyqaleeq100% (1)
- Introduction To Obstetrics & Midwifery CareDocument18 pagesIntroduction To Obstetrics & Midwifery CareWhirmey ChinyamaNo ratings yet
- AbortionDocument62 pagesAbortionRaj KumarNo ratings yet
- Midwifery CurriculumDocument98 pagesMidwifery CurriculumMunawar100% (1)
- Diagnosis of PregnancyDocument42 pagesDiagnosis of PregnancyAastha BistaNo ratings yet
- Abnormal LabourDocument12 pagesAbnormal Labourabidul hoqueNo ratings yet
- DystociaDocument17 pagesDystociaKarinaNo ratings yet
- AFE, RUPTURE OF UTERUS, (Autosaved)Document31 pagesAFE, RUPTURE OF UTERUS, (Autosaved)maezu100% (1)
- Abruptio PlacentaDocument20 pagesAbruptio PlacentaAlphine DalgoNo ratings yet
- Signs of LaborDocument5 pagesSigns of Labormarianne_07No ratings yet
- Nursing Care of Family During Labor and BirthhhDocument6 pagesNursing Care of Family During Labor and BirthhhAudreySalvadorNo ratings yet
- Breech DeliveryDocument6 pagesBreech DeliveryNyoman TapayanaNo ratings yet
- EngorgementDocument1 pageEngorgementVijith.V.kumarNo ratings yet
- First Stage of Labor ManagementDocument6 pagesFirst Stage of Labor ManagementFarheen khanNo ratings yet
- PuerperiumDocument28 pagesPuerperiumZarlyn MirafloresNo ratings yet
- Abortion: TH THDocument36 pagesAbortion: TH THdimly100% (1)
- Complications of Labor and DeliveryDocument5 pagesComplications of Labor and DeliveryLovelyn Joy Abubo CortezNo ratings yet
- Many Types:: Definition of Malpresentation: Any Presentation Other Than Vertex PresentationDocument5 pagesMany Types:: Definition of Malpresentation: Any Presentation Other Than Vertex PresentationMelissa Aina Mohd YusofNo ratings yet
- MalpresentationDocument37 pagesMalpresentationLovely SarangiNo ratings yet
- Shoulder DystociaDocument14 pagesShoulder Dystociarake sardevaNo ratings yet
- Rhesus Isoimmunization: Ishen PerumalDocument29 pagesRhesus Isoimmunization: Ishen PerumalIshen PerumalNo ratings yet
- Operative ObstetricsDocument4 pagesOperative Obstetricssarguss14100% (3)
- Placenta CirculationDocument11 pagesPlacenta CirculationJason Jimmy Lee PillayNo ratings yet
- Pregnancy CareDocument17 pagesPregnancy CareHONEYNo ratings yet
- Fix Care of NewbornDocument39 pagesFix Care of Newborngratzia fionaNo ratings yet
- Before Starting The Presentation, I Am Requesting You All To Get A HandkerchiefDocument35 pagesBefore Starting The Presentation, I Am Requesting You All To Get A HandkerchiefOng KarlNo ratings yet
- Postpartum Care - GLOWMDocument13 pagesPostpartum Care - GLOWMAli KhaterNo ratings yet
- Abortion: Maxima Vera Pinalgan, MDDocument21 pagesAbortion: Maxima Vera Pinalgan, MDgayon09No ratings yet
- 18 - Oligohydramnios and PolyhydramniosDocument3 pages18 - Oligohydramnios and PolyhydramniosSu OoNo ratings yet
- Fetal MalpresentationDocument28 pagesFetal MalpresentationAhmed Gh Al-zechrawiNo ratings yet
- Post Partum HemorhageDocument7 pagesPost Partum HemorhageLithiya JoseNo ratings yet
- Inversion of Uterus 170225210149Document54 pagesInversion of Uterus 170225210149anju kumawatNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky Amalia100% (1)
- Genital ProlapseDocument3 pagesGenital Prolapsecraniophage95No ratings yet
- Measure of VariabilityDocument3 pagesMeasure of VariabilityZari NovelaNo ratings yet
- Venn DiagramDocument33 pagesVenn DiagramZari NovelaNo ratings yet
- Role Master TeacherDocument1 pageRole Master TeacherZari NovelaNo ratings yet
- SAH RevisedDocument41 pagesSAH RevisedZari NovelaNo ratings yet
- Barangay Letter - Electric WireDocument1 pageBarangay Letter - Electric WireZari NovelaNo ratings yet
- Amino Acids and ProteinsDocument9 pagesAmino Acids and ProteinsZari NovelaNo ratings yet
- Glaucoma: Zarieh Dawn Novela Medicine 2Document41 pagesGlaucoma: Zarieh Dawn Novela Medicine 2Zari NovelaNo ratings yet
- Retina: Zarieh Dawn L. Novela Medicine 2Document50 pagesRetina: Zarieh Dawn L. Novela Medicine 2Zari NovelaNo ratings yet
- Health Education ProgramDocument4 pagesHealth Education ProgramZari Novela100% (1)
- Animal Physio Lab Report3-OsmoregulationDocument7 pagesAnimal Physio Lab Report3-OsmoregulationZari Novela100% (1)
- Case Analysis: Prepared by Kezia Cryzl L. Novela Hrs-2 A Submitted ToDocument1 pageCase Analysis: Prepared by Kezia Cryzl L. Novela Hrs-2 A Submitted ToZari NovelaNo ratings yet
- Management of MhoDocument5 pagesManagement of MhoZari NovelaNo ratings yet
- Lesson 5Document21 pagesLesson 5TrishaNo ratings yet
- Feeling Sick: Vocabulary CheckDocument6 pagesFeeling Sick: Vocabulary CheckCLAUDIA ARELLANONo ratings yet
- Volunteer Application Form Updated 5-2017 PDFDocument2 pagesVolunteer Application Form Updated 5-2017 PDFDiane AngelineNo ratings yet
- NikolDocument6 pagesNikolIsaiah Nia PascualNo ratings yet
- Enteral Feeding: Indications, Complications, and Nursing CareDocument6 pagesEnteral Feeding: Indications, Complications, and Nursing CareSheena CabrilesNo ratings yet
- Holistic ApproachDocument16 pagesHolistic ApproachVINCENT MUHARINo ratings yet
- Experiment No.9 Potassium Nitrate ObjectiveDocument3 pagesExperiment No.9 Potassium Nitrate ObjectiveBlazy InhumangNo ratings yet
- Ostomy CareNursing - SkillDocument1 pageOstomy CareNursing - SkillAA DDNo ratings yet
- A Beautiful Mind-Jason PadgettDocument11 pagesA Beautiful Mind-Jason PadgettvishalankitNo ratings yet
- Tugas DR Vanda Covid 19 in Scuba DivingDocument2 pagesTugas DR Vanda Covid 19 in Scuba Divingfrd2c456ydNo ratings yet
- Sommerlad-2003-Plastic and Reconstructive SurgeryDocument7 pagesSommerlad-2003-Plastic and Reconstructive SurgeryAbdul HameedNo ratings yet
- Evans, Alice MEMOIRS Retyped 2020Document58 pagesEvans, Alice MEMOIRS Retyped 2020Katherine McKennaNo ratings yet
- Evaluation of Chronic Renal Disease, A Staged ApproachDocument8 pagesEvaluation of Chronic Renal Disease, A Staged Approachtaner_soysurenNo ratings yet
- New England Journal Medicine: The ofDocument9 pagesNew England Journal Medicine: The ofalibakirNo ratings yet
- Ventilation Mini ManualDocument44 pagesVentilation Mini ManualKhusnul DwinitaNo ratings yet
- Bettencourt Et Al - 2017Document5 pagesBettencourt Et Al - 2017Andreia BettencourtNo ratings yet
- CSIC - January 2019Document52 pagesCSIC - January 2019rakikiraNo ratings yet
- Laparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleDocument4 pagesLaparoscopic Cholecystectomy:An Experience of 200 Cases: Original ArticleAndrei GheorghitaNo ratings yet
- Measles Case Reporting Form I.Case Identification/ Demographic DetailsDocument2 pagesMeasles Case Reporting Form I.Case Identification/ Demographic DetailsActivity ManagerNo ratings yet
- Plant Pathology - SG 2.0Document8 pagesPlant Pathology - SG 2.0Cha ChaNo ratings yet
- Polyphenols Health Benefits PDFDocument10 pagesPolyphenols Health Benefits PDFfather.mckenzie.twitterNo ratings yet
- Shear FlowDocument20 pagesShear FlowHaithem HammoudaNo ratings yet
- Standard of Nursing ServicesDocument30 pagesStandard of Nursing Servicesjvfaderon7492% (25)
- Genetic Polymorphisms Personalized MedicineDocument38 pagesGenetic Polymorphisms Personalized MedicineBayu WisnuNo ratings yet
- Loneliness - ScribdDocument66 pagesLoneliness - ScribdNoob GulalaNo ratings yet
- Senate Aging Report Sudden Price Spikes in Off Patent Prescription DrugsDocument131 pagesSenate Aging Report Sudden Price Spikes in Off Patent Prescription DrugskmccoynycNo ratings yet
- Community Health Project TopicsDocument3 pagesCommunity Health Project Topicsthomasgrace0107No ratings yet
- Mature Times July 2011Document12 pagesMature Times July 2011Aiken StandardNo ratings yet
- Oral Viral Infections Diagnosis and ManagementDocument13 pagesOral Viral Infections Diagnosis and ManagementhunarsandhuNo ratings yet