
MR Bunga CA Recti
MR Bunga CA Recti
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anti-Diet Reclaim Your Time, Money, Well-Being and Happiness Through Intuitive Eating by Christy HarrisonDocument281 pagesAnti-Diet Reclaim Your Time, Money, Well-Being and Happiness Through Intuitive Eating by Christy HarrisonDann' Mendoza Ü100% (1)
- PQM-700 Manual v1.07.1 GB PDFDocument86 pagesPQM-700 Manual v1.07.1 GB PDFmuhdshafiq12No ratings yet
- Shakti VahiniDocument22 pagesShakti VahiniPragyesh Pratap SinghNo ratings yet
- Section 1.3 - Evaluating Limits AnalyticallyDocument20 pagesSection 1.3 - Evaluating Limits Analyticallyseetha_thundena301No ratings yet
- People vs. Baldogo, G.R. Nos. 128106 07 January 24, 2003Document1 pagePeople vs. Baldogo, G.R. Nos. 128106 07 January 24, 2003Mark ReyesNo ratings yet
- Advantages and Disadvantages of Global WarmingDocument11 pagesAdvantages and Disadvantages of Global WarmingA Aldika Farlis50% (2)
- Hidayatullah National Law University, RaipurDocument42 pagesHidayatullah National Law University, RaipurIshwarNo ratings yet
- Peoria County Jail Booking Sheet For Aug. 8, 2016Document5 pagesPeoria County Jail Booking Sheet For Aug. 8, 2016Journal Star police documentsNo ratings yet
- Philosophy DLLDocument10 pagesPhilosophy DLLGiljohn SoberanoNo ratings yet
- Calculating Lost Labor Productivity-Is There A Better WayDocument17 pagesCalculating Lost Labor Productivity-Is There A Better Waypatrickcarvalho6df100% (1)
- Your Adv Plus Banking: Account SummaryDocument7 pagesYour Adv Plus Banking: Account SummaryRafaelNo ratings yet
- Disproportionate Identification of Minorities in Special EducationDocument4 pagesDisproportionate Identification of Minorities in Special Educationapi-656943209No ratings yet
- Seminar On Contemparary Issues in ManagementDocument4 pagesSeminar On Contemparary Issues in ManagementNaimish BodarNo ratings yet
- Solar Water Heater BOQDocument69 pagesSolar Water Heater BOQSami Al-aminNo ratings yet
- Homework 3 - Solutions: Complex VariablesDocument2 pagesHomework 3 - Solutions: Complex VariablesderlavaiNo ratings yet
- EoDocument139 pagesEoVientihAgNo ratings yet
- PFT FormDocument1 pagePFT FormConnie Diaz CarmonaNo ratings yet
- Discourse Analysis: Ove K. PedersenDocument9 pagesDiscourse Analysis: Ove K. Pedersenmervat_aastNo ratings yet
- Tan Delta Cable TestingDocument6 pagesTan Delta Cable Testingdamlan1100% (2)
- Assignment 7 Lesson Plans Revised For PortfolioDocument11 pagesAssignment 7 Lesson Plans Revised For Portfolioapi-224842070No ratings yet
- CSP Information For SCAA Heritage StudentsDocument1 pageCSP Information For SCAA Heritage Studentsjorge luciano rodriguez nuñezNo ratings yet
- Cstring Management: Joseph M. NewcomerDocument17 pagesCstring Management: Joseph M. NewcomerRodrigo A SaucedoNo ratings yet
- Copy of Famous Educator Infographic Template ExampleDocument1 pageCopy of Famous Educator Infographic Template Exampleapi-643989450No ratings yet
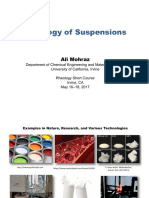
- RheologyShortCourse Lecture10 PDFDocument67 pagesRheologyShortCourse Lecture10 PDFMehdi EzadiNo ratings yet
- Diabetic Ketoacidosis and New Onset DiabetesDocument3 pagesDiabetic Ketoacidosis and New Onset DiabetessabrinaNo ratings yet
- WP - Demystifying The Demo Solution LandscapeDocument6 pagesWP - Demystifying The Demo Solution LandscapeJigar VikamseyNo ratings yet
- Concept Map 1Document1 pageConcept Map 1api-451076853No ratings yet
- Buber Resume2019 2Document2 pagesBuber Resume2019 2Matthew BuberNo ratings yet
- Moorish HistoryDocument72 pagesMoorish HistorySaadiq El-Haqq100% (2)
- Venturi MetersDocument2 pagesVenturi MetersBala SubrahmanyamNo ratings yet





































































Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anti-Diet Reclaim Your Time, Money, Well-Being and Happiness Through Intuitive Eating by Christy HarrisonDocument281 pagesAnti-Diet Reclaim Your Time, Money, Well-Being and Happiness Through Intuitive Eating by Christy HarrisonDann' Mendoza Ü100% (1)
- PQM-700 Manual v1.07.1 GB PDFDocument86 pagesPQM-700 Manual v1.07.1 GB PDFmuhdshafiq12No ratings yet
- Shakti VahiniDocument22 pagesShakti VahiniPragyesh Pratap SinghNo ratings yet
- Section 1.3 - Evaluating Limits AnalyticallyDocument20 pagesSection 1.3 - Evaluating Limits Analyticallyseetha_thundena301No ratings yet
- People vs. Baldogo, G.R. Nos. 128106 07 January 24, 2003Document1 pagePeople vs. Baldogo, G.R. Nos. 128106 07 January 24, 2003Mark ReyesNo ratings yet
- Advantages and Disadvantages of Global WarmingDocument11 pagesAdvantages and Disadvantages of Global WarmingA Aldika Farlis50% (2)
- Hidayatullah National Law University, RaipurDocument42 pagesHidayatullah National Law University, RaipurIshwarNo ratings yet
- Peoria County Jail Booking Sheet For Aug. 8, 2016Document5 pagesPeoria County Jail Booking Sheet For Aug. 8, 2016Journal Star police documentsNo ratings yet
- Philosophy DLLDocument10 pagesPhilosophy DLLGiljohn SoberanoNo ratings yet
- Calculating Lost Labor Productivity-Is There A Better WayDocument17 pagesCalculating Lost Labor Productivity-Is There A Better Waypatrickcarvalho6df100% (1)
- Your Adv Plus Banking: Account SummaryDocument7 pagesYour Adv Plus Banking: Account SummaryRafaelNo ratings yet
- Disproportionate Identification of Minorities in Special EducationDocument4 pagesDisproportionate Identification of Minorities in Special Educationapi-656943209No ratings yet
- Seminar On Contemparary Issues in ManagementDocument4 pagesSeminar On Contemparary Issues in ManagementNaimish BodarNo ratings yet
- Solar Water Heater BOQDocument69 pagesSolar Water Heater BOQSami Al-aminNo ratings yet
- Homework 3 - Solutions: Complex VariablesDocument2 pagesHomework 3 - Solutions: Complex VariablesderlavaiNo ratings yet
- EoDocument139 pagesEoVientihAgNo ratings yet
- PFT FormDocument1 pagePFT FormConnie Diaz CarmonaNo ratings yet
- Discourse Analysis: Ove K. PedersenDocument9 pagesDiscourse Analysis: Ove K. Pedersenmervat_aastNo ratings yet
- Tan Delta Cable TestingDocument6 pagesTan Delta Cable Testingdamlan1100% (2)
- Assignment 7 Lesson Plans Revised For PortfolioDocument11 pagesAssignment 7 Lesson Plans Revised For Portfolioapi-224842070No ratings yet
- CSP Information For SCAA Heritage StudentsDocument1 pageCSP Information For SCAA Heritage Studentsjorge luciano rodriguez nuñezNo ratings yet
- Cstring Management: Joseph M. NewcomerDocument17 pagesCstring Management: Joseph M. NewcomerRodrigo A SaucedoNo ratings yet
- Copy of Famous Educator Infographic Template ExampleDocument1 pageCopy of Famous Educator Infographic Template Exampleapi-643989450No ratings yet
- RheologyShortCourse Lecture10 PDFDocument67 pagesRheologyShortCourse Lecture10 PDFMehdi EzadiNo ratings yet
- Diabetic Ketoacidosis and New Onset DiabetesDocument3 pagesDiabetic Ketoacidosis and New Onset DiabetessabrinaNo ratings yet
- WP - Demystifying The Demo Solution LandscapeDocument6 pagesWP - Demystifying The Demo Solution LandscapeJigar VikamseyNo ratings yet
- Concept Map 1Document1 pageConcept Map 1api-451076853No ratings yet
- Buber Resume2019 2Document2 pagesBuber Resume2019 2Matthew BuberNo ratings yet
- Moorish HistoryDocument72 pagesMoorish HistorySaadiq El-Haqq100% (2)
- Venturi MetersDocument2 pagesVenturi MetersBala SubrahmanyamNo ratings yet