
Post Abortion Care
Post Abortion Care
You might also like
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Obstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayDocument35 pagesObstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayKutumela MolebogengNo ratings yet
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Post Partum HemorhageDocument7 pagesPost Partum HemorhageLithiya JoseNo ratings yet
- Pregnancy Induced HypertensionDocument21 pagesPregnancy Induced HypertensionLorren Frances Marie CalsarinNo ratings yet
- Instrumental DeliveryDocument25 pagesInstrumental DeliveryAhmed ElmohandesNo ratings yet
- Practice Essentials: DefinitionsDocument5 pagesPractice Essentials: DefinitionsNovita sariNo ratings yet
- Perineal TearDocument9 pagesPerineal Teardg_tajudinNo ratings yet
- Lecture Notes On AphDocument41 pagesLecture Notes On AphEyob MizanNo ratings yet
- Obstetrical EmergencyDocument41 pagesObstetrical EmergencyDrPreeti Thakur ChouhanNo ratings yet
- Vacuum DeliveryDocument3 pagesVacuum DeliveryKinjal Mistri100% (2)
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- Normal DeliveryDocument41 pagesNormal DeliveryAliNo ratings yet
- Diagnosis of PregnancyDocument26 pagesDiagnosis of PregnancyRamona GaluNo ratings yet
- Puerperal PyrexiaDocument20 pagesPuerperal Pyrexiaهلا اكرم عقل طميزهNo ratings yet
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Induction and AugmentationDocument23 pagesInduction and AugmentationMerry ZewduNo ratings yet
- Physiology of Lactation and PurpuriumDocument37 pagesPhysiology of Lactation and Purpuriumvarshasharma05No ratings yet
- Postmature Infants 1Document13 pagesPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Prolonged PregnancyDocument41 pagesProlonged PregnancyArif Febrianto100% (1)
- 3rd Stage of LabourDocument16 pages3rd Stage of LabourVaibhav KrishnaNo ratings yet
- Management of Placenta Previa - UpToDateDocument15 pagesManagement of Placenta Previa - UpToDateJuanPulgarínNo ratings yet
- Essential Newborn CareDocument5 pagesEssential Newborn CareElaine Iris AbastaNo ratings yet
- Diagnosis of Pregnancy: Presented By: Ms. Vruti Patel, Lecturer, SCNDocument22 pagesDiagnosis of Pregnancy: Presented By: Ms. Vruti Patel, Lecturer, SCNvrutipatel100% (1)
- Gravida and Parity Practice QuestionsDocument1 pageGravida and Parity Practice QuestionsHazelynne MamucudNo ratings yet
- Pre-Eclampsia and EclampsiaDocument21 pagesPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- Multiple PregnancyDocument21 pagesMultiple PregnancyMazlina Maidin100% (1)
- Abruption PacentaDocument6 pagesAbruption PacentaKondapavuluru JyothiNo ratings yet
- Care of The Pregnant Woman With HIVDocument34 pagesCare of The Pregnant Woman With HIVJenelle Melinda TullochNo ratings yet
- PREMATURITYDocument40 pagesPREMATURITYBlykeBantuganNo ratings yet
- 3rd Stage ComplicationsDocument84 pages3rd Stage ComplicationsDream100% (1)
- LSCS PRESENTATIONDocument13 pagesLSCS PRESENTATIONMichael AdkinsNo ratings yet
- Uterine Malformations PDFDocument6 pagesUterine Malformations PDFsaritha OrugantiNo ratings yet
- PartogramDocument20 pagesPartogramKasumba ChandaNo ratings yet
- Puerperium & Puerperal SepsisDocument15 pagesPuerperium & Puerperal SepsisMohammad HafizNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky Amalia100% (1)
- APH&PPHDocument77 pagesAPH&PPHKåbåñå TürüñåNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Physiologic Changes PregnancyDocument53 pagesPhysiologic Changes PregnancyDeedong Zydee100% (1)
- Management of Third Stage of LaborDocument6 pagesManagement of Third Stage of LaborYogesh BharankarNo ratings yet
- Reposition of Inverted UterusDocument5 pagesReposition of Inverted Uterusshraddha vermaNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)
- Obstetric and Gynaecological Nursing IInd YearDocument8 pagesObstetric and Gynaecological Nursing IInd YearsanthiyasandyNo ratings yet
- 5 Asphyxia NeonetrumDocument27 pages5 Asphyxia NeonetrumRana VandanaNo ratings yet
- HIV in Mothers and ChildrenDocument90 pagesHIV in Mothers and Childrenabubaker100% (1)
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- Labour, Neonate & PuerperiumDocument550 pagesLabour, Neonate & PuerperiumJonah nyachaeNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- AbortionDocument62 pagesAbortionRaj KumarNo ratings yet
- Antenatal PreparationDocument26 pagesAntenatal Preparationvaishali TMU studentNo ratings yet
- Management of A Case of Hydramnios and Oligohydramnio1Document12 pagesManagement of A Case of Hydramnios and Oligohydramnio1Easter Soma HageNo ratings yet
- Bleeding in Early PregnancyDocument20 pagesBleeding in Early Pregnancynanapet80No ratings yet
- PARTOGRAMDocument17 pagesPARTOGRAMKrutthivaasa PriyaNo ratings yet
- 17 Normal PuerperiumDocument12 pages17 Normal PuerperiumAhmed TarigNo ratings yet
- Postpartum ComplicationsDocument26 pagesPostpartum ComplicationsSharinah Ainee Sabalburo PasandalanNo ratings yet
- Exercises To Facilitate Change of Baby's Position From Breech To CephalicDocument3 pagesExercises To Facilitate Change of Baby's Position From Breech To CephalicaziskarnNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Emotions FinalDocument7 pagesEmotions FinalNatukunda DianahNo ratings yet
- Definition of TermsDocument14 pagesDefinition of TermsNatukunda DianahNo ratings yet
- The Nervous SystemDocument86 pagesThe Nervous SystemNatukunda Dianah100% (1)
- Cognitive DevDocument6 pagesCognitive DevNatukunda DianahNo ratings yet
- Special SensesDocument4 pagesSpecial SensesNatukunda DianahNo ratings yet
- Intro To Communicable Diseases-1Document101 pagesIntro To Communicable Diseases-1Natukunda DianahNo ratings yet
- SkinDocument36 pagesSkinNatukunda DianahNo ratings yet
- Parmacology OneDocument44 pagesParmacology OneNatukunda DianahNo ratings yet
- Special Senses TestDocument47 pagesSpecial Senses TestNatukunda DianahNo ratings yet
- Physiology MCQsDocument7 pagesPhysiology MCQsNatukunda DianahNo ratings yet
- Oliva ch13Document79 pagesOliva ch13Natukunda DianahNo ratings yet
- HearingDocument4 pagesHearingNatukunda DianahNo ratings yet
- Faeco-Oral DiseasesDocument46 pagesFaeco-Oral DiseasesNatukunda DianahNo ratings yet
- Human Resource Structure For BTVET INSTITUTIONSDocument21 pagesHuman Resource Structure For BTVET INSTITUTIONSNatukunda DianahNo ratings yet
- Culture Practices, Gender and Impact On HealthDocument31 pagesCulture Practices, Gender and Impact On HealthNatukunda Dianah100% (1)
- Conceptualization and Definition of A CurriculumDocument23 pagesConceptualization and Definition of A CurriculumNatukunda Dianah100% (1)
- Gender Identity and Gender Roles: by James KatereggaDocument24 pagesGender Identity and Gender Roles: by James KatereggaNatukunda DianahNo ratings yet
- Proffessional Ethics in Medical Education GME 6205 Teachers Proffesional Ethics & Medical Proffesional EthicsDocument13 pagesProffessional Ethics in Medical Education GME 6205 Teachers Proffesional Ethics & Medical Proffesional EthicsNatukunda DianahNo ratings yet
- Female Genital MutilationDocument14 pagesFemale Genital MutilationNatukunda DianahNo ratings yet
- I Notes: Cornea: February 2014Document7 pagesI Notes: Cornea: February 2014Natukunda DianahNo ratings yet
- UoE IADEngage FeedbackAssess A5 V4 WEBDocument12 pagesUoE IADEngage FeedbackAssess A5 V4 WEBNatukunda DianahNo ratings yet
- Red Eye The Role of Primary CareDocument16 pagesRed Eye The Role of Primary CareNatukunda DianahNo ratings yet
- Tom Brown: Anagement in The 21St EnturyDocument4 pagesTom Brown: Anagement in The 21St EnturyNatukunda DianahNo ratings yet
- Congenital Heart Disease Lecture NotesDocument8 pagesCongenital Heart Disease Lecture NotesNatukunda DianahNo ratings yet
- Paed Prelim SummaryDocument10 pagesPaed Prelim SummaryNatukunda DianahNo ratings yet
- Use of Maternal and Neonatal Health Services Associated With Neonatal Death in MyanmarDocument44 pagesUse of Maternal and Neonatal Health Services Associated With Neonatal Death in MyanmarNatukunda DianahNo ratings yet
- BMJGH 2019 June 4 3 Inline Supplementary Material 1 PDFDocument15 pagesBMJGH 2019 June 4 3 Inline Supplementary Material 1 PDFNatukunda DianahNo ratings yet
- Original Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalDocument6 pagesOriginal Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalNatukunda DianahNo ratings yet
- Curriculum Development in Agricultural Education (AED 605) : Lecture Note OnDocument35 pagesCurriculum Development in Agricultural Education (AED 605) : Lecture Note OnNatukunda DianahNo ratings yet
- Feedback Ms-WordDocument10 pagesFeedback Ms-WordNatukunda DianahNo ratings yet
- Who, Whom, Which, Whose, That... : The Nurse Is in ICU Now. You Are Looking For HerDocument6 pagesWho, Whom, Which, Whose, That... : The Nurse Is in ICU Now. You Are Looking For HerYunita HarahapNo ratings yet
- A Cesarean SectionDocument9 pagesA Cesarean SectionmejulNo ratings yet
- 2022-23 OBG MMed 2 - 3btest 1 - KeyDocument12 pages2022-23 OBG MMed 2 - 3btest 1 - KeyKenneth ChandaNo ratings yet
- Ebola Virus DiseaseDocument41 pagesEbola Virus DiseaseAbshame T.No ratings yet
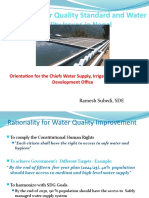
- NDWQS and Water Quality Issues in Nepal - SindhuliDocument41 pagesNDWQS and Water Quality Issues in Nepal - SindhuliBipin GyawaliNo ratings yet
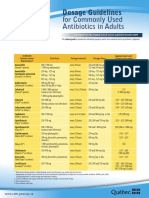
- CDM Antibio1 DosageGuidelines Adults enDocument2 pagesCDM Antibio1 DosageGuidelines Adults endwiNo ratings yet
- Group 4Document59 pagesGroup 4Esmel Jane Cañedo PeñaflorNo ratings yet
- Family PlanningDocument15 pagesFamily PlanningSiwani BarmaNo ratings yet
- Artigo de Opinião: Eu Estou Aí, Compondo o MundoDocument9 pagesArtigo de Opinião: Eu Estou Aí, Compondo o MundoHenrique BettinNo ratings yet
- Counseling For ObesityDocument52 pagesCounseling For ObesityAjithaNo ratings yet
- Self-Declaration Form - PHD Students - July 2021Document2 pagesSelf-Declaration Form - PHD Students - July 2021Pardha SaradhiNo ratings yet
- Covid Test-NegativeDocument2 pagesCovid Test-NegativeSuresh VarmaNo ratings yet
- Food Safety and Standards (Food or Health Supplements, Nutraceuticals, Foods For Special Dietary Uses, Foods For Special Medical Purpose, Functional Foods and Novel Food) Regulations, 2016Document131 pagesFood Safety and Standards (Food or Health Supplements, Nutraceuticals, Foods For Special Dietary Uses, Foods For Special Medical Purpose, Functional Foods and Novel Food) Regulations, 2016Latest Laws TeamNo ratings yet
- Introduction To EpidemiologyDocument15 pagesIntroduction To EpidemiologyNathnael Gebeyehu0% (1)
- Definitions of Occupational DiseasesDocument2 pagesDefinitions of Occupational DiseasesNoopur GandhiNo ratings yet
- HEALTH - Q3 PPT-MAPEH10 - Lesson 3 (Issues in The Implementation of Global Health Initiatives)Document18 pagesHEALTH - Q3 PPT-MAPEH10 - Lesson 3 (Issues in The Implementation of Global Health Initiatives)Lemuel Español Camus100% (3)
- Gambaran Status Gizi Pada Pasien Tuberkulosis Paru (TB Paru) Yang Menjalani Rawat Inap Di Rsud Arifin Achmad PekanbaruDocument33 pagesGambaran Status Gizi Pada Pasien Tuberkulosis Paru (TB Paru) Yang Menjalani Rawat Inap Di Rsud Arifin Achmad PekanbaruAmalia SuryaniNo ratings yet
- Bio Protein Plus HIV Study ResultsDocument5 pagesBio Protein Plus HIV Study ResultsRichard Beardsley Jr.No ratings yet
- Ru33sal3hm5tyreaybs2g4g4Document4 pagesRu33sal3hm5tyreaybs2g4g4okendroNo ratings yet
- Paul PitchfordDocument2 pagesPaul PitchfordloibalfNo ratings yet
- Diarrheal DiseaseDocument11 pagesDiarrheal DiseaseEbrahim El-sayedNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)Document18 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)subiNo ratings yet
- CA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Document38 pagesCA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Camilly CampanharoNo ratings yet
- PSM Supplement by DR Vivek JainDocument5 pagesPSM Supplement by DR Vivek JainVivek Jain100% (14)
- Restaurant Report Card: January 4, 2024Document4 pagesRestaurant Report Card: January 4, 2024KBTXNo ratings yet
- BRM Manual TemplateDocument36 pagesBRM Manual Templatepakmahmud100% (1)
- Linen and Laundry Pres IntroDocument5 pagesLinen and Laundry Pres IntroO.r. CadzNo ratings yet
- CertificateDocument1 pageCertificateNitin TayadeNo ratings yet
- Viral Hepatitis in ChildrenDocument15 pagesViral Hepatitis in ChildrenDr AnilNo ratings yet




















































































































Download as ppt, pdf, or txt
You might also like
- Partograph PPT 1Document55 pagesPartograph PPT 1Maria Lejani Terencio100% (1)
- Obstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayDocument35 pagesObstetric Emergencies and Anesthetic Management: Co-Ordinator: DR - Navab Singh (M.D.) Speaker: Dr. UdayKutumela MolebogengNo ratings yet
- An Update On Menopause ManagementDocument10 pagesAn Update On Menopause ManagementJuan FranciscoNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Post Partum HemorhageDocument7 pagesPost Partum HemorhageLithiya JoseNo ratings yet
- Pregnancy Induced HypertensionDocument21 pagesPregnancy Induced HypertensionLorren Frances Marie CalsarinNo ratings yet
- Instrumental DeliveryDocument25 pagesInstrumental DeliveryAhmed ElmohandesNo ratings yet
- Practice Essentials: DefinitionsDocument5 pagesPractice Essentials: DefinitionsNovita sariNo ratings yet
- Perineal TearDocument9 pagesPerineal Teardg_tajudinNo ratings yet
- Lecture Notes On AphDocument41 pagesLecture Notes On AphEyob MizanNo ratings yet
- Obstetrical EmergencyDocument41 pagesObstetrical EmergencyDrPreeti Thakur ChouhanNo ratings yet
- Vacuum DeliveryDocument3 pagesVacuum DeliveryKinjal Mistri100% (2)
- Polyhydramnios 10Document4 pagesPolyhydramnios 10hussain AltaherNo ratings yet
- Normal DeliveryDocument41 pagesNormal DeliveryAliNo ratings yet
- Diagnosis of PregnancyDocument26 pagesDiagnosis of PregnancyRamona GaluNo ratings yet
- Puerperal PyrexiaDocument20 pagesPuerperal Pyrexiaهلا اكرم عقل طميزهNo ratings yet
- Multiple PregnanciesDocument36 pagesMultiple PregnanciesBasudev ch100% (1)
- Obg Objective QuestionDocument1 pageObg Objective QuestionDESUN Nursing School100% (1)
- Induction and AugmentationDocument23 pagesInduction and AugmentationMerry ZewduNo ratings yet
- Physiology of Lactation and PurpuriumDocument37 pagesPhysiology of Lactation and Purpuriumvarshasharma05No ratings yet
- Postmature Infants 1Document13 pagesPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Prolonged PregnancyDocument41 pagesProlonged PregnancyArif Febrianto100% (1)
- 3rd Stage of LabourDocument16 pages3rd Stage of LabourVaibhav KrishnaNo ratings yet
- Management of Placenta Previa - UpToDateDocument15 pagesManagement of Placenta Previa - UpToDateJuanPulgarínNo ratings yet
- Essential Newborn CareDocument5 pagesEssential Newborn CareElaine Iris AbastaNo ratings yet
- Diagnosis of Pregnancy: Presented By: Ms. Vruti Patel, Lecturer, SCNDocument22 pagesDiagnosis of Pregnancy: Presented By: Ms. Vruti Patel, Lecturer, SCNvrutipatel100% (1)
- Gravida and Parity Practice QuestionsDocument1 pageGravida and Parity Practice QuestionsHazelynne MamucudNo ratings yet
- Pre-Eclampsia and EclampsiaDocument21 pagesPre-Eclampsia and EclampsiaTamratKelelegn100% (1)
- Multiple PregnancyDocument21 pagesMultiple PregnancyMazlina Maidin100% (1)
- Abruption PacentaDocument6 pagesAbruption PacentaKondapavuluru JyothiNo ratings yet
- Care of The Pregnant Woman With HIVDocument34 pagesCare of The Pregnant Woman With HIVJenelle Melinda TullochNo ratings yet
- PREMATURITYDocument40 pagesPREMATURITYBlykeBantuganNo ratings yet
- 3rd Stage ComplicationsDocument84 pages3rd Stage ComplicationsDream100% (1)
- LSCS PRESENTATIONDocument13 pagesLSCS PRESENTATIONMichael AdkinsNo ratings yet
- Uterine Malformations PDFDocument6 pagesUterine Malformations PDFsaritha OrugantiNo ratings yet
- PartogramDocument20 pagesPartogramKasumba ChandaNo ratings yet
- Puerperium & Puerperal SepsisDocument15 pagesPuerperium & Puerperal SepsisMohammad HafizNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky Amalia100% (1)
- APH&PPHDocument77 pagesAPH&PPHKåbåñå TürüñåNo ratings yet
- Understanding Multiple Pregnancy: Maternal & Fetal ComplicationsDocument69 pagesUnderstanding Multiple Pregnancy: Maternal & Fetal Complications966342No ratings yet
- Physiologic Changes PregnancyDocument53 pagesPhysiologic Changes PregnancyDeedong Zydee100% (1)
- Management of Third Stage of LaborDocument6 pagesManagement of Third Stage of LaborYogesh BharankarNo ratings yet
- Reposition of Inverted UterusDocument5 pagesReposition of Inverted Uterusshraddha vermaNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)
- Obstetric and Gynaecological Nursing IInd YearDocument8 pagesObstetric and Gynaecological Nursing IInd YearsanthiyasandyNo ratings yet
- 5 Asphyxia NeonetrumDocument27 pages5 Asphyxia NeonetrumRana VandanaNo ratings yet
- HIV in Mothers and ChildrenDocument90 pagesHIV in Mothers and Childrenabubaker100% (1)
- Prolonged Labor and Labor InductionDocument28 pagesProlonged Labor and Labor InductionNovia RizqiNo ratings yet
- Labour, Neonate & PuerperiumDocument550 pagesLabour, Neonate & PuerperiumJonah nyachaeNo ratings yet
- Bleeding During PregnancyDocument5 pagesBleeding During PregnancyMaryela Maceda GalozoNo ratings yet
- AbortionDocument62 pagesAbortionRaj KumarNo ratings yet
- Antenatal PreparationDocument26 pagesAntenatal Preparationvaishali TMU studentNo ratings yet
- Management of A Case of Hydramnios and Oligohydramnio1Document12 pagesManagement of A Case of Hydramnios and Oligohydramnio1Easter Soma HageNo ratings yet
- Bleeding in Early PregnancyDocument20 pagesBleeding in Early Pregnancynanapet80No ratings yet
- PARTOGRAMDocument17 pagesPARTOGRAMKrutthivaasa PriyaNo ratings yet
- 17 Normal PuerperiumDocument12 pages17 Normal PuerperiumAhmed TarigNo ratings yet
- Postpartum ComplicationsDocument26 pagesPostpartum ComplicationsSharinah Ainee Sabalburo PasandalanNo ratings yet
- Exercises To Facilitate Change of Baby's Position From Breech To CephalicDocument3 pagesExercises To Facilitate Change of Baby's Position From Breech To CephalicaziskarnNo ratings yet
- Fanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandFanconi Anemia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Role of Dietary Fibers and Nutraceuticals in Preventing DiseasesFrom EverandRole of Dietary Fibers and Nutraceuticals in Preventing DiseasesRating: 5 out of 5 stars5/5 (1)
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Emotions FinalDocument7 pagesEmotions FinalNatukunda DianahNo ratings yet
- Definition of TermsDocument14 pagesDefinition of TermsNatukunda DianahNo ratings yet
- The Nervous SystemDocument86 pagesThe Nervous SystemNatukunda Dianah100% (1)
- Cognitive DevDocument6 pagesCognitive DevNatukunda DianahNo ratings yet
- Special SensesDocument4 pagesSpecial SensesNatukunda DianahNo ratings yet
- Intro To Communicable Diseases-1Document101 pagesIntro To Communicable Diseases-1Natukunda DianahNo ratings yet
- SkinDocument36 pagesSkinNatukunda DianahNo ratings yet
- Parmacology OneDocument44 pagesParmacology OneNatukunda DianahNo ratings yet
- Special Senses TestDocument47 pagesSpecial Senses TestNatukunda DianahNo ratings yet
- Physiology MCQsDocument7 pagesPhysiology MCQsNatukunda DianahNo ratings yet
- Oliva ch13Document79 pagesOliva ch13Natukunda DianahNo ratings yet
- HearingDocument4 pagesHearingNatukunda DianahNo ratings yet
- Faeco-Oral DiseasesDocument46 pagesFaeco-Oral DiseasesNatukunda DianahNo ratings yet
- Human Resource Structure For BTVET INSTITUTIONSDocument21 pagesHuman Resource Structure For BTVET INSTITUTIONSNatukunda DianahNo ratings yet
- Culture Practices, Gender and Impact On HealthDocument31 pagesCulture Practices, Gender and Impact On HealthNatukunda Dianah100% (1)
- Conceptualization and Definition of A CurriculumDocument23 pagesConceptualization and Definition of A CurriculumNatukunda Dianah100% (1)
- Gender Identity and Gender Roles: by James KatereggaDocument24 pagesGender Identity and Gender Roles: by James KatereggaNatukunda DianahNo ratings yet
- Proffessional Ethics in Medical Education GME 6205 Teachers Proffesional Ethics & Medical Proffesional EthicsDocument13 pagesProffessional Ethics in Medical Education GME 6205 Teachers Proffesional Ethics & Medical Proffesional EthicsNatukunda DianahNo ratings yet
- Female Genital MutilationDocument14 pagesFemale Genital MutilationNatukunda DianahNo ratings yet
- I Notes: Cornea: February 2014Document7 pagesI Notes: Cornea: February 2014Natukunda DianahNo ratings yet
- UoE IADEngage FeedbackAssess A5 V4 WEBDocument12 pagesUoE IADEngage FeedbackAssess A5 V4 WEBNatukunda DianahNo ratings yet
- Red Eye The Role of Primary CareDocument16 pagesRed Eye The Role of Primary CareNatukunda DianahNo ratings yet
- Tom Brown: Anagement in The 21St EnturyDocument4 pagesTom Brown: Anagement in The 21St EnturyNatukunda DianahNo ratings yet
- Congenital Heart Disease Lecture NotesDocument8 pagesCongenital Heart Disease Lecture NotesNatukunda DianahNo ratings yet
- Paed Prelim SummaryDocument10 pagesPaed Prelim SummaryNatukunda DianahNo ratings yet
- Use of Maternal and Neonatal Health Services Associated With Neonatal Death in MyanmarDocument44 pagesUse of Maternal and Neonatal Health Services Associated With Neonatal Death in MyanmarNatukunda DianahNo ratings yet
- BMJGH 2019 June 4 3 Inline Supplementary Material 1 PDFDocument15 pagesBMJGH 2019 June 4 3 Inline Supplementary Material 1 PDFNatukunda DianahNo ratings yet
- Original Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalDocument6 pagesOriginal Article: Pregnancy Outcome Between Booked and Unbooked Cases in A Tertiary Level HospitalNatukunda DianahNo ratings yet
- Curriculum Development in Agricultural Education (AED 605) : Lecture Note OnDocument35 pagesCurriculum Development in Agricultural Education (AED 605) : Lecture Note OnNatukunda DianahNo ratings yet
- Feedback Ms-WordDocument10 pagesFeedback Ms-WordNatukunda DianahNo ratings yet
- Who, Whom, Which, Whose, That... : The Nurse Is in ICU Now. You Are Looking For HerDocument6 pagesWho, Whom, Which, Whose, That... : The Nurse Is in ICU Now. You Are Looking For HerYunita HarahapNo ratings yet
- A Cesarean SectionDocument9 pagesA Cesarean SectionmejulNo ratings yet
- 2022-23 OBG MMed 2 - 3btest 1 - KeyDocument12 pages2022-23 OBG MMed 2 - 3btest 1 - KeyKenneth ChandaNo ratings yet
- Ebola Virus DiseaseDocument41 pagesEbola Virus DiseaseAbshame T.No ratings yet
- NDWQS and Water Quality Issues in Nepal - SindhuliDocument41 pagesNDWQS and Water Quality Issues in Nepal - SindhuliBipin GyawaliNo ratings yet
- CDM Antibio1 DosageGuidelines Adults enDocument2 pagesCDM Antibio1 DosageGuidelines Adults endwiNo ratings yet
- Group 4Document59 pagesGroup 4Esmel Jane Cañedo PeñaflorNo ratings yet
- Family PlanningDocument15 pagesFamily PlanningSiwani BarmaNo ratings yet
- Artigo de Opinião: Eu Estou Aí, Compondo o MundoDocument9 pagesArtigo de Opinião: Eu Estou Aí, Compondo o MundoHenrique BettinNo ratings yet
- Counseling For ObesityDocument52 pagesCounseling For ObesityAjithaNo ratings yet
- Self-Declaration Form - PHD Students - July 2021Document2 pagesSelf-Declaration Form - PHD Students - July 2021Pardha SaradhiNo ratings yet
- Covid Test-NegativeDocument2 pagesCovid Test-NegativeSuresh VarmaNo ratings yet
- Food Safety and Standards (Food or Health Supplements, Nutraceuticals, Foods For Special Dietary Uses, Foods For Special Medical Purpose, Functional Foods and Novel Food) Regulations, 2016Document131 pagesFood Safety and Standards (Food or Health Supplements, Nutraceuticals, Foods For Special Dietary Uses, Foods For Special Medical Purpose, Functional Foods and Novel Food) Regulations, 2016Latest Laws TeamNo ratings yet
- Introduction To EpidemiologyDocument15 pagesIntroduction To EpidemiologyNathnael Gebeyehu0% (1)
- Definitions of Occupational DiseasesDocument2 pagesDefinitions of Occupational DiseasesNoopur GandhiNo ratings yet
- HEALTH - Q3 PPT-MAPEH10 - Lesson 3 (Issues in The Implementation of Global Health Initiatives)Document18 pagesHEALTH - Q3 PPT-MAPEH10 - Lesson 3 (Issues in The Implementation of Global Health Initiatives)Lemuel Español Camus100% (3)
- Gambaran Status Gizi Pada Pasien Tuberkulosis Paru (TB Paru) Yang Menjalani Rawat Inap Di Rsud Arifin Achmad PekanbaruDocument33 pagesGambaran Status Gizi Pada Pasien Tuberkulosis Paru (TB Paru) Yang Menjalani Rawat Inap Di Rsud Arifin Achmad PekanbaruAmalia SuryaniNo ratings yet
- Bio Protein Plus HIV Study ResultsDocument5 pagesBio Protein Plus HIV Study ResultsRichard Beardsley Jr.No ratings yet
- Ru33sal3hm5tyreaybs2g4g4Document4 pagesRu33sal3hm5tyreaybs2g4g4okendroNo ratings yet
- Paul PitchfordDocument2 pagesPaul PitchfordloibalfNo ratings yet
- Diarrheal DiseaseDocument11 pagesDiarrheal DiseaseEbrahim El-sayedNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)Document18 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangalore Annexure - Ii Name of The Candidate and Address (In Block Letters)subiNo ratings yet
- CA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Document38 pagesCA A Cancer J Clinicians - 2024 - Siegel - Cancer Statistics 2024Camilly CampanharoNo ratings yet
- PSM Supplement by DR Vivek JainDocument5 pagesPSM Supplement by DR Vivek JainVivek Jain100% (14)
- Restaurant Report Card: January 4, 2024Document4 pagesRestaurant Report Card: January 4, 2024KBTXNo ratings yet
- BRM Manual TemplateDocument36 pagesBRM Manual Templatepakmahmud100% (1)
- Linen and Laundry Pres IntroDocument5 pagesLinen and Laundry Pres IntroO.r. CadzNo ratings yet
- CertificateDocument1 pageCertificateNitin TayadeNo ratings yet
- Viral Hepatitis in ChildrenDocument15 pagesViral Hepatitis in ChildrenDr AnilNo ratings yet