Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Booty Boost Home Program - Vol 2Document5 pagesBooty Boost Home Program - Vol 2Elyse Sonson100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hoist Mi6 - Exercise - PosterDocument1 pageHoist Mi6 - Exercise - PosterBarry Ghotra100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Map Hand Washing SurgicalA3Document1 pageMap Hand Washing SurgicalA3Pankaj Babu SaxenaNo ratings yet
- Corelation SDH Brain AtrophyDocument16 pagesCorelation SDH Brain Atrophyselubung lineNo ratings yet
- Clinico-Pathological ConferenceDocument116 pagesClinico-Pathological Conferenceselubung lineNo ratings yet
- CPC MuhrojiDocument19 pagesCPC Muhrojiselubung lineNo ratings yet
- Revmar2013 Wr2 Ys1e Tulangfraktur VFDocument41 pagesRevmar2013 Wr2 Ys1e Tulangfraktur VFselubung lineNo ratings yet
- Sunaryo Hardjowijoto Division Uro Oncology Department of Urology Airlangga School of Medicine Dr. Sutomo Hospital SurabayaDocument20 pagesSunaryo Hardjowijoto Division Uro Oncology Department of Urology Airlangga School of Medicine Dr. Sutomo Hospital Surabayaselubung lineNo ratings yet
- Arnis SportDocument6 pagesArnis SportUwuuUNo ratings yet
- Kalinga State University Department of Physical Education 1st Semester, SY 2021-2022Document1 pageKalinga State University Department of Physical Education 1st Semester, SY 2021-2022WALLANG, Nicol B.No ratings yet
- The Equine Stay ApparatusDocument7 pagesThe Equine Stay ApparatusSavannah Simone Petrachenko100% (4)
- Chapter 20: Ankle Joint and Foot: General Anatomy QuestionsDocument11 pagesChapter 20: Ankle Joint and Foot: General Anatomy QuestionspoNo ratings yet
- Iii. Fundamental Positions of Arms and FeetDocument3 pagesIii. Fundamental Positions of Arms and Feetmochii100% (1)
- First Aid With LAF DR - IndahDocument32 pagesFirst Aid With LAF DR - IndahIndah Triayu IriantiNo ratings yet
- Congenital Vertical Talus Relevant AnatomyDocument5 pagesCongenital Vertical Talus Relevant AnatomyJohann Sebastian CruzNo ratings yet
- Shashankasana - Hare Posure & Balasana - Child's PostureDocument10 pagesShashankasana - Hare Posure & Balasana - Child's Posturegaya3mageshNo ratings yet
- Acara Sukan Bagi Kategori Umur 9 - 10Document21 pagesAcara Sukan Bagi Kategori Umur 9 - 10angNo ratings yet
- ANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Document3 pagesANAT1012.1019 Example Regional Lower Limb SAQ's - 2022Grace YNo ratings yet
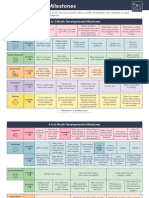
- Solid Starts - Developmental MilestonesDocument6 pagesSolid Starts - Developmental Milestonestohru89No ratings yet
- CTEVDocument24 pagesCTEVwildanmalikNo ratings yet
- 34 Pilates ExercisesDocument7 pages34 Pilates ExerciseskerryNo ratings yet
- Laboratory Ergonomics Checklist: (DOSH Registration)Document3 pagesLaboratory Ergonomics Checklist: (DOSH Registration)Bakhtiar DollahNo ratings yet
- Calf StrainDocument3 pagesCalf StrainCamden VistainNo ratings yet
- Pediatric Special TestDocument17 pagesPediatric Special TestMaesy LorenaNo ratings yet
- Pilates For Post-PregnancyDocument10 pagesPilates For Post-PregnancyGem Res MésNo ratings yet
- Limb Length DiscrepancyDocument75 pagesLimb Length DiscrepancyDavidBeatonComuladaNo ratings yet
- Caresole Review 2021: All You Need To Know and MoreDocument12 pagesCaresole Review 2021: All You Need To Know and MorePulkit sharmaNo ratings yet
- Efek Terapi Oksigen Hiperbarik (TOHB) Pada Penyembuhan Ulkus Kaki DM Tipe 2 Berdasarkan Skor PEDISDocument6 pagesEfek Terapi Oksigen Hiperbarik (TOHB) Pada Penyembuhan Ulkus Kaki DM Tipe 2 Berdasarkan Skor PEDISagus tinusNo ratings yet
- Facharbeit Laufen Von PhilipDocument2 pagesFacharbeit Laufen Von Philipphilipp.david079No ratings yet
- Activity 2 - US Measurements & Converting SystemsDocument3 pagesActivity 2 - US Measurements & Converting SystemsshayNo ratings yet
- Curvy Workout EbDocument2 pagesCurvy Workout Ebsuz8585No ratings yet
- 25 Best Exercises To Increase HeightDocument38 pages25 Best Exercises To Increase HeightPaden TranNo ratings yet
- Injury & Illness Prevention ProgramDocument2 pagesInjury & Illness Prevention ProgramsampathdtNo ratings yet
- Open Bed MakingDocument3 pagesOpen Bed MakingAparna HarshanNo ratings yet
- Ultimate BodyWeight Control, One Arm HandstandsDocument7 pagesUltimate BodyWeight Control, One Arm HandstandsVasyaNo ratings yet