Download as ppt, pdf, or txt
You might also like
- Sample Review Questions MTLE 2019Document73 pagesSample Review Questions MTLE 2019Kervy Jay AgraviadorNo ratings yet
- Anatomy and Physiology of EarDocument33 pagesAnatomy and Physiology of EarNidya PutriNo ratings yet
- Hem Lab Manual Diff F16Document10 pagesHem Lab Manual Diff F16LAB.RSWB0% (1)
- Basic Examination of BloodDocument48 pagesBasic Examination of Bloodmedino100% (1)
- PT Wakode - Clinical Methods in ENT PDFDocument171 pagesPT Wakode - Clinical Methods in ENT PDFRisya Nur Fadillah Sapitri100% (3)
- BT - EfaDocument94 pagesBT - EfaCharles NepomucenoNo ratings yet
- 1.BC 5800 PrincipleDocument37 pages1.BC 5800 PrinciplekiryNo ratings yet
- CSF PDFDocument58 pagesCSF PDFVas KannanNo ratings yet
- CSF LectureDocument58 pagesCSF Lectureshweta yadavNo ratings yet
- Anurbf 132 135Document4 pagesAnurbf 132 135Victor GonzalesNo ratings yet
- Cerebrospinal Fluid: Practice Test SheetDocument7 pagesCerebrospinal Fluid: Practice Test SheetJoey MagnoNo ratings yet
- Cerebrospinal Fluid: Prepared By: Muath M. Abu-Samreh Supervisor: Dr. Samir KhalilDocument12 pagesCerebrospinal Fluid: Prepared By: Muath M. Abu-Samreh Supervisor: Dr. Samir KhalilMohammad Abu-SamrehNo ratings yet
- Hema I Chapter 14 - CSFDocument28 pagesHema I Chapter 14 - CSFTesfaNo ratings yet
- Presentation On Full Blood Count by Group EightDocument15 pagesPresentation On Full Blood Count by Group Eightmaxwell amponsahNo ratings yet
- Cerebrospinal FluidDocument12 pagesCerebrospinal FluidMuath M. AbusamrehNo ratings yet
- Hema I Chapter 14_CSFDocument40 pagesHema I Chapter 14_CSFtsegeye aregawiNo ratings yet
- Presentation On Full Blood Count by Group EightDocument15 pagesPresentation On Full Blood Count by Group Eightmaxwell amponsahNo ratings yet
- Basics in Haematology Nihon KohdenDocument63 pagesBasics in Haematology Nihon Kohdengkp97899No ratings yet
- CSF, UF 1000i, 2015Document11 pagesCSF, UF 1000i, 2015balkisNo ratings yet
- Cerebrospinal Fluid CSFDocument60 pagesCerebrospinal Fluid CSFpikachuNo ratings yet
- Cerebrospinal FluidDocument43 pagesCerebrospinal FluidBrylle UgayNo ratings yet
- Meningitis MicrobiologyDocument74 pagesMeningitis MicrobiologyJyoti YadavNo ratings yet
- Blood Sample Preparation Techniques and ProtocolsDocument34 pagesBlood Sample Preparation Techniques and ProtocolsnadiaghiamorNo ratings yet
- The Peripheral Blood FilmDocument5 pagesThe Peripheral Blood FilmanggaririnNo ratings yet
- Hema I Chapter 8 - DiffDocument67 pagesHema I Chapter 8 - DiffderibewNo ratings yet
- 1 Hematology TestDocument48 pages1 Hematology TestAhmed YassinNo ratings yet
- hema 8Document73 pageshema 8tsegeye aregawiNo ratings yet
- Basic HematologyDocument89 pagesBasic Hematologydrafq2000No ratings yet
- Como Interpreto Un Hemograma en Adulto-Mayo-2005Document14 pagesComo Interpreto Un Hemograma en Adulto-Mayo-2005Gustavo VasquezNo ratings yet
- Handout Basic HematologyDocument188 pagesHandout Basic HematologymaikkadoriaNo ratings yet
- Body Fluid Chapter 1Document76 pagesBody Fluid Chapter 1kanakalakshmimbsfNo ratings yet
- 4 CSF Examination-1Document35 pages4 CSF Examination-1Bilal LatifNo ratings yet
- Reticulocyte Count: Name: - SGD GRP: - Tests On Blood Cell DisordersDocument6 pagesReticulocyte Count: Name: - SGD GRP: - Tests On Blood Cell DisordersChristyl JoNo ratings yet
- Lab4: Cerebral Spinal Fluid (CSF) : Faisal Klufah M.S.H.S, MLS (ASCP)Document30 pagesLab4: Cerebral Spinal Fluid (CSF) : Faisal Klufah M.S.H.S, MLS (ASCP)wfNo ratings yet
- Hematology Romania-1Document88 pagesHematology Romania-1Ştefania MafteiNo ratings yet
- Blood and He Ma To PoiesisDocument19 pagesBlood and He Ma To PoiesisDrishtantRaghavNo ratings yet
- CBCDocument15 pagesCBCUlicer CruzNo ratings yet
- Hematology 1 (Laboratory) - Week 10-11 ModuleDocument8 pagesHematology 1 (Laboratory) - Week 10-11 ModuleJam RamosNo ratings yet
- 4 - Hematology UnitDocument16 pages4 - Hematology UnitMary Cabalce100% (1)
- SEED Haematology: Sysmex Educational Enhancement and Development March 2012Document4 pagesSEED Haematology: Sysmex Educational Enhancement and Development March 2012ujjawal_46No ratings yet
- Automated Counters3Document14 pagesAutomated Counters3Jacky SharmaNo ratings yet
- Test Bank for Rodaks Hematology 5th Edition by Keohane download pdf full chapterDocument26 pagesTest Bank for Rodaks Hematology 5th Edition by Keohane download pdf full chapterpozzhuadji100% (8)
- NRBCDocument5 pagesNRBCGaurav AggarwalNo ratings yet
- 2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyDocument3 pages2nd Sem - Hema1 - An Overview of Clinical Laboratory HematologyAisle Malibiran PalerNo ratings yet
- Lab Activity No. 8 - Slide PresentationDocument20 pagesLab Activity No. 8 - Slide PresentationChelsea Padilla Delos ReyesNo ratings yet
- DR Preeti Mansukhani - CBC 5 Parts - 2017Document56 pagesDR Preeti Mansukhani - CBC 5 Parts - 2017Silence T-jmNo ratings yet
- CSFDocument37 pagesCSFMujtaba IbrahimNo ratings yet
- Other Body Fluid Cerebrospinal FluidDocument16 pagesOther Body Fluid Cerebrospinal Fluidrona hilarioNo ratings yet
- Novel Automated Hematology Parameters in Clinical Pediatric PracticeDocument9 pagesNovel Automated Hematology Parameters in Clinical Pediatric PracticerahulNo ratings yet
- Haematology 2 ManualDocument26 pagesHaematology 2 Manualhayamitib11No ratings yet
- 10 1111@ijlh 12760Document6 pages10 1111@ijlh 12760Hedo HidayatNo ratings yet
- Letter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologyDocument3 pagesLetter To The Editor: Comparison Between Automated and Microscopic Analysis in Body Fluids CytologybalkisNo ratings yet
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- Classification_of_Blood_Cells_Using_Deep_Learning_Document19 pagesClassification_of_Blood_Cells_Using_Deep_Learning_Sandhyashree UNo ratings yet
- Accurasi Perhitungan PlateletDocument68 pagesAccurasi Perhitungan PlateletMaria Yosefina HeraNo ratings yet
- WBC Count, CSF, XN 5000, 2014Document8 pagesWBC Count, CSF, XN 5000, 2014balkisNo ratings yet
- Hematology Must Knows-Converted-1 PDFDocument13 pagesHematology Must Knows-Converted-1 PDFJeffrey LimNo ratings yet
- Hematology Must Knows PDFDocument34 pagesHematology Must Knows PDFJeffrey LimNo ratings yet
- Chapter SixDocument182 pagesChapter Sixtadele10No ratings yet
- 3 PracticalDocument47 pages3 PracticalT NNo ratings yet
- Piis0025619611615681 PDFDocument14 pagesPiis0025619611615681 PDFMaryJoy Dela CruzNo ratings yet
- Red CellDocument4 pagesRed CellUmer naeemNo ratings yet
- Topic 2Document21 pagesTopic 2Jacqueline Tungcul DonatoNo ratings yet
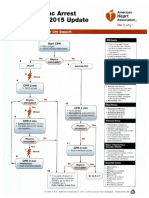
- ACLS 2015 Algorithm PDFDocument8 pagesACLS 2015 Algorithm PDFRisya Nur Fadillah SapitriNo ratings yet
- Case Report LBPDocument34 pagesCase Report LBPRisya Nur Fadillah SapitriNo ratings yet
- Bimbingan Ko-AsDocument14 pagesBimbingan Ko-AsRisya Nur Fadillah SapitriNo ratings yet
- Contoh Case ReportDocument4 pagesContoh Case ReportLyvia ChristieNo ratings yet
- Rulerships and Qualities Anatomy and Physiology Correlated To The ZodiacDocument4 pagesRulerships and Qualities Anatomy and Physiology Correlated To The Zodiactushar100% (1)
- TECH 614 Full Spine I (Castellucci)Document10 pagesTECH 614 Full Spine I (Castellucci)Robert StraubNo ratings yet
- Animalia ChartDocument8 pagesAnimalia CharthkNo ratings yet
- BoneDocument47 pagesBoned2krgn6hbmNo ratings yet
- Fertilization Fetal DevelopmentDocument97 pagesFertilization Fetal DevelopmentXo Yem100% (1)
- Kelainan Morf EritrositDocument12 pagesKelainan Morf EritrositTrio Singgih SaputroNo ratings yet
- Párpado Duane'sDocument34 pagesPárpado Duane'sLuis Miguel Salazar AmatureNo ratings yet
- Kuliah 3 - Fisiologi Sistem Muskuloskeletal (Dr. Adelia Handoko)Document36 pagesKuliah 3 - Fisiologi Sistem Muskuloskeletal (Dr. Adelia Handoko)Linda ayuNo ratings yet
- Leukemia: What You Need To Know AboutDocument36 pagesLeukemia: What You Need To Know AboutOsama AlrawabNo ratings yet
- Chorionic Villus Sampling: Ashique Palliyal 09M2385Document15 pagesChorionic Villus Sampling: Ashique Palliyal 09M2385Sanjay Kumar SanjuNo ratings yet
- Respiration in Organisms: A. Short Answers QuestionsDocument5 pagesRespiration in Organisms: A. Short Answers QuestionsnarayanaNo ratings yet
- ABSTRAK-Izzatul AzmiDocument3 pagesABSTRAK-Izzatul AzmiMuhammad DzulfachriNo ratings yet
- Patología Bucal - Bruch (Ingles)Document176 pagesPatología Bucal - Bruch (Ingles)MarielEsmeraldaNo ratings yet
- 3-Major Veins of The BodyDocument26 pages3-Major Veins of The BodyTJPlayz100% (1)
- Rodent OncologyDocument24 pagesRodent Oncology黃皓No ratings yet
- Bronchial Asthma Power PointDocument44 pagesBronchial Asthma Power Pointjohnbech07No ratings yet
- 1GS Cell PPT 2018Document73 pages1GS Cell PPT 2018pixiedustNo ratings yet
- Cloning 1 QPDocument11 pagesCloning 1 QPWayne Mc DonaghNo ratings yet
- Lecture 1 Respiratory SystemDocument2 pagesLecture 1 Respiratory SystemArnelNo ratings yet
- 12-New Physiology of The EyeDocument53 pages12-New Physiology of The EyeFaris Azhar100% (1)
- Hematology Reference RangeDocument1 pageHematology Reference RangeNheeya WarzNo ratings yet
- Massive Haemorrhage: P Donnelly B FergusonDocument18 pagesMassive Haemorrhage: P Donnelly B FergusonRizqiNo ratings yet
- EndocrineDocument94 pagesEndocrineSuzana VoiculescuNo ratings yet
- Blood Supply To The GitDocument15 pagesBlood Supply To The GitEniola abdullahi AduagbaNo ratings yet
- Lipoma & Kista AtheromaDocument24 pagesLipoma & Kista AtheromaAgnes NiyNo ratings yet
- Brain-Aging-By Ray PeatDocument2 pagesBrain-Aging-By Ray PeatIURY GABRIEL DUARTE SANTOSNo ratings yet