
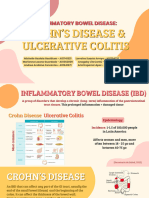
Inflammatory Bowl Disease
Inflammatory Bowl Disease
You might also like
- Essential Interviewing and Counseling Skills - An Integrated Approach To Practice (PDFDrive)Document439 pagesEssential Interviewing and Counseling Skills - An Integrated Approach To Practice (PDFDrive)Như Ngọc Nguyễn HoàngNo ratings yet
- Arnett-Facial Keys To Orthodontic Diagnosis IIDocument17 pagesArnett-Facial Keys To Orthodontic Diagnosis IIFiorella Loli Pinto100% (1)
- Medical Abbreviations: White Blood Cells: WBC 15. Bedrest: BR 6Document5 pagesMedical Abbreviations: White Blood Cells: WBC 15. Bedrest: BR 6Muhammad Farhan Rizqullah100% (1)
- Infidelity Treatment Patterns A Practice - Based Evidence Approach PDFDocument16 pagesInfidelity Treatment Patterns A Practice - Based Evidence Approach PDFJulián Alberto MatulevichNo ratings yet
- IBD Final11Document41 pagesIBD Final11abraham debebeNo ratings yet
- Inflammatory Bowel Disease: - DR - Parashuram Professor Department of Internal Medicine DR Bramch, BengaluruDocument39 pagesInflammatory Bowel Disease: - DR - Parashuram Professor Department of Internal Medicine DR Bramch, BengaluruNeelesh PatilNo ratings yet
- 28 - IbdDocument57 pages28 - IbdsitiNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel Diseasenathan asfahaNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- Ulcerative ColitisDocument21 pagesUlcerative Colitismel_chakNo ratings yet
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDocument18 pagesEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanNo ratings yet
- Inflammatory Bowel DiseaseDocument4 pagesInflammatory Bowel DiseaseJustisia PadmiyatiNo ratings yet
- Inflammatory Bowel DiseaseDocument66 pagesInflammatory Bowel Diseasestephanie gayetaNo ratings yet
- Inflammatory DisturbancesDocument63 pagesInflammatory DisturbancesWang Ming YaNo ratings yet
- Crohn'S Disease: Rahul R Menon I MSC MB & GeDocument25 pagesCrohn'S Disease: Rahul R Menon I MSC MB & GerahulbioNo ratings yet
- Crohn's DiseaseDocument8 pagesCrohn's DiseaseShannen Madrid Tindugan100% (1)
- Gastro NotesDocument18 pagesGastro NoteslukeNo ratings yet
- Ulcerative Colitis in ChildrenDocument5 pagesUlcerative Colitis in ChildrentheservantNo ratings yet
- Inflammatory Bowl Disease: RPH - Muhammad UsmanDocument19 pagesInflammatory Bowl Disease: RPH - Muhammad UsmanUsamaNo ratings yet
- Pharma 3Document38 pagesPharma 3starbadani38No ratings yet
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- Inflammatory Bowel Disease-1Document37 pagesInflammatory Bowel Disease-1SowndharyaNo ratings yet
- Swmana 4 Teórico Digestive DisordersDocument43 pagesSwmana 4 Teórico Digestive DisordersAna Paula Hernández CarballoNo ratings yet
- Msn-Small Bowel Disorder - SeminarDocument71 pagesMsn-Small Bowel Disorder - SeminarSarithaRajeshNo ratings yet
- Study Notes For Upper GI ProblemsDocument5 pagesStudy Notes For Upper GI ProblemsPrince K. Tailey100% (1)
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- Inflammatory Bowel Disease (IBD)Document41 pagesInflammatory Bowel Disease (IBD)ririNo ratings yet
- IBD - Shane Ryan ApperleyDocument63 pagesIBD - Shane Ryan Apperleyvivi avisaNo ratings yet
- Ulcerative ColitisDocument5 pagesUlcerative ColitisVenice Jame SanchezNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CK: GastroDocument32 pagesDr. Ali's Uworld Notes For Step 2 CK: GastrouyesNo ratings yet
- IBD Obat Ganguan Saluran CernaDocument13 pagesIBD Obat Ganguan Saluran CernaKhumairah mohtarNo ratings yet
- Praduman SirDocument38 pagesPraduman Sirguptaharshvardhan9565No ratings yet
- Inflammatory Bowel DiseaseDocument14 pagesInflammatory Bowel Diseasehazelel100% (1)
- Gastrointestinal Manifestations in Apeced Syndrome 2013Document9 pagesGastrointestinal Manifestations in Apeced Syndrome 2013jessicaNo ratings yet
- Inflammatory Bowel Disease: By: Yilak G. Augst 2015Document44 pagesInflammatory Bowel Disease: By: Yilak G. Augst 2015TESFAYE YIRSAWNo ratings yet
- Ulcerative Colitis: An Update: Authors: Jonathan P SegalDocument5 pagesUlcerative Colitis: An Update: Authors: Jonathan P SegalManoel Victor Moreira MachadoNo ratings yet
- Ulcerative Colitis and Crohns Disease AHN 1Document42 pagesUlcerative Colitis and Crohns Disease AHN 1Zille HummaNo ratings yet
- Ulcerative ColitisDocument17 pagesUlcerative ColitisCamille Joy Lucero Villegas100% (1)
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Ulcerative Colitis-Diagnostic and Therapeutic Algorithms: Continuing Medical EducationDocument14 pagesUlcerative Colitis-Diagnostic and Therapeutic Algorithms: Continuing Medical EducationManoel Victor Moreira MachadoNo ratings yet
- Ulcerativecolitis 170323180448 PDFDocument88 pagesUlcerativecolitis 170323180448 PDFBasudewo Agung100% (1)
- Inflammatory Bowel Disease (Ibd) : Dr. Fandy A. G. Gosal, MPPM, SP - Pd-KgehDocument15 pagesInflammatory Bowel Disease (Ibd) : Dr. Fandy A. G. Gosal, MPPM, SP - Pd-KgehvanessaNo ratings yet
- CholangitisDocument19 pagesCholangitisJohn mvulaNo ratings yet
- Gastritis: Ns. M. Ali Hamid, M. Kes., CWCCADocument86 pagesGastritis: Ns. M. Ali Hamid, M. Kes., CWCCAindri damayantiNo ratings yet
- Ulcerative Colitis: PseudopolypsDocument26 pagesUlcerative Colitis: PseudopolypsSocorro S. Gantalao-CorbedaNo ratings yet
- Ibd AnushaDocument32 pagesIbd AnushaRupesh R100% (1)
- Sem 1-Fitofarm - 2014Document24 pagesSem 1-Fitofarm - 2014Jessica Benavides BermudezNo ratings yet
- Peptic Ulcer Disease m1Document60 pagesPeptic Ulcer Disease m1frankozed1No ratings yet
- Involuntary Weight Loss (GSH)Document39 pagesInvoluntary Weight Loss (GSH)AchmadRizaNo ratings yet
- Infammatory Bowel Diseases: DR Yasser MahrousDocument32 pagesInfammatory Bowel Diseases: DR Yasser Mahrousmohamed hanyNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Coli TidesDocument11 pagesColi TidesAndrea Cayufilo CarmonaNo ratings yet
- Disorders of The Stomach and DuodenumDocument42 pagesDisorders of The Stomach and DuodenumMillicent KajaraNo ratings yet
- Pud 2Document5 pagesPud 2Jake MillerNo ratings yet
- Antibiotic-Associated Diarrhea andDocument41 pagesAntibiotic-Associated Diarrhea andSanjay ShresthaNo ratings yet
- Gastroenterology Conference 2019Document4 pagesGastroenterology Conference 2019Marie JosephNo ratings yet
- Khalil PathoDocument43 pagesKhalil PathoMohammad zreadNo ratings yet
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- 1 s2.0 S0022460X19305474 MainDocument11 pages1 s2.0 S0022460X19305474 MainKarin AdraiNo ratings yet
- Inexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationDocument8 pagesInexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationKarin AdraiNo ratings yet
- Transient Ischemic Attack: Tom Shefi NOV' 5, 2018Document54 pagesTransient Ischemic Attack: Tom Shefi NOV' 5, 2018Karin AdraiNo ratings yet
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- Summary of ECG AbnormalitiesDocument7 pagesSummary of ECG AbnormalitiesKarin AdraiNo ratings yet
- Lecture Notes First Semester Yr 2 BPham BMLS BDSDocument57 pagesLecture Notes First Semester Yr 2 BPham BMLS BDSKarin AdraiNo ratings yet
- Prescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionDocument20 pagesPrescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionSouthern California Public RadioNo ratings yet
- Liquid BiopsyDocument2 pagesLiquid BiopsySalman MajidNo ratings yet
- Nclex 3CDocument17 pagesNclex 3Cannisa mazda firdausNo ratings yet
- Data Sheet - HFO Heavy Fuel OilDocument9 pagesData Sheet - HFO Heavy Fuel OilPierluigiBusettoNo ratings yet
- Hist AntihisDocument20 pagesHist AntihisSusanti AsmiNo ratings yet
- Concept Map, Neil Floyd Ventura PDFDocument1 pageConcept Map, Neil Floyd Ventura PDFNeil Floyd VenturaNo ratings yet
- Zeolites Applications in Veterinary MedicineDocument17 pagesZeolites Applications in Veterinary MedicineCamelia TulcanNo ratings yet
- A Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerDocument6 pagesA Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerIOSRjournalNo ratings yet
- Summary X Ray MachineDocument3 pagesSummary X Ray MachineIndri SuciNo ratings yet
- FundamentalsDocument5 pagesFundamentalsWillieNo ratings yet
- Carum Carvi MonographDocument3 pagesCarum Carvi MonographOliver Rathbone100% (1)
- Allison Pinto TestimonyDocument4 pagesAllison Pinto TestimonyficanetworkNo ratings yet
- Neuro EquilibriumDocument6 pagesNeuro EquilibriumNeuro EquilibriumNo ratings yet
- How To Do Lymphatic Self-Massage On Your Face, Head and NeckDocument11 pagesHow To Do Lymphatic Self-Massage On Your Face, Head and NeckAkankshaNo ratings yet
- Croup Severity Score - UpToDateDocument3 pagesCroup Severity Score - UpToDateJosé Abraham Amaya DuarteNo ratings yet
- ACE Inhibitors Vs ARBsDocument4 pagesACE Inhibitors Vs ARBsRizqi Haqqum MNo ratings yet
- Beta Thalassemia: Thalassemia Minor or Thalassemia Trait - OnlyDocument7 pagesBeta Thalassemia: Thalassemia Minor or Thalassemia Trait - Onlydoc313No ratings yet
- Mental Illness BrochureDocument24 pagesMental Illness BrochureHadley AuliaNo ratings yet
- Primary SurveyDocument34 pagesPrimary SurveyTausif HaqueNo ratings yet
- BDocument18 pagesBBenjamin Tantiansu100% (1)
- Perioperative Nursing Reviewer Part 3Document13 pagesPerioperative Nursing Reviewer Part 3JUDE MARIANO JR. ALBANCES CARLOSNo ratings yet
- Ched-Prescribed Student Logbook On Patients Seen Department of Surgery-BghmcDocument2 pagesChed-Prescribed Student Logbook On Patients Seen Department of Surgery-BghmcMarieCrisNo ratings yet
- Which OCP Is Best Handout PDFDocument4 pagesWhich OCP Is Best Handout PDFMarianna LeeNo ratings yet
- Voucher TopamaxDocument2 pagesVoucher Topamaxapi-3738852100% (1)
- Zantac 150: (Ranitidine Hydrochloride) Tablets, USPDocument15 pagesZantac 150: (Ranitidine Hydrochloride) Tablets, USPbmartindoyle6396No ratings yet
- United States Court of Appeals: For The First CircuitDocument20 pagesUnited States Court of Appeals: For The First CircuitScribd Government DocsNo ratings yet































































































Download as pptx, pdf, or txt
You might also like
- Essential Interviewing and Counseling Skills - An Integrated Approach To Practice (PDFDrive)Document439 pagesEssential Interviewing and Counseling Skills - An Integrated Approach To Practice (PDFDrive)Như Ngọc Nguyễn HoàngNo ratings yet
- Arnett-Facial Keys To Orthodontic Diagnosis IIDocument17 pagesArnett-Facial Keys To Orthodontic Diagnosis IIFiorella Loli Pinto100% (1)
- Medical Abbreviations: White Blood Cells: WBC 15. Bedrest: BR 6Document5 pagesMedical Abbreviations: White Blood Cells: WBC 15. Bedrest: BR 6Muhammad Farhan Rizqullah100% (1)
- Infidelity Treatment Patterns A Practice - Based Evidence Approach PDFDocument16 pagesInfidelity Treatment Patterns A Practice - Based Evidence Approach PDFJulián Alberto MatulevichNo ratings yet
- IBD Final11Document41 pagesIBD Final11abraham debebeNo ratings yet
- Inflammatory Bowel Disease: - DR - Parashuram Professor Department of Internal Medicine DR Bramch, BengaluruDocument39 pagesInflammatory Bowel Disease: - DR - Parashuram Professor Department of Internal Medicine DR Bramch, BengaluruNeelesh PatilNo ratings yet
- 28 - IbdDocument57 pages28 - IbdsitiNo ratings yet
- Inflammatory Bowel DiseaseDocument19 pagesInflammatory Bowel Diseasenathan asfahaNo ratings yet
- Inflammatory Bowel Disease (Ibd)Document28 pagesInflammatory Bowel Disease (Ibd)suhaNo ratings yet
- Ulcerative ColitisDocument21 pagesUlcerative Colitismel_chakNo ratings yet
- 01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENDocument66 pages01 14 2021 GERD Inflammatory Bowel Disease Irritable Bowel Syndrome ALLENMikey ZhitnitskyNo ratings yet
- Inflammatoray Bowel DiseaseDocument14 pagesInflammatoray Bowel DiseaseSadr AkrmNo ratings yet
- Eric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafDocument18 pagesEric Ji-Yuan Mao, MD Samir A. Shah, MD, Facg, Fasge, AgafMuhammad GassanNo ratings yet
- Inflammatory Bowel DiseaseDocument4 pagesInflammatory Bowel DiseaseJustisia PadmiyatiNo ratings yet
- Inflammatory Bowel DiseaseDocument66 pagesInflammatory Bowel Diseasestephanie gayetaNo ratings yet
- Inflammatory DisturbancesDocument63 pagesInflammatory DisturbancesWang Ming YaNo ratings yet
- Crohn'S Disease: Rahul R Menon I MSC MB & GeDocument25 pagesCrohn'S Disease: Rahul R Menon I MSC MB & GerahulbioNo ratings yet
- Crohn's DiseaseDocument8 pagesCrohn's DiseaseShannen Madrid Tindugan100% (1)
- Gastro NotesDocument18 pagesGastro NoteslukeNo ratings yet
- Ulcerative Colitis in ChildrenDocument5 pagesUlcerative Colitis in ChildrentheservantNo ratings yet
- Inflammatory Bowl Disease: RPH - Muhammad UsmanDocument19 pagesInflammatory Bowl Disease: RPH - Muhammad UsmanUsamaNo ratings yet
- Pharma 3Document38 pagesPharma 3starbadani38No ratings yet
- Inflammatory Bowel DiseaseDocument15 pagesInflammatory Bowel DiseaseYanushka Bruce HerathNo ratings yet
- Inflammatory Bowel Disease-1Document37 pagesInflammatory Bowel Disease-1SowndharyaNo ratings yet
- Swmana 4 Teórico Digestive DisordersDocument43 pagesSwmana 4 Teórico Digestive DisordersAna Paula Hernández CarballoNo ratings yet
- Msn-Small Bowel Disorder - SeminarDocument71 pagesMsn-Small Bowel Disorder - SeminarSarithaRajeshNo ratings yet
- Study Notes For Upper GI ProblemsDocument5 pagesStudy Notes For Upper GI ProblemsPrince K. Tailey100% (1)
- Inflammatory Bowel Disease .. Last EditDocument22 pagesInflammatory Bowel Disease .. Last EditRashed ShatnawiNo ratings yet
- Inflammatory Bowel Disease (IBD)Document41 pagesInflammatory Bowel Disease (IBD)ririNo ratings yet
- IBD - Shane Ryan ApperleyDocument63 pagesIBD - Shane Ryan Apperleyvivi avisaNo ratings yet
- Ulcerative ColitisDocument5 pagesUlcerative ColitisVenice Jame SanchezNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CK: GastroDocument32 pagesDr. Ali's Uworld Notes For Step 2 CK: GastrouyesNo ratings yet
- IBD Obat Ganguan Saluran CernaDocument13 pagesIBD Obat Ganguan Saluran CernaKhumairah mohtarNo ratings yet
- Praduman SirDocument38 pagesPraduman Sirguptaharshvardhan9565No ratings yet
- Inflammatory Bowel DiseaseDocument14 pagesInflammatory Bowel Diseasehazelel100% (1)
- Gastrointestinal Manifestations in Apeced Syndrome 2013Document9 pagesGastrointestinal Manifestations in Apeced Syndrome 2013jessicaNo ratings yet
- Inflammatory Bowel Disease: By: Yilak G. Augst 2015Document44 pagesInflammatory Bowel Disease: By: Yilak G. Augst 2015TESFAYE YIRSAWNo ratings yet
- Ulcerative Colitis: An Update: Authors: Jonathan P SegalDocument5 pagesUlcerative Colitis: An Update: Authors: Jonathan P SegalManoel Victor Moreira MachadoNo ratings yet
- Ulcerative Colitis and Crohns Disease AHN 1Document42 pagesUlcerative Colitis and Crohns Disease AHN 1Zille HummaNo ratings yet
- Ulcerative ColitisDocument17 pagesUlcerative ColitisCamille Joy Lucero Villegas100% (1)
- UlcerativecolitisDocument27 pagesUlcerativecolitisMohamed Abdulrazaq100% (1)
- Ulcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryDocument71 pagesUlcerative Colitis: DR Syed Ubaid Associate Professor of SurgeryFachry Al RafiqiNo ratings yet
- Crohns DiseaseDocument32 pagesCrohns DiseaseMin Chi PakNo ratings yet
- Inflammatory Bowel DiseaseDocument59 pagesInflammatory Bowel DiseaseLala Rahma Qodriyan SofiakmiNo ratings yet
- Ulcerative Colitis-Diagnostic and Therapeutic Algorithms: Continuing Medical EducationDocument14 pagesUlcerative Colitis-Diagnostic and Therapeutic Algorithms: Continuing Medical EducationManoel Victor Moreira MachadoNo ratings yet
- Ulcerativecolitis 170323180448 PDFDocument88 pagesUlcerativecolitis 170323180448 PDFBasudewo Agung100% (1)
- Inflammatory Bowel Disease (Ibd) : Dr. Fandy A. G. Gosal, MPPM, SP - Pd-KgehDocument15 pagesInflammatory Bowel Disease (Ibd) : Dr. Fandy A. G. Gosal, MPPM, SP - Pd-KgehvanessaNo ratings yet
- CholangitisDocument19 pagesCholangitisJohn mvulaNo ratings yet
- Gastritis: Ns. M. Ali Hamid, M. Kes., CWCCADocument86 pagesGastritis: Ns. M. Ali Hamid, M. Kes., CWCCAindri damayantiNo ratings yet
- Ulcerative Colitis: PseudopolypsDocument26 pagesUlcerative Colitis: PseudopolypsSocorro S. Gantalao-CorbedaNo ratings yet
- Ibd AnushaDocument32 pagesIbd AnushaRupesh R100% (1)
- Sem 1-Fitofarm - 2014Document24 pagesSem 1-Fitofarm - 2014Jessica Benavides BermudezNo ratings yet
- Peptic Ulcer Disease m1Document60 pagesPeptic Ulcer Disease m1frankozed1No ratings yet
- Involuntary Weight Loss (GSH)Document39 pagesInvoluntary Weight Loss (GSH)AchmadRizaNo ratings yet
- Infammatory Bowel Diseases: DR Yasser MahrousDocument32 pagesInfammatory Bowel Diseases: DR Yasser Mahrousmohamed hanyNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Coli TidesDocument11 pagesColi TidesAndrea Cayufilo CarmonaNo ratings yet
- Disorders of The Stomach and DuodenumDocument42 pagesDisorders of The Stomach and DuodenumMillicent KajaraNo ratings yet
- Pud 2Document5 pagesPud 2Jake MillerNo ratings yet
- Antibiotic-Associated Diarrhea andDocument41 pagesAntibiotic-Associated Diarrhea andSanjay ShresthaNo ratings yet
- Gastroenterology Conference 2019Document4 pagesGastroenterology Conference 2019Marie JosephNo ratings yet
- Khalil PathoDocument43 pagesKhalil PathoMohammad zreadNo ratings yet
- Fast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careFrom EverandFast Facts: Inflammatory Bowel Disease: Translating the science into compassionate IBD careNo ratings yet
- 1 s2.0 S0022460X19305474 MainDocument11 pages1 s2.0 S0022460X19305474 MainKarin AdraiNo ratings yet
- Inexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationDocument8 pagesInexpensive FIA Method To Determine Trace Levels of Imazapyr by UV-detection Enhanced With Electrochemical PolarizationKarin AdraiNo ratings yet
- Transient Ischemic Attack: Tom Shefi NOV' 5, 2018Document54 pagesTransient Ischemic Attack: Tom Shefi NOV' 5, 2018Karin AdraiNo ratings yet
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- Create A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouDocument6 pagesCreate A PDF File: Exercise 1 and Exercise 2 Produce The Same Result. Choose The One That Works Best For YouKarin AdraiNo ratings yet
- Summary of ECG AbnormalitiesDocument7 pagesSummary of ECG AbnormalitiesKarin AdraiNo ratings yet
- Lecture Notes First Semester Yr 2 BPham BMLS BDSDocument57 pagesLecture Notes First Semester Yr 2 BPham BMLS BDSKarin AdraiNo ratings yet
- Prescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionDocument20 pagesPrescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionSouthern California Public RadioNo ratings yet
- Liquid BiopsyDocument2 pagesLiquid BiopsySalman MajidNo ratings yet
- Nclex 3CDocument17 pagesNclex 3Cannisa mazda firdausNo ratings yet
- Data Sheet - HFO Heavy Fuel OilDocument9 pagesData Sheet - HFO Heavy Fuel OilPierluigiBusettoNo ratings yet
- Hist AntihisDocument20 pagesHist AntihisSusanti AsmiNo ratings yet
- Concept Map, Neil Floyd Ventura PDFDocument1 pageConcept Map, Neil Floyd Ventura PDFNeil Floyd VenturaNo ratings yet
- Zeolites Applications in Veterinary MedicineDocument17 pagesZeolites Applications in Veterinary MedicineCamelia TulcanNo ratings yet
- A Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerDocument6 pagesA Comparative Study of Topical Phenytoin Vs Conventional Wound Care in Diabetic UlcerIOSRjournalNo ratings yet
- Summary X Ray MachineDocument3 pagesSummary X Ray MachineIndri SuciNo ratings yet
- FundamentalsDocument5 pagesFundamentalsWillieNo ratings yet
- Carum Carvi MonographDocument3 pagesCarum Carvi MonographOliver Rathbone100% (1)
- Allison Pinto TestimonyDocument4 pagesAllison Pinto TestimonyficanetworkNo ratings yet
- Neuro EquilibriumDocument6 pagesNeuro EquilibriumNeuro EquilibriumNo ratings yet
- How To Do Lymphatic Self-Massage On Your Face, Head and NeckDocument11 pagesHow To Do Lymphatic Self-Massage On Your Face, Head and NeckAkankshaNo ratings yet
- Croup Severity Score - UpToDateDocument3 pagesCroup Severity Score - UpToDateJosé Abraham Amaya DuarteNo ratings yet
- ACE Inhibitors Vs ARBsDocument4 pagesACE Inhibitors Vs ARBsRizqi Haqqum MNo ratings yet
- Beta Thalassemia: Thalassemia Minor or Thalassemia Trait - OnlyDocument7 pagesBeta Thalassemia: Thalassemia Minor or Thalassemia Trait - Onlydoc313No ratings yet
- Mental Illness BrochureDocument24 pagesMental Illness BrochureHadley AuliaNo ratings yet
- Primary SurveyDocument34 pagesPrimary SurveyTausif HaqueNo ratings yet
- BDocument18 pagesBBenjamin Tantiansu100% (1)
- Perioperative Nursing Reviewer Part 3Document13 pagesPerioperative Nursing Reviewer Part 3JUDE MARIANO JR. ALBANCES CARLOSNo ratings yet
- Ched-Prescribed Student Logbook On Patients Seen Department of Surgery-BghmcDocument2 pagesChed-Prescribed Student Logbook On Patients Seen Department of Surgery-BghmcMarieCrisNo ratings yet
- Which OCP Is Best Handout PDFDocument4 pagesWhich OCP Is Best Handout PDFMarianna LeeNo ratings yet
- Voucher TopamaxDocument2 pagesVoucher Topamaxapi-3738852100% (1)
- Zantac 150: (Ranitidine Hydrochloride) Tablets, USPDocument15 pagesZantac 150: (Ranitidine Hydrochloride) Tablets, USPbmartindoyle6396No ratings yet
- United States Court of Appeals: For The First CircuitDocument20 pagesUnited States Court of Appeals: For The First CircuitScribd Government DocsNo ratings yet