
Liver Cirrhosis: USMF "Nicolae Testemiţanu"
Liver Cirrhosis: USMF "Nicolae Testemiţanu"
You might also like
- Project-Charter (Mohammad Adnan)Document4 pagesProject-Charter (Mohammad Adnan)Mohammad Adnan80% (5)
- A Complete Neurological Nursing Assessment GuideDocument57 pagesA Complete Neurological Nursing Assessment GuideSarithaRajeshNo ratings yet
- List of Government WebsitesDocument1 pageList of Government Websitessumit-7No ratings yet
- Hydrolysis of Nucleic AcidsDocument7 pagesHydrolysis of Nucleic Acidskeepersake81% (16)
- Cirrhosis - Hepatic and Biliary Disorders - MSD Manual Professional EditionDocument9 pagesCirrhosis - Hepatic and Biliary Disorders - MSD Manual Professional EditionSky ShieldNo ratings yet
- L10 - Liver CirrhosisDocument10 pagesL10 - Liver CirrhosisMerehan El RoosNo ratings yet
- Cirrhosis: DR AkhondeiDocument111 pagesCirrhosis: DR AkhondeiMuvenn KannanNo ratings yet
- The Pathogenesis of Liver Cirrhosis / Fibrosis: Dr. Indranil BhattacharyaDocument46 pagesThe Pathogenesis of Liver Cirrhosis / Fibrosis: Dr. Indranil BhattacharyaDr. Indranil BhattacharayaNo ratings yet
- Cirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverDocument29 pagesCirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverdahsyatnyaNo ratings yet
- 3rd Stage Liver Diseases (2) - HMUDocument31 pages3rd Stage Liver Diseases (2) - HMUjwan ahmedNo ratings yet
- Biliary CirrhosisDocument11 pagesBiliary CirrhosisradistryaNo ratings yet
- Liver Cirrhosis and Hepatocellular FailureDocument36 pagesLiver Cirrhosis and Hepatocellular FailureLedia EssamNo ratings yet
- Classic Diseases Revisited Liver Cirrhosis: PreviouslyDocument10 pagesClassic Diseases Revisited Liver Cirrhosis: PreviouslyFrancescaNo ratings yet
- Chronic Liver Disease - StatPearls - NCBI Bookshelf PDFDocument13 pagesChronic Liver Disease - StatPearls - NCBI Bookshelf PDFAdriana Margarita María Trejos TenorioNo ratings yet
- 12.pathology of The LiverDocument67 pages12.pathology of The LiverBlessings Thummim ChiumiaNo ratings yet
- The Liver and The Biliary TractDocument109 pagesThe Liver and The Biliary TractKw ChanNo ratings yet
- Chronic Liver DiseaseDocument20 pagesChronic Liver DiseaseDastogir AlamNo ratings yet
- Cirrosis HepaticaDocument10 pagesCirrosis Hepaticaadriel710No ratings yet
- Cirrhosis of LiverDocument35 pagesCirrhosis of LiverShazia Parveen100% (1)
- Systemic Path Slides Final-By A Student PDFDocument60 pagesSystemic Path Slides Final-By A Student PDFpixey55No ratings yet
- Liver CirrhosisDocument5 pagesLiver CirrhosisBerkah MilleniumNo ratings yet
- 3 - Hepato-Pancreato-Biliary Diseases 2.4 (2024)Document60 pages3 - Hepato-Pancreato-Biliary Diseases 2.4 (2024)R. nounNo ratings yet
- Disorders and Drugs That Can Cause Hepatic Fibrosis: PathophysiologyDocument3 pagesDisorders and Drugs That Can Cause Hepatic Fibrosis: PathophysiologyJazelyn Mae UyNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverpakdejackNo ratings yet
- Cirrhosis Jol 2009Document54 pagesCirrhosis Jol 2009SaaraAlleyahAlAnazi100% (1)
- Renal PathologyDocument34 pagesRenal PathologyShanaz ShaxawanNo ratings yet
- Portal Hypertension and Cirrhosis: Key ConceptsDocument16 pagesPortal Hypertension and Cirrhosis: Key ConceptsWa Ode FasridaNo ratings yet
- Seminar: Detlef Schuppan, Nezam H AfdhalDocument14 pagesSeminar: Detlef Schuppan, Nezam H AfdhalJonathan Arif PutraNo ratings yet
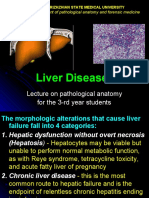
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument27 pagesLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Document72 pagesWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Darin MonerNo ratings yet
- Liver CirrhosisDocument6 pagesLiver CirrhosisBaharudin WahyuNo ratings yet
- Acknowledgement ReceiptDocument21 pagesAcknowledgement ReceiptdeevoncNo ratings yet
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDocument33 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDonto KonoNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Intrahepatic Cholestasis in Common Chronic Liver Diseases: ReviewDocument15 pagesIntrahepatic Cholestasis in Common Chronic Liver Diseases: Reviewzendah123No ratings yet
- Pathology B Finals RatioDocument56 pagesPathology B Finals RatioLemuel ValerioNo ratings yet
- Wen CZ 2014 WJG 20 7312 Patogenesis of Liver CirrhocisDocument14 pagesWen CZ 2014 WJG 20 7312 Patogenesis of Liver CirrhocisViola Shawolmagnaejuliettetaemin SaranghaeyonanamjaNo ratings yet
- Sirosis Hepatis Review JurnalDocument6 pagesSirosis Hepatis Review JurnalNadhila ByantNo ratings yet
- Liver CirrhosisDocument5 pagesLiver Cirrhosisdewi tanjungNo ratings yet
- Hepatic CirrhosisDocument20 pagesHepatic CirrhosisAnifowose samsonNo ratings yet
- Cirrosis Adnd Its ComplicationDocument50 pagesCirrosis Adnd Its Complicationnathan asfahaNo ratings yet
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDateDocument41 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDateMiraf MesfinNo ratings yet
- Bab IDocument30 pagesBab IInesia Putri WulandariNo ratings yet
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSDocument66 pagesSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmNo ratings yet
- Robbin's Chapter 20 Kidney PathologyDocument4 pagesRobbin's Chapter 20 Kidney Pathologynbaumgartner0100% (1)
- Cureus 0014 00000022733Document6 pagesCureus 0014 00000022733Dede IskandarNo ratings yet
- Liver Metastasis - NAFLD NASHDocument2 pagesLiver Metastasis - NAFLD NASHrafael514No ratings yet
- Cirrosis LANCET 2008Document14 pagesCirrosis LANCET 2008Natalia ElizabethNo ratings yet
- Budd - Chiari (Hepatic VenousDocument43 pagesBudd - Chiari (Hepatic VenousRamy ElbarodyNo ratings yet
- Renal DiseaseDocument191 pagesRenal Diseasetokkeetak13No ratings yet
- Cirrhosis and Its Complications: Further ReadingDocument10 pagesCirrhosis and Its Complications: Further ReadingJacob BorongNo ratings yet
- The Hepatobiliary System: by DR - Varughese George Department of PathologyDocument29 pagesThe Hepatobiliary System: by DR - Varughese George Department of PathologyRahulNo ratings yet
- GallbladderDocument44 pagesGallbladderAli SafaaNo ratings yet
- Cirrhosis - Wikipedia, The ...Document11 pagesCirrhosis - Wikipedia, The ...PrakashNo ratings yet
- Hepatocellular CarcinomaDocument9 pagesHepatocellular CarcinomaGeorge WinchesterNo ratings yet
- Primary Biliary Cirrhosis and Other Ductopenic Diseases: Alastair D. Burt, BSC, MD CHB, Frcpath, FibiolDocument18 pagesPrimary Biliary Cirrhosis and Other Ductopenic Diseases: Alastair D. Burt, BSC, MD CHB, Frcpath, Fibiollourdes marquezNo ratings yet
- Station 5 Cases 4Document73 pagesStation 5 Cases 4Sagit Nauman81100% (1)
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis PDFDocument36 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis PDFAhraxazel Galicia ReynaNo ratings yet
- Hepatitis ABCDEDocument9 pagesHepatitis ABCDEAnish SharmaNo ratings yet
- Hepatic FibrogenesisDocument10 pagesHepatic FibrogenesisPawan KumarNo ratings yet
- Liver Transplant Workup: IntroductionDocument9 pagesLiver Transplant Workup: IntroductionKay BristolNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- The Evolving Landscape of Liver Cirrhosis ManagementFrom EverandThe Evolving Landscape of Liver Cirrhosis ManagementHitoshi YoshijiNo ratings yet
- Hospice SynopsisDocument6 pagesHospice SynopsisPhalguna NaiduNo ratings yet
- Gill Disease in Barramundi (Lates Calcarifer)Document228 pagesGill Disease in Barramundi (Lates Calcarifer)mmsfNo ratings yet
- 04-46 Analysis of Gold-Copper Braze Joint in Glidcop For UHV Components at The APS W.Toter S.SharmaDocument10 pages04-46 Analysis of Gold-Copper Braze Joint in Glidcop For UHV Components at The APS W.Toter S.SharmaKai XuNo ratings yet
- ANSWERS For ExercisesDocument13 pagesANSWERS For ExercisesAlia HazwaniNo ratings yet
- PTS MATH GRADE 3 ICP (2022-2023) - Abidah FixDocument4 pagesPTS MATH GRADE 3 ICP (2022-2023) - Abidah FixAnita Noor Maidah S.Pd.i. SD Lab UMNo ratings yet
- Drainage Below GroundDocument5 pagesDrainage Below GroundmisharyNo ratings yet
- Experiencing Postsocialist CapitalismDocument251 pagesExperiencing Postsocialist CapitalismjelisNo ratings yet
- Montessori ObservationsDocument7 pagesMontessori Observationsapi-439426688No ratings yet
- Whittaker Dynamics 17Document442 pagesWhittaker Dynamics 17Mahmoud Ahmed 202201238No ratings yet
- MTT Assay To Evaluate The Cytotoxic Potential of A DrugDocument5 pagesMTT Assay To Evaluate The Cytotoxic Potential of A DrugThanh KieuNo ratings yet
- Effective Phone and Door Scripts 0Document6 pagesEffective Phone and Door Scripts 0Kaso MuseNo ratings yet
- EC Physical Sciences Grade 11 November 2022 P1 and MemoDocument25 pagesEC Physical Sciences Grade 11 November 2022 P1 and MemokhulntandoNo ratings yet
- PLC - HMI Lab #4 22W1Document2 pagesPLC - HMI Lab #4 22W1crazyjmprNo ratings yet
- Indian Standard: Methods of Test For Stabilized SoilsDocument10 pagesIndian Standard: Methods of Test For Stabilized Soilsphanendra kumarNo ratings yet
- 1231.322 323 MSDS Sabroe 1507-100 MSDSDocument6 pages1231.322 323 MSDS Sabroe 1507-100 MSDSzhyhhNo ratings yet
- SoftOne BlackBook ENG Ver.3.3 PDFDocument540 pagesSoftOne BlackBook ENG Ver.3.3 PDFLiviu BuliganNo ratings yet
- SAILOR 6081 Power Supply Unit and Charger: Installation ManualDocument72 pagesSAILOR 6081 Power Supply Unit and Charger: Installation ManualMariosNo ratings yet
- Ericka Joyce O. Reynera: PERSONAL - INFORMATIONDocument2 pagesEricka Joyce O. Reynera: PERSONAL - INFORMATIONdead insideNo ratings yet
- VIETNAM. PROCESSING OF AROMA CHEMICALS AND FRAGRANCE MATERIALS. TECHNICAL REPORT - AROMA CHEMICALS AND PERFUME BLENDING (20598.en) PDFDocument83 pagesVIETNAM. PROCESSING OF AROMA CHEMICALS AND FRAGRANCE MATERIALS. TECHNICAL REPORT - AROMA CHEMICALS AND PERFUME BLENDING (20598.en) PDFOsamaAliMoussaNo ratings yet
- Nemo Complete Documentation 2017Document65 pagesNemo Complete Documentation 2017Fredy A. CastañedaNo ratings yet
- Mapeh GR9 First Quarter ReviewerDocument8 pagesMapeh GR9 First Quarter ReviewerRalph Emerson SantillanNo ratings yet
- Channel DecisionsDocument30 pagesChannel Decisionsuzmatabassum1996No ratings yet
- 10 Science NcertSolutions Chapter 8 ExercisesDocument4 pages10 Science NcertSolutions Chapter 8 ExercisesAnita GargNo ratings yet
- Christmas Vigil MassDocument106 pagesChristmas Vigil MassMary JosephNo ratings yet
- English For ITDocument276 pagesEnglish For ITBao Tram100% (1)
- Form Service A40gDocument1 pageForm Service A40gBrando ImanuelNo ratings yet
- Philippine Statistics Authority: Date (2021)Document9 pagesPhilippine Statistics Authority: Date (2021)Nah ReeNo ratings yet























































































Download as ppt, pdf, or txt
You might also like
- Project-Charter (Mohammad Adnan)Document4 pagesProject-Charter (Mohammad Adnan)Mohammad Adnan80% (5)
- A Complete Neurological Nursing Assessment GuideDocument57 pagesA Complete Neurological Nursing Assessment GuideSarithaRajeshNo ratings yet
- List of Government WebsitesDocument1 pageList of Government Websitessumit-7No ratings yet
- Hydrolysis of Nucleic AcidsDocument7 pagesHydrolysis of Nucleic Acidskeepersake81% (16)
- Cirrhosis - Hepatic and Biliary Disorders - MSD Manual Professional EditionDocument9 pagesCirrhosis - Hepatic and Biliary Disorders - MSD Manual Professional EditionSky ShieldNo ratings yet
- L10 - Liver CirrhosisDocument10 pagesL10 - Liver CirrhosisMerehan El RoosNo ratings yet
- Cirrhosis: DR AkhondeiDocument111 pagesCirrhosis: DR AkhondeiMuvenn KannanNo ratings yet
- The Pathogenesis of Liver Cirrhosis / Fibrosis: Dr. Indranil BhattacharyaDocument46 pagesThe Pathogenesis of Liver Cirrhosis / Fibrosis: Dr. Indranil BhattacharyaDr. Indranil BhattacharayaNo ratings yet
- Cirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverDocument29 pagesCirrhosis: Author: David C Wolf, MD, FACP, FACG, AGAF, Medical Director of LiverdahsyatnyaNo ratings yet
- 3rd Stage Liver Diseases (2) - HMUDocument31 pages3rd Stage Liver Diseases (2) - HMUjwan ahmedNo ratings yet
- Biliary CirrhosisDocument11 pagesBiliary CirrhosisradistryaNo ratings yet
- Liver Cirrhosis and Hepatocellular FailureDocument36 pagesLiver Cirrhosis and Hepatocellular FailureLedia EssamNo ratings yet
- Classic Diseases Revisited Liver Cirrhosis: PreviouslyDocument10 pagesClassic Diseases Revisited Liver Cirrhosis: PreviouslyFrancescaNo ratings yet
- Chronic Liver Disease - StatPearls - NCBI Bookshelf PDFDocument13 pagesChronic Liver Disease - StatPearls - NCBI Bookshelf PDFAdriana Margarita María Trejos TenorioNo ratings yet
- 12.pathology of The LiverDocument67 pages12.pathology of The LiverBlessings Thummim ChiumiaNo ratings yet
- The Liver and The Biliary TractDocument109 pagesThe Liver and The Biliary TractKw ChanNo ratings yet
- Chronic Liver DiseaseDocument20 pagesChronic Liver DiseaseDastogir AlamNo ratings yet
- Cirrosis HepaticaDocument10 pagesCirrosis Hepaticaadriel710No ratings yet
- Cirrhosis of LiverDocument35 pagesCirrhosis of LiverShazia Parveen100% (1)
- Systemic Path Slides Final-By A Student PDFDocument60 pagesSystemic Path Slides Final-By A Student PDFpixey55No ratings yet
- Liver CirrhosisDocument5 pagesLiver CirrhosisBerkah MilleniumNo ratings yet
- 3 - Hepato-Pancreato-Biliary Diseases 2.4 (2024)Document60 pages3 - Hepato-Pancreato-Biliary Diseases 2.4 (2024)R. nounNo ratings yet
- Disorders and Drugs That Can Cause Hepatic Fibrosis: PathophysiologyDocument3 pagesDisorders and Drugs That Can Cause Hepatic Fibrosis: PathophysiologyJazelyn Mae UyNo ratings yet
- Cirrhosis of LiverDocument6 pagesCirrhosis of LiverpakdejackNo ratings yet
- Cirrhosis Jol 2009Document54 pagesCirrhosis Jol 2009SaaraAlleyahAlAnazi100% (1)
- Renal PathologyDocument34 pagesRenal PathologyShanaz ShaxawanNo ratings yet
- Portal Hypertension and Cirrhosis: Key ConceptsDocument16 pagesPortal Hypertension and Cirrhosis: Key ConceptsWa Ode FasridaNo ratings yet
- Seminar: Detlef Schuppan, Nezam H AfdhalDocument14 pagesSeminar: Detlef Schuppan, Nezam H AfdhalJonathan Arif PutraNo ratings yet
- Liver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsDocument27 pagesLiver Diseases: Lecture On Pathological Anatomy For The 3-rd Year StudentsRodriguez Vivanco Kevin DanielNo ratings yet
- With Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Document72 pagesWith Ordinary Talent and Extraordinary Perseverance, All Things Are Attainable.Darin MonerNo ratings yet
- Liver CirrhosisDocument6 pagesLiver CirrhosisBaharudin WahyuNo ratings yet
- Acknowledgement ReceiptDocument21 pagesAcknowledgement ReceiptdeevoncNo ratings yet
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDocument33 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDonto KonoNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Intrahepatic Cholestasis in Common Chronic Liver Diseases: ReviewDocument15 pagesIntrahepatic Cholestasis in Common Chronic Liver Diseases: Reviewzendah123No ratings yet
- Pathology B Finals RatioDocument56 pagesPathology B Finals RatioLemuel ValerioNo ratings yet
- Wen CZ 2014 WJG 20 7312 Patogenesis of Liver CirrhocisDocument14 pagesWen CZ 2014 WJG 20 7312 Patogenesis of Liver CirrhocisViola Shawolmagnaejuliettetaemin SaranghaeyonanamjaNo ratings yet
- Sirosis Hepatis Review JurnalDocument6 pagesSirosis Hepatis Review JurnalNadhila ByantNo ratings yet
- Liver CirrhosisDocument5 pagesLiver Cirrhosisdewi tanjungNo ratings yet
- Hepatic CirrhosisDocument20 pagesHepatic CirrhosisAnifowose samsonNo ratings yet
- Cirrosis Adnd Its ComplicationDocument50 pagesCirrosis Adnd Its Complicationnathan asfahaNo ratings yet
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDateDocument41 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDateMiraf MesfinNo ratings yet
- Bab IDocument30 pagesBab IInesia Putri WulandariNo ratings yet
- Sirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSDocument66 pagesSirosis Hepatis: Sigit Widyatmoko Fakultas Kedokteran UMSArif Rahman DmNo ratings yet
- Robbin's Chapter 20 Kidney PathologyDocument4 pagesRobbin's Chapter 20 Kidney Pathologynbaumgartner0100% (1)
- Cureus 0014 00000022733Document6 pagesCureus 0014 00000022733Dede IskandarNo ratings yet
- Liver Metastasis - NAFLD NASHDocument2 pagesLiver Metastasis - NAFLD NASHrafael514No ratings yet
- Cirrosis LANCET 2008Document14 pagesCirrosis LANCET 2008Natalia ElizabethNo ratings yet
- Budd - Chiari (Hepatic VenousDocument43 pagesBudd - Chiari (Hepatic VenousRamy ElbarodyNo ratings yet
- Renal DiseaseDocument191 pagesRenal Diseasetokkeetak13No ratings yet
- Cirrhosis and Its Complications: Further ReadingDocument10 pagesCirrhosis and Its Complications: Further ReadingJacob BorongNo ratings yet
- The Hepatobiliary System: by DR - Varughese George Department of PathologyDocument29 pagesThe Hepatobiliary System: by DR - Varughese George Department of PathologyRahulNo ratings yet
- GallbladderDocument44 pagesGallbladderAli SafaaNo ratings yet
- Cirrhosis - Wikipedia, The ...Document11 pagesCirrhosis - Wikipedia, The ...PrakashNo ratings yet
- Hepatocellular CarcinomaDocument9 pagesHepatocellular CarcinomaGeorge WinchesterNo ratings yet
- Primary Biliary Cirrhosis and Other Ductopenic Diseases: Alastair D. Burt, BSC, MD CHB, Frcpath, FibiolDocument18 pagesPrimary Biliary Cirrhosis and Other Ductopenic Diseases: Alastair D. Burt, BSC, MD CHB, Frcpath, Fibiollourdes marquezNo ratings yet
- Station 5 Cases 4Document73 pagesStation 5 Cases 4Sagit Nauman81100% (1)
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis PDFDocument36 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis PDFAhraxazel Galicia ReynaNo ratings yet
- Hepatitis ABCDEDocument9 pagesHepatitis ABCDEAnish SharmaNo ratings yet
- Hepatic FibrogenesisDocument10 pagesHepatic FibrogenesisPawan KumarNo ratings yet
- Liver Transplant Workup: IntroductionDocument9 pagesLiver Transplant Workup: IntroductionKay BristolNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- The Evolving Landscape of Liver Cirrhosis ManagementFrom EverandThe Evolving Landscape of Liver Cirrhosis ManagementHitoshi YoshijiNo ratings yet
- Hospice SynopsisDocument6 pagesHospice SynopsisPhalguna NaiduNo ratings yet
- Gill Disease in Barramundi (Lates Calcarifer)Document228 pagesGill Disease in Barramundi (Lates Calcarifer)mmsfNo ratings yet
- 04-46 Analysis of Gold-Copper Braze Joint in Glidcop For UHV Components at The APS W.Toter S.SharmaDocument10 pages04-46 Analysis of Gold-Copper Braze Joint in Glidcop For UHV Components at The APS W.Toter S.SharmaKai XuNo ratings yet
- ANSWERS For ExercisesDocument13 pagesANSWERS For ExercisesAlia HazwaniNo ratings yet
- PTS MATH GRADE 3 ICP (2022-2023) - Abidah FixDocument4 pagesPTS MATH GRADE 3 ICP (2022-2023) - Abidah FixAnita Noor Maidah S.Pd.i. SD Lab UMNo ratings yet
- Drainage Below GroundDocument5 pagesDrainage Below GroundmisharyNo ratings yet
- Experiencing Postsocialist CapitalismDocument251 pagesExperiencing Postsocialist CapitalismjelisNo ratings yet
- Montessori ObservationsDocument7 pagesMontessori Observationsapi-439426688No ratings yet
- Whittaker Dynamics 17Document442 pagesWhittaker Dynamics 17Mahmoud Ahmed 202201238No ratings yet
- MTT Assay To Evaluate The Cytotoxic Potential of A DrugDocument5 pagesMTT Assay To Evaluate The Cytotoxic Potential of A DrugThanh KieuNo ratings yet
- Effective Phone and Door Scripts 0Document6 pagesEffective Phone and Door Scripts 0Kaso MuseNo ratings yet
- EC Physical Sciences Grade 11 November 2022 P1 and MemoDocument25 pagesEC Physical Sciences Grade 11 November 2022 P1 and MemokhulntandoNo ratings yet
- PLC - HMI Lab #4 22W1Document2 pagesPLC - HMI Lab #4 22W1crazyjmprNo ratings yet
- Indian Standard: Methods of Test For Stabilized SoilsDocument10 pagesIndian Standard: Methods of Test For Stabilized Soilsphanendra kumarNo ratings yet
- 1231.322 323 MSDS Sabroe 1507-100 MSDSDocument6 pages1231.322 323 MSDS Sabroe 1507-100 MSDSzhyhhNo ratings yet
- SoftOne BlackBook ENG Ver.3.3 PDFDocument540 pagesSoftOne BlackBook ENG Ver.3.3 PDFLiviu BuliganNo ratings yet
- SAILOR 6081 Power Supply Unit and Charger: Installation ManualDocument72 pagesSAILOR 6081 Power Supply Unit and Charger: Installation ManualMariosNo ratings yet
- Ericka Joyce O. Reynera: PERSONAL - INFORMATIONDocument2 pagesEricka Joyce O. Reynera: PERSONAL - INFORMATIONdead insideNo ratings yet
- VIETNAM. PROCESSING OF AROMA CHEMICALS AND FRAGRANCE MATERIALS. TECHNICAL REPORT - AROMA CHEMICALS AND PERFUME BLENDING (20598.en) PDFDocument83 pagesVIETNAM. PROCESSING OF AROMA CHEMICALS AND FRAGRANCE MATERIALS. TECHNICAL REPORT - AROMA CHEMICALS AND PERFUME BLENDING (20598.en) PDFOsamaAliMoussaNo ratings yet
- Nemo Complete Documentation 2017Document65 pagesNemo Complete Documentation 2017Fredy A. CastañedaNo ratings yet
- Mapeh GR9 First Quarter ReviewerDocument8 pagesMapeh GR9 First Quarter ReviewerRalph Emerson SantillanNo ratings yet
- Channel DecisionsDocument30 pagesChannel Decisionsuzmatabassum1996No ratings yet
- 10 Science NcertSolutions Chapter 8 ExercisesDocument4 pages10 Science NcertSolutions Chapter 8 ExercisesAnita GargNo ratings yet
- Christmas Vigil MassDocument106 pagesChristmas Vigil MassMary JosephNo ratings yet
- English For ITDocument276 pagesEnglish For ITBao Tram100% (1)
- Form Service A40gDocument1 pageForm Service A40gBrando ImanuelNo ratings yet
- Philippine Statistics Authority: Date (2021)Document9 pagesPhilippine Statistics Authority: Date (2021)Nah ReeNo ratings yet