Download as ppt, pdf, or txt
You might also like
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDocument22 pagesAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraNo ratings yet
- Acute Kidney InjuryDocument42 pagesAcute Kidney InjurysushmaNo ratings yet
- Acute Kidney Injury (AKI) : Departemen Penyakit DalamDocument43 pagesAcute Kidney Injury (AKI) : Departemen Penyakit DalamFitria Dewi LestariNo ratings yet
- Acute Kidney Injury (AKI) : Vivian PhanDocument15 pagesAcute Kidney Injury (AKI) : Vivian PhanRenzo HerreraNo ratings yet
- Insuficienta Renala Acuta: Actualitati Patogenice Si de TratamentDocument83 pagesInsuficienta Renala Acuta: Actualitati Patogenice Si de TratamentAnodine Daliko MarkovnaNo ratings yet
- Acute Renal FailureDocument41 pagesAcute Renal FailureShams Ul HaqNo ratings yet
- ACUTE KIDNEY INJURY. 2016m UNISMUHDocument26 pagesACUTE KIDNEY INJURY. 2016m UNISMUHWhulandary DyaswaraNo ratings yet
- Acute Kidney Injury: Syakib BakriDocument46 pagesAcute Kidney Injury: Syakib BakriBhisma D. SyaputraNo ratings yet
- 10 Kidneys 2017 PDFDocument42 pages10 Kidneys 2017 PDFSajid AhmadNo ratings yet
- Drugs Therapy For Kidney: Budi RaharjoDocument33 pagesDrugs Therapy For Kidney: Budi RaharjoNurul MasyithahNo ratings yet
- 11.0 Acute Kidney InjuryDocument26 pages11.0 Acute Kidney InjuryHeny KsNo ratings yet
- Acute Kidney InjuryDocument62 pagesAcute Kidney InjuryApidha KartinasariNo ratings yet
- 16 - RE - Acute Kidney InjuryDocument8 pages16 - RE - Acute Kidney Injury078229933aaNo ratings yet
- Acute Kidney InjuryDocument16 pagesAcute Kidney InjuryPutrii Rahayu Sriikandi100% (1)
- AKI MBCHB VDocument64 pagesAKI MBCHB VSsenyonga DominicNo ratings yet
- 15.kid Func TestDocument31 pages15.kid Func TestSubhi MishraNo ratings yet
- Gagal Ginjal Akut Pada AnakDocument37 pagesGagal Ginjal Akut Pada AnakNycoNo ratings yet
- Acute Kidney InjuryDocument26 pagesAcute Kidney InjuryUmmuhani AbubakarNo ratings yet
- IraDocument53 pagesIraadelinamihaela7No ratings yet
- Kidney DiseasesDocument45 pagesKidney DiseasesSai ViswasNo ratings yet
- Renal FunctionsDocument30 pagesRenal FunctionsJay Andrea Vea Israel100% (1)
- Tatalaksana Terkini Cedera Ginjal AkutDocument25 pagesTatalaksana Terkini Cedera Ginjal AkutSulistyawati WrimunNo ratings yet
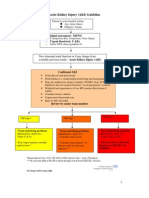
- Acute Kidney Injury (AKI) Guideline: - Initial Assessment: MEWSDocument2 pagesAcute Kidney Injury (AKI) Guideline: - Initial Assessment: MEWSMichael Nabil ShakerNo ratings yet
- 2 - Diagnostic AKI in ICU From KDIGO To BlomakerDocument80 pages2 - Diagnostic AKI in ICU From KDIGO To Blomakerhartanto_budi6222No ratings yet
- Renal Function TestsDocument38 pagesRenal Function TestsDr Abhinav Manish MDNo ratings yet
- RTC Acute Renal FailureDocument24 pagesRTC Acute Renal FailureVIDYANo ratings yet
- Kidney Emergency: M. Syamsul BakhriDocument30 pagesKidney Emergency: M. Syamsul BakhrierahadeNo ratings yet
- Acute Kidney InjuryDocument43 pagesAcute Kidney InjuryIwan ToniroNo ratings yet
- Approach To Acute Kidney InjuryDocument44 pagesApproach To Acute Kidney InjuryKue GosongNo ratings yet
- Renal FunctionDocument20 pagesRenal FunctionBatrisyia BalqisNo ratings yet
- Acute Renal Failure Lecture 1 Critical Care NursingDocument52 pagesAcute Renal Failure Lecture 1 Critical Care NursingDina Rasmita100% (2)
- Acute Renal Failure and TreatmentDocument103 pagesAcute Renal Failure and TreatmentNathan AsinasNo ratings yet
- Acute Kidney Injury (AKI) : Bagian Ginjal Hipertensi, Bagian Ilmu Penyakit Dalam FK Unand / RSUP Dr.M.Djamil PadangDocument19 pagesAcute Kidney Injury (AKI) : Bagian Ginjal Hipertensi, Bagian Ilmu Penyakit Dalam FK Unand / RSUP Dr.M.Djamil PadangfrisyaNo ratings yet
- L4 KFTsDocument4 pagesL4 KFTsRobin TikhatriNo ratings yet
- Mechanism of Urine Production. Urine Composition in Health and Pathologies. Biochemistry of Water and Salts TurnoverDocument73 pagesMechanism of Urine Production. Urine Composition in Health and Pathologies. Biochemistry of Water and Salts TurnoverRAJA RAJANNo ratings yet
- Acute Kidney Injury:: A Brief OutlineDocument48 pagesAcute Kidney Injury:: A Brief OutlinehanaNo ratings yet
- 1 Acute Renal FailureDocument65 pages1 Acute Renal FailureDammaqsaa W BiyyanaaNo ratings yet
- Renal Function TestDocument36 pagesRenal Function TestPoomuhi sathasivamNo ratings yet
- Chapter 43: Assessment of Renal and Urinary Tract Function: SodiumDocument9 pagesChapter 43: Assessment of Renal and Urinary Tract Function: SodiumBuddy PageNo ratings yet
- Renal Function TestsDocument31 pagesRenal Function TestsPhysiology by Dr RaghuveerNo ratings yet
- Renal Function TestsDocument43 pagesRenal Function TestsAbdulelah MurshidNo ratings yet
- Clinical Chemistry Renal FunctionDocument20 pagesClinical Chemistry Renal FunctionNida RidzuanNo ratings yet
- Acute Renal Failure: Dr. Rebecca JacobDocument6 pagesAcute Renal Failure: Dr. Rebecca JacobRevalitha PutriNo ratings yet
- Modul 7 Kegawatan Ginjal AnakDocument24 pagesModul 7 Kegawatan Ginjal AnakSanti IskandarNo ratings yet
- 6 To 12 Hours. For 12 Hours For 24 HoursDocument3 pages6 To 12 Hours. For 12 Hours For 24 HoursMohamad AbdelkhalikNo ratings yet
- AKI For Diploma Modified 2024Document33 pagesAKI For Diploma Modified 2024wesam.uv55No ratings yet
- Gangguan Ginjal AkutDocument29 pagesGangguan Ginjal Akutb3djo_76No ratings yet
- The Clinical Biochemistry of Kidney Functions: 2019 DR Boldizsár CZÉHDocument46 pagesThe Clinical Biochemistry of Kidney Functions: 2019 DR Boldizsár CZÉHJACOB FRANCISNo ratings yet
- AKIDocument23 pagesAKInadddNo ratings yet
- Liver Disease and Complications StudentsDocument2 pagesLiver Disease and Complications Studentsapi-660408385No ratings yet
- Gambaran Dari: Acute Kidney Injury (Aki) : Dr. Hasan BasriDocument22 pagesGambaran Dari: Acute Kidney Injury (Aki) : Dr. Hasan BasriLiana Ika SuwandyNo ratings yet
- Acute Renal Failure or Acute Kidney InjuryDocument3 pagesAcute Renal Failure or Acute Kidney InjuryHemanth PrakashNo ratings yet
- Diagnosis Aki Dan CKDDocument39 pagesDiagnosis Aki Dan CKDEly Kartika100% (1)
- Review of LaboratoryDocument48 pagesReview of LaboratoryIkhar RidhoNo ratings yet
- CKD EsrdDocument83 pagesCKD EsrdRita Lakhani100% (1)
- Acute Kidney Injury (AKI) : Haerani Rasyid FK Unhas 2016Document46 pagesAcute Kidney Injury (AKI) : Haerani Rasyid FK Unhas 2016Ana Yusriana AzzahraNo ratings yet
- Chronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDDocument32 pagesChronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDErryz JogjuzzNo ratings yet
- Biohemija Bubrega2011Document94 pagesBiohemija Bubrega2011Dejan Todorovic100% (1)
- 1.2 Cardinal Manifestations of Renal Disease DR MoraDocument36 pages1.2 Cardinal Manifestations of Renal Disease DR MoraJewelNo ratings yet
- Urinary Stones: Medical and Surgical ManagementFrom EverandUrinary Stones: Medical and Surgical ManagementMichael GrassoNo ratings yet