
Met Caz Clinic
Met Caz Clinic
You might also like
- MRI Study GuideDocument66 pagesMRI Study GuideJuan Doval100% (7)
- RMO Handbook AussieDocument48 pagesRMO Handbook Aussienvrtm43No ratings yet
- Case Analysis: Arnold Palmer HospitalDocument20 pagesCase Analysis: Arnold Palmer HospitalAlexis Rebano100% (3)
- T5 Pancreas PDFDocument19 pagesT5 Pancreas PDFAmin ZahariNo ratings yet
- Imaging in Chronic PancreatitisDocument7 pagesImaging in Chronic Pancreatitisdesy 102017135No ratings yet
- Carcinoma StomachDocument51 pagesCarcinoma StomachOnkar SinghNo ratings yet
- Css CT Scan AbdomenDocument54 pagesCss CT Scan AbdomenUlfa DiyaNo ratings yet
- Tumors of Pancreas DR DilberDocument51 pagesTumors of Pancreas DR Dilberdrdilber100% (2)
- en Papilla Vaters Tumor in Elderly An InterDocument5 pagesen Papilla Vaters Tumor in Elderly An InterAyip Bahsan AlBantaniNo ratings yet
- Roys Pangayoman, DR., SPBDocument45 pagesRoys Pangayoman, DR., SPBIdham Muhammad100% (1)
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantVasanth MalagiNo ratings yet
- Sajid SurgeryDocument42 pagesSajid SurgerySajidNo ratings yet
- KlatskinDocument24 pagesKlatskinArian WawolumajaNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyMolla WariNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Case Report: Pancreas As Delayed Site of Metastasis From Papillary Thyroid CarcinomaDocument4 pagesCase Report: Pancreas As Delayed Site of Metastasis From Papillary Thyroid CarcinomaTri Rahma Yani YawatiNo ratings yet
- Amma 2018 0026Document4 pagesAmma 2018 0026Dan CretuNo ratings yet
- Gastriccancer 160428190410Document54 pagesGastriccancer 160428190410Pranavi ShewaleNo ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantDaniel Alfredo Tenorio GonzálezNo ratings yet
- DuodenalcarcinoidDocument5 pagesDuodenalcarcinoidMudassar SattarNo ratings yet
- CA Stomach OverviewDocument84 pagesCA Stomach OverviewDr Shafiq Ahmad ChughtaiNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: Ultrasonographynarsing59No ratings yet
- s13304 011 0131 2 PDFDocument3 pagess13304 011 0131 2 PDFRoderick Núñez JNo ratings yet
- Rez Ect I I Pancreatic Ed Rep TeDocument10 pagesRez Ect I I Pancreatic Ed Rep TestelixxNo ratings yet
- CNP - AjDocument33 pagesCNP - AjeviltohuntNo ratings yet
- Pancreas: DR Sigid Djuniawan, SPBDocument40 pagesPancreas: DR Sigid Djuniawan, SPBditaayupNo ratings yet
- Colon ImagingDocument24 pagesColon ImagingShahla RasulNo ratings yet
- Jurding BedahDocument18 pagesJurding BedahSharon Natalia RuntulaloNo ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
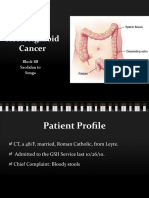
- Rectosigmoid Cancer: Block 8B Sacdalan To SengaDocument58 pagesRectosigmoid Cancer: Block 8B Sacdalan To SengaAngeli-Tristel SaquitanNo ratings yet
- CPC PancreatitisDocument67 pagesCPC PancreatitisM. Baidar SaeedNo ratings yet
- 1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFDocument4 pages1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFNawzad SulayvaniNo ratings yet
- Gastrointestinal Surgery Rounds: Dr. Twinkle Parekh Moderator - Dr. Satish S.NDocument112 pagesGastrointestinal Surgery Rounds: Dr. Twinkle Parekh Moderator - Dr. Satish S.NNaveen PentakotaNo ratings yet
- Cystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationDocument20 pagesCystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationVictor Kenzo IvanoNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- 10 StomachDocument10 pages10 StomachApabrita KarmakarNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- Groove Pancreatitis - Cause of Recurrent PancreatitisDocument7 pagesGroove Pancreatitis - Cause of Recurrent PancreatitisroxxanaNo ratings yet
- Carcinoma Esophagus: Presented byDocument59 pagesCarcinoma Esophagus: Presented byBayarbaatar BoldNo ratings yet
- Esophageal Cancer SuyogDocument46 pagesEsophageal Cancer SuyogUsmle GuyNo ratings yet
- 97438-Article Text-254324-1-10-20131121Document2 pages97438-Article Text-254324-1-10-20131121June Faith HacheroNo ratings yet
- Referat CA PancreasDocument25 pagesReferat CA PancreasPamela VasikhaNo ratings yet
- Oesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Document71 pagesOesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Abhishek KumarNo ratings yet
- 20.MBBS Pancreatic CancerDocument52 pages20.MBBS Pancreatic Cancermrajah95No ratings yet
- Yamao 2003Document5 pagesYamao 2003Patricia BezneaNo ratings yet
- Jurnal 7Document3 pagesJurnal 7rahayuNo ratings yet
- OvaryDocument4 pagesOvaryCarolina MartinezNo ratings yet
- Neoplasma of PankreasDocument33 pagesNeoplasma of PankreasGina Sonia RahmahNo ratings yet
- Jurnal Radiologi FixDocument44 pagesJurnal Radiologi FixAfifa Prima GittaNo ratings yet
- Pancreatic CancerDocument6 pagesPancreatic CancermillexaNo ratings yet
- Colorectal Cancer: - Dr. Suneet KhuranaDocument36 pagesColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNo ratings yet
- Pancreatic PathologyDocument7 pagesPancreatic Pathologyzeroun24100% (1)
- Case Presentation:: DR - Amra Farrukh PG.T Su.IDocument75 pagesCase Presentation:: DR - Amra Farrukh PG.T Su.IpeeconNo ratings yet
- Gastric Schwannoma: MRI Findings: Case ReportDocument3 pagesGastric Schwannoma: MRI Findings: Case ReportjihaneNo ratings yet
- Aghiz 3Document12 pagesAghiz 3nandaaa aprilNo ratings yet
- Initial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsDocument33 pagesInitial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsClaudia YalanNo ratings yet
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- RIZ - Enterocutaneous FistulaDocument35 pagesRIZ - Enterocutaneous FistulaAdiwirya AristiaraNo ratings yet
- Clinical and Radiological Features of Mesenteric Panniculitis: A Critical OverviewDocument12 pagesClinical and Radiological Features of Mesenteric Panniculitis: A Critical OverviewriyanysidikNo ratings yet
- Diseases of Esophagus: I. GeneralDocument4 pagesDiseases of Esophagus: I. GeneralAdilMoumnaNo ratings yet
- Cancer of PancreasDocument50 pagesCancer of PancreasIsaac MwangiNo ratings yet
- Gastric CarcinomaDocument43 pagesGastric CarcinomaPragadeswaran SNo ratings yet
- Endoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyFrom EverandEndoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyAntonio FacciorussoNo ratings yet
- Raleigh Brown Manual Project Final 1Document16 pagesRaleigh Brown Manual Project Final 1api-456848393No ratings yet
- Neurosurgeon Under Shadow of Covid 19Document2 pagesNeurosurgeon Under Shadow of Covid 19salikaabrarNo ratings yet
- CPR Logo - Google SearchDocument1 pageCPR Logo - Google SearchRola MohammadNo ratings yet
- Mycoplasma in PoultryDocument31 pagesMycoplasma in PoultryLalit ChaudhariNo ratings yet
- TMP DEDADocument8 pagesTMP DEDAFrontiersNo ratings yet
- Lapsus Kaki DiabetikDocument53 pagesLapsus Kaki DiabetikAhdiat Sang MantanNo ratings yet
- Pediatric Cystoscope OlympusDocument4 pagesPediatric Cystoscope Olympusgoutham sivasailamNo ratings yet
- The Only NGO Working in Kashmir in The Feild of Drug Abuse PreventionDocument2 pagesThe Only NGO Working in Kashmir in The Feild of Drug Abuse Preventionhnssdar100% (3)
- FS For SubmissionDocument79 pagesFS For SubmissionJosephine Policar0% (1)
- EC Disability Benefits Form (20210914-ECC-IBCP-HCPI-III) 2Document3 pagesEC Disability Benefits Form (20210914-ECC-IBCP-HCPI-III) 2FreitzNo ratings yet
- Bifocal Contact Lenses PDFDocument10 pagesBifocal Contact Lenses PDFLauw Dwi AndrikNo ratings yet
- Qeh Ambulatory Care ServicesDocument2 pagesQeh Ambulatory Care Servicesrobinmilton1998No ratings yet
- DVT DR Moses KazeevuDocument24 pagesDVT DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Cooper, Mick (2011) - Meeting The Demand For Evidence Based Practice. Therapy Today 22Document9 pagesCooper, Mick (2011) - Meeting The Demand For Evidence Based Practice. Therapy Today 22Arina IulianaNo ratings yet
- Ortho13 14Document64 pagesOrtho13 14priyasargunan100% (4)
- Institutional Pharmacy: Continuation of MARS/TARSDocument17 pagesInstitutional Pharmacy: Continuation of MARS/TARScoastalcitiessNo ratings yet
- Alithera Eng Version 20220207Document20 pagesAlithera Eng Version 20220207mohd aminNo ratings yet
- 20 Trapozzano and Lazzari. A Study of Hinge Axis Determination. JPD 11 (5) - 858-863, 1961Document6 pages20 Trapozzano and Lazzari. A Study of Hinge Axis Determination. JPD 11 (5) - 858-863, 1961Ful WgNo ratings yet
- Synopsis - Priti - Whole Document PDFDocument11 pagesSynopsis - Priti - Whole Document PDFelixir indiaNo ratings yet
- Gyentics-Catalogus Volledig 06-2019 LR PDFDocument42 pagesGyentics-Catalogus Volledig 06-2019 LR PDFAhad M AhmedNo ratings yet
- EKG Self Study GuideDocument40 pagesEKG Self Study GuideArgee AlonsabeNo ratings yet
- MaxigardDocument17 pagesMaxigardrizqi dwikiNo ratings yet
- IjhsDocument10 pagesIjhsAnamika SinhaNo ratings yet
- Better Homes & Gardens Eat To Feel Good - 2018Document100 pagesBetter Homes & Gardens Eat To Feel Good - 2018steve hope100% (1)
- PiperacillinDocument3 pagesPiperacillinmyer pasandalanNo ratings yet
- Nihon Kohden Eeg Meb 2300KDocument23 pagesNihon Kohden Eeg Meb 2300KSulay Avila LlanosNo ratings yet
- Kenalog Injection PiDocument1 pageKenalog Injection PiSam ヅ VeliNo ratings yet























































































Download as ppt, pdf, or txt
You might also like
- MRI Study GuideDocument66 pagesMRI Study GuideJuan Doval100% (7)
- RMO Handbook AussieDocument48 pagesRMO Handbook Aussienvrtm43No ratings yet
- Case Analysis: Arnold Palmer HospitalDocument20 pagesCase Analysis: Arnold Palmer HospitalAlexis Rebano100% (3)
- T5 Pancreas PDFDocument19 pagesT5 Pancreas PDFAmin ZahariNo ratings yet
- Imaging in Chronic PancreatitisDocument7 pagesImaging in Chronic Pancreatitisdesy 102017135No ratings yet
- Carcinoma StomachDocument51 pagesCarcinoma StomachOnkar SinghNo ratings yet
- Css CT Scan AbdomenDocument54 pagesCss CT Scan AbdomenUlfa DiyaNo ratings yet
- Tumors of Pancreas DR DilberDocument51 pagesTumors of Pancreas DR Dilberdrdilber100% (2)
- en Papilla Vaters Tumor in Elderly An InterDocument5 pagesen Papilla Vaters Tumor in Elderly An InterAyip Bahsan AlBantaniNo ratings yet
- Roys Pangayoman, DR., SPBDocument45 pagesRoys Pangayoman, DR., SPBIdham Muhammad100% (1)
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantVasanth MalagiNo ratings yet
- Sajid SurgeryDocument42 pagesSajid SurgerySajidNo ratings yet
- KlatskinDocument24 pagesKlatskinArian WawolumajaNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyMolla WariNo ratings yet
- Carcinoma Gall BladderDocument25 pagesCarcinoma Gall Bladderrajan kumarNo ratings yet
- Case Report: Pancreas As Delayed Site of Metastasis From Papillary Thyroid CarcinomaDocument4 pagesCase Report: Pancreas As Delayed Site of Metastasis From Papillary Thyroid CarcinomaTri Rahma Yani YawatiNo ratings yet
- Amma 2018 0026Document4 pagesAmma 2018 0026Dan CretuNo ratings yet
- Gastriccancer 160428190410Document54 pagesGastriccancer 160428190410Pranavi ShewaleNo ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantDaniel Alfredo Tenorio GonzálezNo ratings yet
- DuodenalcarcinoidDocument5 pagesDuodenalcarcinoidMudassar SattarNo ratings yet
- CA Stomach OverviewDocument84 pagesCA Stomach OverviewDr Shafiq Ahmad ChughtaiNo ratings yet
- Pancreatic Head Mass: What Can Be Done ? Diagnosis: UltrasonographyDocument4 pagesPancreatic Head Mass: What Can Be Done ? Diagnosis: Ultrasonographynarsing59No ratings yet
- s13304 011 0131 2 PDFDocument3 pagess13304 011 0131 2 PDFRoderick Núñez JNo ratings yet
- Rez Ect I I Pancreatic Ed Rep TeDocument10 pagesRez Ect I I Pancreatic Ed Rep TestelixxNo ratings yet
- CNP - AjDocument33 pagesCNP - AjeviltohuntNo ratings yet
- Pancreas: DR Sigid Djuniawan, SPBDocument40 pagesPancreas: DR Sigid Djuniawan, SPBditaayupNo ratings yet
- Colon ImagingDocument24 pagesColon ImagingShahla RasulNo ratings yet
- Jurding BedahDocument18 pagesJurding BedahSharon Natalia RuntulaloNo ratings yet
- Block 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May FahmiDocument96 pagesBlock 3.3 Sesi 3 Pathology of Urinary Tract: by Asdos 2011: Vetta Awe Eric Lily Fiko Ghana Ikal Linda May Fahmimail junkNo ratings yet
- Rectosigmoid Cancer: Block 8B Sacdalan To SengaDocument58 pagesRectosigmoid Cancer: Block 8B Sacdalan To SengaAngeli-Tristel SaquitanNo ratings yet
- CPC PancreatitisDocument67 pagesCPC PancreatitisM. Baidar SaeedNo ratings yet
- 1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFDocument4 pages1999-07 - Intraductal Papillary-Mucinous Tumor of The Pancreas - Presentation in A Young Adult PDFNawzad SulayvaniNo ratings yet
- Gastrointestinal Surgery Rounds: Dr. Twinkle Parekh Moderator - Dr. Satish S.NDocument112 pagesGastrointestinal Surgery Rounds: Dr. Twinkle Parekh Moderator - Dr. Satish S.NNaveen PentakotaNo ratings yet
- Cystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationDocument20 pagesCystic Lesions of The Pancreas - RadiologicEndosonographic CorrelationVictor Kenzo IvanoNo ratings yet
- Primary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportDocument6 pagesPrimary Congenital Choledochal Cyst With Squamous Cell Carcinoma: A Case ReportRais KhairuddinNo ratings yet
- 10 StomachDocument10 pages10 StomachApabrita KarmakarNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- Groove Pancreatitis - Cause of Recurrent PancreatitisDocument7 pagesGroove Pancreatitis - Cause of Recurrent PancreatitisroxxanaNo ratings yet
- Carcinoma Esophagus: Presented byDocument59 pagesCarcinoma Esophagus: Presented byBayarbaatar BoldNo ratings yet
- Esophageal Cancer SuyogDocument46 pagesEsophageal Cancer SuyogUsmle GuyNo ratings yet
- 97438-Article Text-254324-1-10-20131121Document2 pages97438-Article Text-254324-1-10-20131121June Faith HacheroNo ratings yet
- Referat CA PancreasDocument25 pagesReferat CA PancreasPamela VasikhaNo ratings yet
- Oesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Document71 pagesOesophageal Carcinom A & Its Managment: DR - Vivek Garg (JR-2) Dr. Mohd. Athar (Oncosurgeon)Abhishek KumarNo ratings yet
- 20.MBBS Pancreatic CancerDocument52 pages20.MBBS Pancreatic Cancermrajah95No ratings yet
- Yamao 2003Document5 pagesYamao 2003Patricia BezneaNo ratings yet
- Jurnal 7Document3 pagesJurnal 7rahayuNo ratings yet
- OvaryDocument4 pagesOvaryCarolina MartinezNo ratings yet
- Neoplasma of PankreasDocument33 pagesNeoplasma of PankreasGina Sonia RahmahNo ratings yet
- Jurnal Radiologi FixDocument44 pagesJurnal Radiologi FixAfifa Prima GittaNo ratings yet
- Pancreatic CancerDocument6 pagesPancreatic CancermillexaNo ratings yet
- Colorectal Cancer: - Dr. Suneet KhuranaDocument36 pagesColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNo ratings yet
- Pancreatic PathologyDocument7 pagesPancreatic Pathologyzeroun24100% (1)
- Case Presentation:: DR - Amra Farrukh PG.T Su.IDocument75 pagesCase Presentation:: DR - Amra Farrukh PG.T Su.IpeeconNo ratings yet
- Gastric Schwannoma: MRI Findings: Case ReportDocument3 pagesGastric Schwannoma: MRI Findings: Case ReportjihaneNo ratings yet
- Aghiz 3Document12 pagesAghiz 3nandaaa aprilNo ratings yet
- Initial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsDocument33 pagesInitial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsClaudia YalanNo ratings yet
- Pancreatic Adenocarcinoma Mimicking PseudocystDocument3 pagesPancreatic Adenocarcinoma Mimicking PseudocystInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- RIZ - Enterocutaneous FistulaDocument35 pagesRIZ - Enterocutaneous FistulaAdiwirya AristiaraNo ratings yet
- Clinical and Radiological Features of Mesenteric Panniculitis: A Critical OverviewDocument12 pagesClinical and Radiological Features of Mesenteric Panniculitis: A Critical OverviewriyanysidikNo ratings yet
- Diseases of Esophagus: I. GeneralDocument4 pagesDiseases of Esophagus: I. GeneralAdilMoumnaNo ratings yet
- Cancer of PancreasDocument50 pagesCancer of PancreasIsaac MwangiNo ratings yet
- Gastric CarcinomaDocument43 pagesGastric CarcinomaPragadeswaran SNo ratings yet
- Endoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyFrom EverandEndoscopic Ultrasound Management of Pancreatic Lesions: From Diagnosis to TherapyAntonio FacciorussoNo ratings yet
- Raleigh Brown Manual Project Final 1Document16 pagesRaleigh Brown Manual Project Final 1api-456848393No ratings yet
- Neurosurgeon Under Shadow of Covid 19Document2 pagesNeurosurgeon Under Shadow of Covid 19salikaabrarNo ratings yet
- CPR Logo - Google SearchDocument1 pageCPR Logo - Google SearchRola MohammadNo ratings yet
- Mycoplasma in PoultryDocument31 pagesMycoplasma in PoultryLalit ChaudhariNo ratings yet
- TMP DEDADocument8 pagesTMP DEDAFrontiersNo ratings yet
- Lapsus Kaki DiabetikDocument53 pagesLapsus Kaki DiabetikAhdiat Sang MantanNo ratings yet
- Pediatric Cystoscope OlympusDocument4 pagesPediatric Cystoscope Olympusgoutham sivasailamNo ratings yet
- The Only NGO Working in Kashmir in The Feild of Drug Abuse PreventionDocument2 pagesThe Only NGO Working in Kashmir in The Feild of Drug Abuse Preventionhnssdar100% (3)
- FS For SubmissionDocument79 pagesFS For SubmissionJosephine Policar0% (1)
- EC Disability Benefits Form (20210914-ECC-IBCP-HCPI-III) 2Document3 pagesEC Disability Benefits Form (20210914-ECC-IBCP-HCPI-III) 2FreitzNo ratings yet
- Bifocal Contact Lenses PDFDocument10 pagesBifocal Contact Lenses PDFLauw Dwi AndrikNo ratings yet
- Qeh Ambulatory Care ServicesDocument2 pagesQeh Ambulatory Care Servicesrobinmilton1998No ratings yet
- DVT DR Moses KazeevuDocument24 pagesDVT DR Moses KazeevuMoses Jr KazevuNo ratings yet
- Cooper, Mick (2011) - Meeting The Demand For Evidence Based Practice. Therapy Today 22Document9 pagesCooper, Mick (2011) - Meeting The Demand For Evidence Based Practice. Therapy Today 22Arina IulianaNo ratings yet
- Ortho13 14Document64 pagesOrtho13 14priyasargunan100% (4)
- Institutional Pharmacy: Continuation of MARS/TARSDocument17 pagesInstitutional Pharmacy: Continuation of MARS/TARScoastalcitiessNo ratings yet
- Alithera Eng Version 20220207Document20 pagesAlithera Eng Version 20220207mohd aminNo ratings yet
- 20 Trapozzano and Lazzari. A Study of Hinge Axis Determination. JPD 11 (5) - 858-863, 1961Document6 pages20 Trapozzano and Lazzari. A Study of Hinge Axis Determination. JPD 11 (5) - 858-863, 1961Ful WgNo ratings yet
- Synopsis - Priti - Whole Document PDFDocument11 pagesSynopsis - Priti - Whole Document PDFelixir indiaNo ratings yet
- Gyentics-Catalogus Volledig 06-2019 LR PDFDocument42 pagesGyentics-Catalogus Volledig 06-2019 LR PDFAhad M AhmedNo ratings yet
- EKG Self Study GuideDocument40 pagesEKG Self Study GuideArgee AlonsabeNo ratings yet
- MaxigardDocument17 pagesMaxigardrizqi dwikiNo ratings yet
- IjhsDocument10 pagesIjhsAnamika SinhaNo ratings yet
- Better Homes & Gardens Eat To Feel Good - 2018Document100 pagesBetter Homes & Gardens Eat To Feel Good - 2018steve hope100% (1)
- PiperacillinDocument3 pagesPiperacillinmyer pasandalanNo ratings yet
- Nihon Kohden Eeg Meb 2300KDocument23 pagesNihon Kohden Eeg Meb 2300KSulay Avila LlanosNo ratings yet
- Kenalog Injection PiDocument1 pageKenalog Injection PiSam ヅ VeliNo ratings yet