
Bologna Guidelines For Diagnosis and Management
Bologna Guidelines For Diagnosis and Management
You might also like
- Pedia 2.1 - Pediatric History (Vision) PDFDocument5 pagesPedia 2.1 - Pediatric History (Vision) PDFKaren ValdezNo ratings yet
- Pelayanan Digestif November 2021Document12 pagesPelayanan Digestif November 2021ari irawanNo ratings yet
- Foetal Organ Trafficking in The USDocument5 pagesFoetal Organ Trafficking in The USSister RosettaNo ratings yet
- Pande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byDocument32 pagesPande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byanon_550250832100% (1)
- Slide Jurnal BTKVDocument14 pagesSlide Jurnal BTKVVistaririnNo ratings yet
- Retractile TestisDocument7 pagesRetractile TestisAhmad Rahmat Ramadhan TantuNo ratings yet
- Fusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelainDocument7 pagesFusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelaintarekrabiNo ratings yet
- Partograph: Jillian A. Bejoc, MSN, RNDocument44 pagesPartograph: Jillian A. Bejoc, MSN, RNJiezl Abellano AfinidadNo ratings yet
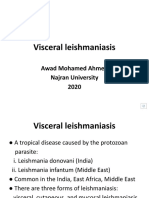
- Visceral Leishmaniasis RecordedDocument19 pagesVisceral Leishmaniasis RecordedFemale calmNo ratings yet
- HERNIORRAPHY (Hernioplasty)Document37 pagesHERNIORRAPHY (Hernioplasty)Aldo AtjehNo ratings yet
- Chapter 36 - Visceral Leishmaniasis and TrypanosomiasisDocument99 pagesChapter 36 - Visceral Leishmaniasis and TrypanosomiasisHyny P'gallaNo ratings yet
- LumbotomiDocument14 pagesLumbotomiazka novriandiNo ratings yet
- Tinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus DecubitusDocument6 pagesTinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus Decubitusrinaldy prayudhiaNo ratings yet
- Chest TubeDocument8 pagesChest TubeTaufik Nur YahyaNo ratings yet
- Jurnal BTKV Herman 1Document11 pagesJurnal BTKV Herman 1Elyas MuhammadNo ratings yet
- Nephrostomy - DR Christopher WattsDocument39 pagesNephrostomy - DR Christopher WattsNidaChoerunnisa100% (1)
- Tg13: Updated Tokyo Guidelinesfor Acute CholecystitisDocument59 pagesTg13: Updated Tokyo Guidelinesfor Acute CholecystitisDeoValendraNo ratings yet
- AdhesiolisisDocument22 pagesAdhesiolisisRisal WintokoNo ratings yet
- BedahDocument139 pagesBedahLunaFia100% (1)
- WIFI Score For Diabetes Foot UlcerDocument17 pagesWIFI Score For Diabetes Foot Ulcertonylee24100% (1)
- Choledochal Cyst: Ronak Patel, DO PGY-3Document11 pagesCholedochal Cyst: Ronak Patel, DO PGY-3Ronak PatelNo ratings yet
- Akses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaDocument28 pagesAkses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaSaeful AmbariNo ratings yet
- Terapi Cairan: Jayapura General Hospital Dept Anesthesiology & Reanimation, Cenderawasih University, School of MedicineDocument31 pagesTerapi Cairan: Jayapura General Hospital Dept Anesthesiology & Reanimation, Cenderawasih University, School of Medicinehandayani nurfitrianaNo ratings yet
- Non Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019Document50 pagesNon Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019peroksidaseNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Wound Healing Normal and Abnormal Mechanisms and Closure TechniquesDocument40 pagesWound Healing Normal and Abnormal Mechanisms and Closure TechniquesAhmad Fakhrozi Helmi100% (1)
- Duodenal InjuryDocument54 pagesDuodenal InjuryTony HardianNo ratings yet
- Catatan DSTC CourseDocument3 pagesCatatan DSTC CourseHanny FadhilaNo ratings yet
- Icd 9 Obstetri N Gynek Plus TindakanDocument4 pagesIcd 9 Obstetri N Gynek Plus TindakanMimi Nanda Miranda AnastasiaNo ratings yet
- HerniaDocument61 pagesHerniaAhmed HassanNo ratings yet
- LONG CASE Luka BakarDocument16 pagesLONG CASE Luka BakarAfiazka LuthfitaNo ratings yet
- Colonoscopy CecilDocument14 pagesColonoscopy Cecilyaba100% (1)
- Rangkuman Salter Bab 14Document64 pagesRangkuman Salter Bab 14Febee NathaliaNo ratings yet
- Cara Mengukur Tekanan IntrakompartemenDocument2 pagesCara Mengukur Tekanan Intrakompartemenfatimah putriNo ratings yet
- JAAOS-Management of Hemorrhage in Life-Threatening Pelvic Fracture 162Document11 pagesJAAOS-Management of Hemorrhage in Life-Threatening Pelvic Fracture 162Enny Yunita HariantiNo ratings yet
- Tracheostomy: Berlian Chevi A. 20184010030Document26 pagesTracheostomy: Berlian Chevi A. 20184010030Berlian Chevi e'Xgepz ThrearsansNo ratings yet
- Dr. Kiki - Pengantar Trauma UpdateDocument20 pagesDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- Shock Management, by Ayman RawehDocument15 pagesShock Management, by Ayman RawehaymxNo ratings yet
- Diabetes Mellitus Pada Anak KuliahDocument51 pagesDiabetes Mellitus Pada Anak KuliahNisha AnggiaNo ratings yet
- Trauma - Pediatric TraumaDocument20 pagesTrauma - Pediatric TraumaLukman NurfauziNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Oeis SyndromeDocument9 pagesOeis SyndromeADEENo ratings yet
- Total Penectomy Urooncology 12thDocument10 pagesTotal Penectomy Urooncology 12thdr. Joko WibowoNo ratings yet
- Syok Hypovolemik-IH FK UMSU2012Document45 pagesSyok Hypovolemik-IH FK UMSU2012Ratika Ayu PiliangNo ratings yet
- (Upgraded) BDH6 - Emergency Trauma & Non Trauma UroDocument122 pages(Upgraded) BDH6 - Emergency Trauma & Non Trauma Uronabila safiraNo ratings yet
- Chronic Limb Threatening IschemiaDocument35 pagesChronic Limb Threatening Ischemiasifatullah khanNo ratings yet
- Fracture and Dislocation-Rahardyan Magetsari (2016) PDFDocument105 pagesFracture and Dislocation-Rahardyan Magetsari (2016) PDFRobertOktaChandraNo ratings yet
- Stoma Siting - Iful Syarif Al MunawiDocument17 pagesStoma Siting - Iful Syarif Al MunawiRamdhani MaulanaNo ratings yet
- Torsio Testis2016Document6 pagesTorsio Testis2016Patrico Rillah SetiawanNo ratings yet
- Acute Pancreatitis: Methas Arunnart MD. Songkhla HospitalDocument70 pagesAcute Pancreatitis: Methas Arunnart MD. Songkhla HospitalMohd ImranNo ratings yet
- Hirschsprung DiseaseDocument20 pagesHirschsprung DiseaseIyan AsianaNo ratings yet
- KARSINOMA TIROID ZakiDocument31 pagesKARSINOMA TIROID ZakiDenny LukasNo ratings yet
- Jurnal DigestiveDocument9 pagesJurnal DigestiveFrancesc OktofabregasNo ratings yet
- OsteosarkomaDocument2 pagesOsteosarkomaLinawati DLNo ratings yet
- Chronic Limb IschemiaDocument29 pagesChronic Limb IschemiaSadia NaveedNo ratings yet
- Tracheostomy: Indications and ProcedureDocument10 pagesTracheostomy: Indications and ProcedureAinur AbdrakhmanovaNo ratings yet
- CSP Groin LumpDocument39 pagesCSP Groin LumpFebby ShabrinaNo ratings yet
- Fistel Vesicovaginalis, Ureterocutaneous, Dan UreterorectalisDocument24 pagesFistel Vesicovaginalis, Ureterocutaneous, Dan Ureterorectalismizz_jcNo ratings yet
- Terapi PaliatifDocument46 pagesTerapi PaliatifViviViviNo ratings yet
- CSS Airway Management RickyDocument53 pagesCSS Airway Management RickyArtha PutuNo ratings yet
- 2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesDocument11 pages2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesOlteanu IonutNo ratings yet
- Wound HealingDocument62 pagesWound HealingRisPerdanaNo ratings yet
- Small Bowel Obstruction: Done By: Hisham Al-Omoush Mohammed Ali Supervised By: DR. Omar MansourDocument30 pagesSmall Bowel Obstruction: Done By: Hisham Al-Omoush Mohammed Ali Supervised By: DR. Omar MansourhalearnNo ratings yet
- Adhesive Small Bowel Adhesions Obstruction: Evolutions in Diagnosis, Management and PreventionDocument24 pagesAdhesive Small Bowel Adhesions Obstruction: Evolutions in Diagnosis, Management and PreventionEunikeSetiyantoWijayaNo ratings yet
- Colonoscopi IndicationDocument26 pagesColonoscopi IndicationTony HardianNo ratings yet
- Amputation: Istan I IrsanDocument40 pagesAmputation: Istan I IrsanTony HardianNo ratings yet
- Duodenal InjuryDocument54 pagesDuodenal InjuryTony HardianNo ratings yet
- Quickdash Scoring System: The Quickdash Outcome Measure: Scoring E-Tool For Use by CliniciansDocument1 pageQuickdash Scoring System: The Quickdash Outcome Measure: Scoring E-Tool For Use by CliniciansTony HardianNo ratings yet
- Practical 12. ReuploadDocument13 pagesPractical 12. Reuploadhawaalia534No ratings yet
- 20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Document1 page20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Ifan JayusdianNo ratings yet
- The Progression From Acute To Chronic Pain: Patricia Lavand'hommeDocument6 pagesThe Progression From Acute To Chronic Pain: Patricia Lavand'hommemaritzabericesNo ratings yet
- SCMHRD SM-5Document49 pagesSCMHRD SM-5ruchit2809100% (1)
- Alyssa Abler ApplicationDocument4 pagesAlyssa Abler Applicationapi-431765232No ratings yet
- Gastritis PDFDocument6 pagesGastritis PDFsrimardiahkusumaNo ratings yet
- Man Power Planning FileDocument5 pagesMan Power Planning FileMukesh KumarNo ratings yet
- Atropine Sulfate Drug STudyDocument2 pagesAtropine Sulfate Drug STudyLiway100% (1)
- Sample PRC Form of MeDocument6 pagesSample PRC Form of Melym13_john246981No ratings yet
- BCC, Laboratory Specimens and Microscopy, MLT 1040, Chapter 11 QUESTIONSDocument12 pagesBCC, Laboratory Specimens and Microscopy, MLT 1040, Chapter 11 QUESTIONSalphacetaNo ratings yet
- Administration of An Enema: Prepared By: Salwa MaghrabiDocument16 pagesAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlNo ratings yet
- Colonoscopy: Dr. Aries Budianto, SPB (K) BDDocument52 pagesColonoscopy: Dr. Aries Budianto, SPB (K) BDRisal WintokoNo ratings yet
- PBL Report 3 FixDocument24 pagesPBL Report 3 FixtiwiNo ratings yet
- VEDA Patient Medical History Form - LongDocument3 pagesVEDA Patient Medical History Form - LongyaddNo ratings yet
- Armamentarium 5Document42 pagesArmamentarium 5Helen Reyes HallareNo ratings yet
- Ultrasound With Shearwave Elastography - Acuson JuniperDocument6 pagesUltrasound With Shearwave Elastography - Acuson Juniperharis shahNo ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- Reproductive Disorders in The Dog and Bitch With Genetic ConcernsDocument5 pagesReproductive Disorders in The Dog and Bitch With Genetic ConcernsLuis WolfNo ratings yet
- Final Coaching - Obgyne 2022Document7 pagesFinal Coaching - Obgyne 2022Jhon PauloNo ratings yet
- Alternative Medicine Council OF Nigeria Inducts MembersDocument2 pagesAlternative Medicine Council OF Nigeria Inducts MembersGILBERTNo ratings yet
- Jennifer Fine - Nursing ResumeDocument2 pagesJennifer Fine - Nursing Resumeapi-383995637No ratings yet
- Procedure File M.S.NDocument11 pagesProcedure File M.S.NShalabh JoharyNo ratings yet
- AMR Guideline7001495889Document64 pagesAMR Guideline7001495889Drkrantianand Anand100% (1)
- 308-Article Text-1214-1-10-20200312Document6 pages308-Article Text-1214-1-10-20200312kintan fadilahNo ratings yet
- PEDocument34 pagesPEbrigette_lagatNo ratings yet
- Nonsurgical Cosmetic Procedures For Men Trends and Technique ConsiderationsDocument11 pagesNonsurgical Cosmetic Procedures For Men Trends and Technique ConsiderationsImanuel CristiantoNo ratings yet
- Fetal MonitoringDocument6 pagesFetal MonitoringRraouzmaaliNo ratings yet


























































































Download as pptx, pdf, or txt
You might also like
- Pedia 2.1 - Pediatric History (Vision) PDFDocument5 pagesPedia 2.1 - Pediatric History (Vision) PDFKaren ValdezNo ratings yet
- Pelayanan Digestif November 2021Document12 pagesPelayanan Digestif November 2021ari irawanNo ratings yet
- Foetal Organ Trafficking in The USDocument5 pagesFoetal Organ Trafficking in The USSister RosettaNo ratings yet
- Pande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byDocument32 pagesPande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byanon_550250832100% (1)
- Slide Jurnal BTKVDocument14 pagesSlide Jurnal BTKVVistaririnNo ratings yet
- Retractile TestisDocument7 pagesRetractile TestisAhmad Rahmat Ramadhan TantuNo ratings yet
- Fusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelainDocument7 pagesFusion of Modern and Ancient: Feldspathic/refractory Veneers Using Zirconia PorcelaintarekrabiNo ratings yet
- Partograph: Jillian A. Bejoc, MSN, RNDocument44 pagesPartograph: Jillian A. Bejoc, MSN, RNJiezl Abellano AfinidadNo ratings yet
- Visceral Leishmaniasis RecordedDocument19 pagesVisceral Leishmaniasis RecordedFemale calmNo ratings yet
- HERNIORRAPHY (Hernioplasty)Document37 pagesHERNIORRAPHY (Hernioplasty)Aldo AtjehNo ratings yet
- Chapter 36 - Visceral Leishmaniasis and TrypanosomiasisDocument99 pagesChapter 36 - Visceral Leishmaniasis and TrypanosomiasisHyny P'gallaNo ratings yet
- LumbotomiDocument14 pagesLumbotomiazka novriandiNo ratings yet
- Tinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus DecubitusDocument6 pagesTinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus Decubitusrinaldy prayudhiaNo ratings yet
- Chest TubeDocument8 pagesChest TubeTaufik Nur YahyaNo ratings yet
- Jurnal BTKV Herman 1Document11 pagesJurnal BTKV Herman 1Elyas MuhammadNo ratings yet
- Nephrostomy - DR Christopher WattsDocument39 pagesNephrostomy - DR Christopher WattsNidaChoerunnisa100% (1)
- Tg13: Updated Tokyo Guidelinesfor Acute CholecystitisDocument59 pagesTg13: Updated Tokyo Guidelinesfor Acute CholecystitisDeoValendraNo ratings yet
- AdhesiolisisDocument22 pagesAdhesiolisisRisal WintokoNo ratings yet
- BedahDocument139 pagesBedahLunaFia100% (1)
- WIFI Score For Diabetes Foot UlcerDocument17 pagesWIFI Score For Diabetes Foot Ulcertonylee24100% (1)
- Choledochal Cyst: Ronak Patel, DO PGY-3Document11 pagesCholedochal Cyst: Ronak Patel, DO PGY-3Ronak PatelNo ratings yet
- Akses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaDocument28 pagesAkses Vena Central: Anestesiologi Dan Reanimasi RSUD TasikmalayaSaeful AmbariNo ratings yet
- Terapi Cairan: Jayapura General Hospital Dept Anesthesiology & Reanimation, Cenderawasih University, School of MedicineDocument31 pagesTerapi Cairan: Jayapura General Hospital Dept Anesthesiology & Reanimation, Cenderawasih University, School of Medicinehandayani nurfitrianaNo ratings yet
- Non Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019Document50 pagesNon Muscle Invasive Bladder Cancer - EAU Full Guidelines 2019peroksidaseNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Wound Healing Normal and Abnormal Mechanisms and Closure TechniquesDocument40 pagesWound Healing Normal and Abnormal Mechanisms and Closure TechniquesAhmad Fakhrozi Helmi100% (1)
- Duodenal InjuryDocument54 pagesDuodenal InjuryTony HardianNo ratings yet
- Catatan DSTC CourseDocument3 pagesCatatan DSTC CourseHanny FadhilaNo ratings yet
- Icd 9 Obstetri N Gynek Plus TindakanDocument4 pagesIcd 9 Obstetri N Gynek Plus TindakanMimi Nanda Miranda AnastasiaNo ratings yet
- HerniaDocument61 pagesHerniaAhmed HassanNo ratings yet
- LONG CASE Luka BakarDocument16 pagesLONG CASE Luka BakarAfiazka LuthfitaNo ratings yet
- Colonoscopy CecilDocument14 pagesColonoscopy Cecilyaba100% (1)
- Rangkuman Salter Bab 14Document64 pagesRangkuman Salter Bab 14Febee NathaliaNo ratings yet
- Cara Mengukur Tekanan IntrakompartemenDocument2 pagesCara Mengukur Tekanan Intrakompartemenfatimah putriNo ratings yet
- JAAOS-Management of Hemorrhage in Life-Threatening Pelvic Fracture 162Document11 pagesJAAOS-Management of Hemorrhage in Life-Threatening Pelvic Fracture 162Enny Yunita HariantiNo ratings yet
- Tracheostomy: Berlian Chevi A. 20184010030Document26 pagesTracheostomy: Berlian Chevi A. 20184010030Berlian Chevi e'Xgepz ThrearsansNo ratings yet
- Dr. Kiki - Pengantar Trauma UpdateDocument20 pagesDr. Kiki - Pengantar Trauma UpdateRsud Malinau Ppk Blud100% (1)
- Shock Management, by Ayman RawehDocument15 pagesShock Management, by Ayman RawehaymxNo ratings yet
- Diabetes Mellitus Pada Anak KuliahDocument51 pagesDiabetes Mellitus Pada Anak KuliahNisha AnggiaNo ratings yet
- Trauma - Pediatric TraumaDocument20 pagesTrauma - Pediatric TraumaLukman NurfauziNo ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Oeis SyndromeDocument9 pagesOeis SyndromeADEENo ratings yet
- Total Penectomy Urooncology 12thDocument10 pagesTotal Penectomy Urooncology 12thdr. Joko WibowoNo ratings yet
- Syok Hypovolemik-IH FK UMSU2012Document45 pagesSyok Hypovolemik-IH FK UMSU2012Ratika Ayu PiliangNo ratings yet
- (Upgraded) BDH6 - Emergency Trauma & Non Trauma UroDocument122 pages(Upgraded) BDH6 - Emergency Trauma & Non Trauma Uronabila safiraNo ratings yet
- Chronic Limb Threatening IschemiaDocument35 pagesChronic Limb Threatening Ischemiasifatullah khanNo ratings yet
- Fracture and Dislocation-Rahardyan Magetsari (2016) PDFDocument105 pagesFracture and Dislocation-Rahardyan Magetsari (2016) PDFRobertOktaChandraNo ratings yet
- Stoma Siting - Iful Syarif Al MunawiDocument17 pagesStoma Siting - Iful Syarif Al MunawiRamdhani MaulanaNo ratings yet
- Torsio Testis2016Document6 pagesTorsio Testis2016Patrico Rillah SetiawanNo ratings yet
- Acute Pancreatitis: Methas Arunnart MD. Songkhla HospitalDocument70 pagesAcute Pancreatitis: Methas Arunnart MD. Songkhla HospitalMohd ImranNo ratings yet
- Hirschsprung DiseaseDocument20 pagesHirschsprung DiseaseIyan AsianaNo ratings yet
- KARSINOMA TIROID ZakiDocument31 pagesKARSINOMA TIROID ZakiDenny LukasNo ratings yet
- Jurnal DigestiveDocument9 pagesJurnal DigestiveFrancesc OktofabregasNo ratings yet
- OsteosarkomaDocument2 pagesOsteosarkomaLinawati DLNo ratings yet
- Chronic Limb IschemiaDocument29 pagesChronic Limb IschemiaSadia NaveedNo ratings yet
- Tracheostomy: Indications and ProcedureDocument10 pagesTracheostomy: Indications and ProcedureAinur AbdrakhmanovaNo ratings yet
- CSP Groin LumpDocument39 pagesCSP Groin LumpFebby ShabrinaNo ratings yet
- Fistel Vesicovaginalis, Ureterocutaneous, Dan UreterorectalisDocument24 pagesFistel Vesicovaginalis, Ureterocutaneous, Dan Ureterorectalismizz_jcNo ratings yet
- Terapi PaliatifDocument46 pagesTerapi PaliatifViviViviNo ratings yet
- CSS Airway Management RickyDocument53 pagesCSS Airway Management RickyArtha PutuNo ratings yet
- 2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesDocument11 pages2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesOlteanu IonutNo ratings yet
- Wound HealingDocument62 pagesWound HealingRisPerdanaNo ratings yet
- Small Bowel Obstruction: Done By: Hisham Al-Omoush Mohammed Ali Supervised By: DR. Omar MansourDocument30 pagesSmall Bowel Obstruction: Done By: Hisham Al-Omoush Mohammed Ali Supervised By: DR. Omar MansourhalearnNo ratings yet
- Adhesive Small Bowel Adhesions Obstruction: Evolutions in Diagnosis, Management and PreventionDocument24 pagesAdhesive Small Bowel Adhesions Obstruction: Evolutions in Diagnosis, Management and PreventionEunikeSetiyantoWijayaNo ratings yet
- Colonoscopi IndicationDocument26 pagesColonoscopi IndicationTony HardianNo ratings yet
- Amputation: Istan I IrsanDocument40 pagesAmputation: Istan I IrsanTony HardianNo ratings yet
- Duodenal InjuryDocument54 pagesDuodenal InjuryTony HardianNo ratings yet
- Quickdash Scoring System: The Quickdash Outcome Measure: Scoring E-Tool For Use by CliniciansDocument1 pageQuickdash Scoring System: The Quickdash Outcome Measure: Scoring E-Tool For Use by CliniciansTony HardianNo ratings yet
- Practical 12. ReuploadDocument13 pagesPractical 12. Reuploadhawaalia534No ratings yet
- 20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Document1 page20.daftar Kuantitas Dan Harga Produk Alat Kesehatan 2020 (Ok)Ifan JayusdianNo ratings yet
- The Progression From Acute To Chronic Pain: Patricia Lavand'hommeDocument6 pagesThe Progression From Acute To Chronic Pain: Patricia Lavand'hommemaritzabericesNo ratings yet
- SCMHRD SM-5Document49 pagesSCMHRD SM-5ruchit2809100% (1)
- Alyssa Abler ApplicationDocument4 pagesAlyssa Abler Applicationapi-431765232No ratings yet
- Gastritis PDFDocument6 pagesGastritis PDFsrimardiahkusumaNo ratings yet
- Man Power Planning FileDocument5 pagesMan Power Planning FileMukesh KumarNo ratings yet
- Atropine Sulfate Drug STudyDocument2 pagesAtropine Sulfate Drug STudyLiway100% (1)
- Sample PRC Form of MeDocument6 pagesSample PRC Form of Melym13_john246981No ratings yet
- BCC, Laboratory Specimens and Microscopy, MLT 1040, Chapter 11 QUESTIONSDocument12 pagesBCC, Laboratory Specimens and Microscopy, MLT 1040, Chapter 11 QUESTIONSalphacetaNo ratings yet
- Administration of An Enema: Prepared By: Salwa MaghrabiDocument16 pagesAdministration of An Enema: Prepared By: Salwa MaghrabiAnonymous 1EoKWlNo ratings yet
- Colonoscopy: Dr. Aries Budianto, SPB (K) BDDocument52 pagesColonoscopy: Dr. Aries Budianto, SPB (K) BDRisal WintokoNo ratings yet
- PBL Report 3 FixDocument24 pagesPBL Report 3 FixtiwiNo ratings yet
- VEDA Patient Medical History Form - LongDocument3 pagesVEDA Patient Medical History Form - LongyaddNo ratings yet
- Armamentarium 5Document42 pagesArmamentarium 5Helen Reyes HallareNo ratings yet
- Ultrasound With Shearwave Elastography - Acuson JuniperDocument6 pagesUltrasound With Shearwave Elastography - Acuson Juniperharis shahNo ratings yet
- OBM752 HM Unit-IV NotesDocument34 pagesOBM752 HM Unit-IV NotesRajanNo ratings yet
- Reproductive Disorders in The Dog and Bitch With Genetic ConcernsDocument5 pagesReproductive Disorders in The Dog and Bitch With Genetic ConcernsLuis WolfNo ratings yet
- Final Coaching - Obgyne 2022Document7 pagesFinal Coaching - Obgyne 2022Jhon PauloNo ratings yet
- Alternative Medicine Council OF Nigeria Inducts MembersDocument2 pagesAlternative Medicine Council OF Nigeria Inducts MembersGILBERTNo ratings yet
- Jennifer Fine - Nursing ResumeDocument2 pagesJennifer Fine - Nursing Resumeapi-383995637No ratings yet
- Procedure File M.S.NDocument11 pagesProcedure File M.S.NShalabh JoharyNo ratings yet
- AMR Guideline7001495889Document64 pagesAMR Guideline7001495889Drkrantianand Anand100% (1)
- 308-Article Text-1214-1-10-20200312Document6 pages308-Article Text-1214-1-10-20200312kintan fadilahNo ratings yet
- PEDocument34 pagesPEbrigette_lagatNo ratings yet
- Nonsurgical Cosmetic Procedures For Men Trends and Technique ConsiderationsDocument11 pagesNonsurgical Cosmetic Procedures For Men Trends and Technique ConsiderationsImanuel CristiantoNo ratings yet
- Fetal MonitoringDocument6 pagesFetal MonitoringRraouzmaaliNo ratings yet