Download as ppt, pdf, or txt
You might also like
- Miscarriage & Early Pregnancy LossDocument38 pagesMiscarriage & Early Pregnancy LossLuqman OsmanNo ratings yet
- High Risk PregnancyDocument10 pagesHigh Risk PregnancyRoy Mujeres CabueñasNo ratings yet
- Druthers March 2021Document12 pagesDruthers March 2021ThomasZiehmer100% (1)
- Abortion KuliahDocument38 pagesAbortion KuliahElsa Hasibuan100% (1)
- 1 - Bleeding in Early PregnancyDocument14 pages1 - Bleeding in Early PregnancyAMEER ALSAABRAWINo ratings yet
- Early Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahDocument33 pagesEarly Pregnancy Complications: by Harvir Singh Supervised by DR Ranjit and DR SyafiqahShre RanjithamNo ratings yet
- 。14.1 Abortion, Miscarriage, TOP 2Document57 pages。14.1 Abortion, Miscarriage, TOP 2genaong2003No ratings yet
- Those Related To The Pregnant State: AbortionDocument43 pagesThose Related To The Pregnant State: AbortionJohannah DaroNo ratings yet
- Miscarriage Early Pregnancy LossDocument10 pagesMiscarriage Early Pregnancy LossiwennieNo ratings yet
- AbortionDocument38 pagesAbortionMd AamirNo ratings yet
- Abortion, Ectopic PregnancyDocument139 pagesAbortion, Ectopic PregnancyINFORMASI MENARIKNo ratings yet
- 2-Complications of Pregnancy Pt1Document37 pages2-Complications of Pregnancy Pt1pavi7muruganathanNo ratings yet
- Bleeding in Early PregnancyDocument28 pagesBleeding in Early Pregnancyinciy093No ratings yet
- Ectopic PregnancyDocument3 pagesEctopic PregnancyMary Anne Yap100% (1)
- Abortion SolenyDocument123 pagesAbortion SolenyAyalewNo ratings yet
- CME Miscarriages Combined 1Document76 pagesCME Miscarriages Combined 1syawal zulfitriNo ratings yet
- D. High Risk PregnanciesDocument78 pagesD. High Risk PregnanciesKeziah TampusNo ratings yet
- Bleeding in Early PregnancyDocument33 pagesBleeding in Early PregnancyFirdaus ShaharNo ratings yet
- Bleeding in Early PregnancyDocument40 pagesBleeding in Early PregnancyOmar mohamedNo ratings yet
- Ectopic PregnancyDocument61 pagesEctopic PregnancySuchie ILyasNo ratings yet
- Obg AbortionDocument62 pagesObg Abortionkashyap priyankaNo ratings yet
- Gestational ConditionsDocument148 pagesGestational ConditionsEsvinch EsvinchNo ratings yet
- Chapter 21Document69 pagesChapter 212082194No ratings yet
- Bleeding in Early PregnancyDocument32 pagesBleeding in Early PregnancyPhuntsho OngmoNo ratings yet
- Bleeding During PregnancyDocument69 pagesBleeding During PregnancyMohnnad Hmood AlgaraybhNo ratings yet
- HemorrhagesDocument3 pagesHemorrhagesARAugustoNo ratings yet
- Abortus: Levina Felicia Supervisor:Dr. Mulyanusa A. Ritonga, Spog (K) ., M.KesDocument27 pagesAbortus: Levina Felicia Supervisor:Dr. Mulyanusa A. Ritonga, Spog (K) ., M.KesIMO UNPADNo ratings yet
- AbortionDocument39 pagesAbortionmedico100% (1)
- AbortionsDocument25 pagesAbortionsaravindNo ratings yet
- Abortion: Renhe Hospital Wang JunjieDocument51 pagesAbortion: Renhe Hospital Wang JunjieMadhu Sudhan PandeyaNo ratings yet
- Individual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerDocument11 pagesIndividual Activity #3: CHAPTER STUDY QUESTIONS: Rubric For Short AnswerSatanichia McDowell KurumizawaNo ratings yet
- Obsandgyne Tables 200pagesDocument221 pagesObsandgyne Tables 200pagesRashed ShatnawiNo ratings yet
- Abortion (BEST)Document40 pagesAbortion (BEST)lemesamamo2023No ratings yet
- Abruptio Placenta and AbortionDocument10 pagesAbruptio Placenta and Abortiondanica grace gubaNo ratings yet
- 2 Nursing Care of The Pregnant Client Gestational ConditionDocument120 pages2 Nursing Care of The Pregnant Client Gestational ConditionjustinjareddNo ratings yet
- 2 Abortion& Ectopic PXDocument33 pages2 Abortion& Ectopic PXabrhamNo ratings yet
- AbortionDocument19 pagesAbortionhodoa437No ratings yet
- Pregnancy Complication: Department of Gynaecology and ObstetricsDocument59 pagesPregnancy Complication: Department of Gynaecology and ObstetricssanjivdasNo ratings yet
- Obs-Gynae CP Final (2nd Batch)Document89 pagesObs-Gynae CP Final (2nd Batch)Dipesh ShresthaNo ratings yet
- AbortionDocument67 pagesAbortionaneley cherinetNo ratings yet
- First Trimester BleedingDocument48 pagesFirst Trimester BleedingEliana ArshidNo ratings yet
- MiscarriageDocument38 pagesMiscarriagezianab aliNo ratings yet
- Module For Abnormal OB 1 - 120227Document129 pagesModule For Abnormal OB 1 - 120227Elizabeth MadejaNo ratings yet
- Vaginal Bleeding in Early PregnancyDocument25 pagesVaginal Bleeding in Early PregnancyPshtiwan MahmoodNo ratings yet
- Completed ABORTION SEMINARDocument31 pagesCompleted ABORTION SEMINARkalla sharon100% (1)
- Obstetric Highlights Elmar P. Sakala PDFDocument47 pagesObstetric Highlights Elmar P. Sakala PDFwalt65No ratings yet
- Vaginal Bleeding in Early PregnancyDocument8 pagesVaginal Bleeding in Early PregnancyBal Ri Mekoleu100% (1)
- Abortion - Del RosarioDocument29 pagesAbortion - Del RosarioLouise Del RosarioNo ratings yet
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- Bleeding in Early Pregnancy Slide WorldDocument57 pagesBleeding in Early Pregnancy Slide Worlddashing_ritamNo ratings yet
- Complications During Pregnancy - Chapt 5 - 1Document40 pagesComplications During Pregnancy - Chapt 5 - 1Bob IrsanNo ratings yet
- Abortion 1Document46 pagesAbortion 1Nikhil TyagiNo ratings yet
- Abortion 4Document45 pagesAbortion 4blatchujosephNo ratings yet
- 5 - Abortion or MiscarriageDocument43 pages5 - Abortion or Miscarriageasifdawar2011No ratings yet
- Bleeding in Early Late PregnancyDocument46 pagesBleeding in Early Late PregnancyAndrada Catrinoiu100% (2)
- Case Study #1: AbortionDocument42 pagesCase Study #1: AbortionJhoanne DelloroNo ratings yet
- Ectopic Pregnancy RevisedDocument44 pagesEctopic Pregnancy RevisedDegefaw BikoyNo ratings yet
- Book Picture Patient PictureDocument22 pagesBook Picture Patient PictureAnsiya K ANo ratings yet
- AbortionDocument33 pagesAbortionAbdi Ñãśìr Møhàmèď ŚàĺàhNo ratings yet
- Spontaneous Abortion PPDocument47 pagesSpontaneous Abortion PPSurgeon Raza Hamid100% (1)
- It's Not Just a Heavy Period; The Miscarriage HandbookFrom EverandIt's Not Just a Heavy Period; The Miscarriage HandbookRating: 2 out of 5 stars2/5 (1)
- Material Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseDocument14 pagesMaterial Safety Data Sheet Belzona® 1311 (Ceramic R-Metal) BaseAri BinukoNo ratings yet
- Assessment of Patients in Emergency DepartmentDocument22 pagesAssessment of Patients in Emergency DepartmentClaudine PadillonNo ratings yet
- The Healing BreathDocument48 pagesThe Healing BreathEugenia Saparipa100% (3)
- Event Investigation: William L. (Bill) Rankin, Ph.D. Boeing Technical FellowDocument18 pagesEvent Investigation: William L. (Bill) Rankin, Ph.D. Boeing Technical FellowLemuel PetronioNo ratings yet
- Mental Health Nursing.: Lesson 1Document177 pagesMental Health Nursing.: Lesson 1Eng Steve WairuaNo ratings yet
- Mother and Child Tracking System-ANAND MLHPDocument42 pagesMother and Child Tracking System-ANAND MLHPAnand gowdaNo ratings yet
- DLL Mapeh Q 3 WK2 Health StraightDocument6 pagesDLL Mapeh Q 3 WK2 Health StraightEdelyn UnayNo ratings yet
- For 'Best Practices in O&M Safety' PDFDocument153 pagesFor 'Best Practices in O&M Safety' PDFSachinGoyalNo ratings yet
- Fair Recruitment & Selection HandbookDocument22 pagesFair Recruitment & Selection HandbookKavithri ponnappaNo ratings yet
- Admin Law Sample Paper 1Document10 pagesAdmin Law Sample Paper 1Jaskaran Singh BediNo ratings yet
- 06SMARTeZ Drug Stability Table Non USDocument2 pages06SMARTeZ Drug Stability Table Non USJessica Blaine BrumfieldNo ratings yet
- Proctology CatalogDocument6 pagesProctology CatalogArber LicajNo ratings yet
- Mapeh 10Document5 pagesMapeh 10laczalj423No ratings yet
- Time Me, Gentlemen! The Bravado and Bravery of Robert ListonDocument5 pagesTime Me, Gentlemen! The Bravado and Bravery of Robert ListonJonathan IsleyNo ratings yet
- 12th 3Document35 pages12th 3sandeepNo ratings yet
- Behavior Intervention and Support Plan (BISP)Document5 pagesBehavior Intervention and Support Plan (BISP)api-379946201No ratings yet
- Journal of The World Federation of OrthodontistsDocument6 pagesJournal of The World Federation of OrthodontistsJuan Carlos MeloNo ratings yet
- Practitioner Guide Georgia English 20130516Document310 pagesPractitioner Guide Georgia English 20130516OSGFNo ratings yet
- Medical College List GujaratDocument1 pageMedical College List GujaratAjay Pal SinghNo ratings yet
- Shimul Tula Medicinal Qualities PaperDocument8 pagesShimul Tula Medicinal Qualities PapertojinboNo ratings yet
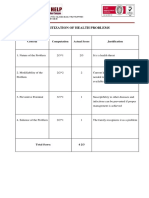
- Prioritization of Health Problems: ParenthoodDocument3 pagesPrioritization of Health Problems: ParenthoodMariana Mikaela AlagarNo ratings yet
- October 25, 2013 Strathmore Times PDFDocument31 pagesOctober 25, 2013 Strathmore Times PDFStrathmore TimesNo ratings yet
- Gilroy Dispatch, February 15, 2019Document40 pagesGilroy Dispatch, February 15, 2019SimonNo ratings yet
- Pattys Generic Letter of RecommendationDocument1 pagePattys Generic Letter of Recommendationapi-355484042No ratings yet
- SN MCQ Block IDocument12 pagesSN MCQ Block Iطال الإنتظارNo ratings yet
- Group 10: 1. Describe The Journey of Shahnaz HussainDocument3 pagesGroup 10: 1. Describe The Journey of Shahnaz HussainShyamsunder SharmaNo ratings yet
- Full Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All ChapterDocument69 pagesFull Ebook of Cardiopulmonary Bypass 3Rd Edition Florian Falter Online PDF All Chapterjustinesmedt868100% (5)
- Daftar PustakaDocument2 pagesDaftar PustakaSyaifulBahriNo ratings yet
- CONSOL Form Oil WBDocument3 pagesCONSOL Form Oil WBimmanuel lumbantobingNo ratings yet