Download as pptx, pdf, or txt
You might also like
- Serve God, Save The Planet: A Christian Call To Action by Matthew Sleeth, M.D.Document45 pagesServe God, Save The Planet: A Christian Call To Action by Matthew Sleeth, M.D.Zondervan100% (2)
- Sics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraDocument74 pagesSics Steps: Divisi Katarak Dan Bedah Refraktif Rumah Sakit Mata Bali MandaraPande GustianaNo ratings yet
- 2012 BRAKES VSA System Components - TL PDFDocument114 pages2012 BRAKES VSA System Components - TL PDFsoftallNo ratings yet
- Argelander Initial InterviewDocument13 pagesArgelander Initial InterviewTiborNo ratings yet
- Primary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewDocument17 pagesPrimary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewPrabu Tirta AjiNo ratings yet
- Kraniotomi DekompresiDocument17 pagesKraniotomi DekompresianamselNo ratings yet
- Multi-Criteria Decision MakingDocument52 pagesMulti-Criteria Decision MakingD'Mhan Mbozo100% (1)
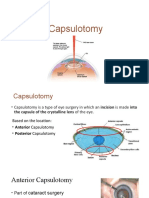
- CapsulotomyDocument15 pagesCapsulotomyAdrian PearlNo ratings yet
- Critical Appraisal KADocument35 pagesCritical Appraisal KAKentVilandkaNo ratings yet
- Materi KatarakDocument39 pagesMateri KatarakfebyNo ratings yet
- 1 - Perbandingan Teknik Endoscopic Third VentriculostomyDocument10 pages1 - Perbandingan Teknik Endoscopic Third VentriculostomyKathryn TurnerNo ratings yet
- Optokinetic Nystagmus TestDocument3 pagesOptokinetic Nystagmus TestRegina CaeciliaNo ratings yet
- Tangga Penutupan LukaDocument16 pagesTangga Penutupan Lukadonny valensiusNo ratings yet
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocument41 pagesAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junNo ratings yet
- Abnormal Chest FindingsDocument5 pagesAbnormal Chest FindingsAbishek Prince100% (1)
- Tutorial SSWALFA by IDI SurabayaDocument6 pagesTutorial SSWALFA by IDI Surabayaaji100% (1)
- Glaukoma: Dr. Mandiri Nindiasari, SPM, MSCDocument59 pagesGlaukoma: Dr. Mandiri Nindiasari, SPM, MSCfebienaNo ratings yet
- Aao Bab 4Document3 pagesAao Bab 4ria mutiaraNo ratings yet
- EmpyemaDocument17 pagesEmpyemadeo_gratias14No ratings yet
- Direct and Indirect FinalDocument31 pagesDirect and Indirect Finalmeenali karnNo ratings yet
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruNo ratings yet
- KeratitisDocument8 pagesKeratitismohamadNo ratings yet
- Trauma MataDocument57 pagesTrauma MataFatmala Umi MaisarahNo ratings yet
- Workshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIDocument57 pagesWorkshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIMichael FlynnNo ratings yet
- Interpretasi Thorax FotoDocument38 pagesInterpretasi Thorax FotoMonika JonesNo ratings yet
- Parese Nervus III (Oculomotorius)Document26 pagesParese Nervus III (Oculomotorius)jantyNo ratings yet
- Retinal DetachmentDocument8 pagesRetinal DetachmentJohanLazuardiNo ratings yet
- Instrumen SICS (Small Incision Cataract Surgery)Document2 pagesInstrumen SICS (Small Incision Cataract Surgery)roifdyahNo ratings yet
- BHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga TotalDocument7 pagesBHP Phaco Umum Dan Langganan BHP Dengan Lensa Premium KALBE 2,100,000 NO BHP Satuan Pemakaian Harga Totalr.mardhiyah delimaNo ratings yet
- Pms Mayor TerbaruDocument43 pagesPms Mayor TerbaruKeyko LampitaNo ratings yet
- Journal Reading - Avizena Muhammad Zamzam - CPPDS Mata UnsriDocument27 pagesJournal Reading - Avizena Muhammad Zamzam - CPPDS Mata UnsriwidyawirapNo ratings yet
- Contoh Soal Residen CardioDocument13 pagesContoh Soal Residen CardioLusyAlwiNo ratings yet
- Database Member CIMSA UNISSULA Update 2 Agustus 2014Document51 pagesDatabase Member CIMSA UNISSULA Update 2 Agustus 2014persijapqNo ratings yet
- Operasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarDocument10 pagesOperasi Monokular Recess Resect Dengan Teknik: Hangback Pada Exotropia Deviasi BesarBlack Clover IdNo ratings yet
- Cataract 20surgery 2029 05 2008 131224024457 Phpapp01Document61 pagesCataract 20surgery 2029 05 2008 131224024457 Phpapp01Bboy ToonNo ratings yet
- RAPDDocument2 pagesRAPDAlpascaFirdausNo ratings yet
- Referat Gangguan Lapang PandangDocument27 pagesReferat Gangguan Lapang PandangIkrima MuhdarmuhallyNo ratings yet
- Corne A: Dr. Yulia Fitriani, SPMDocument47 pagesCorne A: Dr. Yulia Fitriani, SPMEdsel QasswaraNo ratings yet
- Osteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRDocument28 pagesOsteoartritis: Dr. Dewi Nur Fiana.,Sp - KFRgita cahayaNo ratings yet
- Age-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MDocument28 pagesAge-Related Macular Disease: Fitriani Umi Hasanah 201820401011121 Pembimbing: Dr. Fatin Hamamah, SP.MKim NayoungNo ratings yet
- Spleen: DR - Supriti Demonstrator Anatomy Deptt TMMC&RCDocument35 pagesSpleen: DR - Supriti Demonstrator Anatomy Deptt TMMC&RCBilal Yimam100% (1)
- Diagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthaDocument13 pagesDiagnosis Dan Tatalaksana Pasien Dengan Insufisiensi Akomodasi - Sri Hudaya WidihasthamalaNo ratings yet
- What Is The Difference Between A Pterygium and A Pinguecula?Document2 pagesWhat Is The Difference Between A Pterygium and A Pinguecula?Rizky AgustriaNo ratings yet
- Pemeriksaan GonioskopiDocument26 pagesPemeriksaan GonioskopiMuhammad Mu'amar HabibieNo ratings yet
- EviserasiDocument5 pagesEviserasiristaniatauhidNo ratings yet
- Initial Assessment: - Rambam Medical Center - DR Nordkin DmitriDocument60 pagesInitial Assessment: - Rambam Medical Center - DR Nordkin Dmitridheviant12No ratings yet
- RozerplastyDocument4 pagesRozerplastyLutfi Aulia RahmanNo ratings yet
- Retina Examination and Drawing: CEH Retinal TeamDocument39 pagesRetina Examination and Drawing: CEH Retinal TeamrzmNo ratings yet
- Salter BAB 16Document126 pagesSalter BAB 16Yobbi Arissaputra100% (1)
- Penatalaksanaan Trauma Kimia Alkali Pada Mata - Anisa Feby ArifaniDocument18 pagesPenatalaksanaan Trauma Kimia Alkali Pada Mata - Anisa Feby ArifaniLapas Sustik LampungNo ratings yet
- PterygiumDocument69 pagesPterygiumYedi Hendrawiana100% (1)
- Lapkas Hymen ImperforataDocument27 pagesLapkas Hymen ImperforataKhairida Hafni LbsNo ratings yet
- Laporan Kasus Katarak Fathonah (1102013108) .Id - enDocument48 pagesLaporan Kasus Katarak Fathonah (1102013108) .Id - enAnonymous ZbhBxeEVNo ratings yet
- Girl 2 - 5 Tahun - WHODocument3 pagesGirl 2 - 5 Tahun - WHOPatime Nekomata NibinoNo ratings yet
- GonioskopiDocument40 pagesGonioskopiRaissaNo ratings yet
- Unlock-Forensik Etik Medikolegal - PESERTADocument156 pagesUnlock-Forensik Etik Medikolegal - PESERTAAde fathNo ratings yet
- Lapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Document14 pagesLapkas Glaukoma Pemasangan Implan GDD Lapkas Glaukoma (AutoRecovered)Vincent RoorohNo ratings yet
- Z Score Boys PDFDocument15 pagesZ Score Boys PDFMuhammad Aldiansyah Januario0% (1)
- Basic VitrectomyDocument24 pagesBasic Vitrectomykomitemedik.rsudsdaNo ratings yet
- Basic Manual Small Incision Cataract Surgery: Dr. Cok I Dewiyani, SP.MDocument65 pagesBasic Manual Small Incision Cataract Surgery: Dr. Cok I Dewiyani, SP.MCok Krishna D. PemayunNo ratings yet
- Eye ProblemsDocument25 pagesEye ProblemsHikmat UllahNo ratings yet
- Surgery of The EyeDocument3 pagesSurgery of The Eyehonovezaann.a.campita.ctucvmNo ratings yet
- BandagesDocument34 pagesBandagesAnusha VergheseNo ratings yet
- Surgical Procedure For Dehorning and Penile AmputationDocument17 pagesSurgical Procedure For Dehorning and Penile AmputationHikmat UllahNo ratings yet
- Hysterectomy SetDocument2 pagesHysterectomy SetD'Mhan MbozoNo ratings yet
- Brosur Product MEDIST - MEVACS M90.CompressedDocument1 pageBrosur Product MEDIST - MEVACS M90.CompressedD'Mhan MbozoNo ratings yet
- Major Orthopaedic SetDocument2 pagesMajor Orthopaedic SetD'Mhan Mbozo0% (1)
- Hordeolum Instrument SetDocument1 pageHordeolum Instrument SetD'Mhan MbozoNo ratings yet
- Living Sexy With Allana Pratt (Episode 29) Wired For Success TVDocument24 pagesLiving Sexy With Allana Pratt (Episode 29) Wired For Success TVwiredforsuccesstvNo ratings yet
- (Metasol MS) Catalog en 202105Document192 pages(Metasol MS) Catalog en 202105LS ELECTRIC INDIANo ratings yet
- Counter Fort Retaining WallDocument3 pagesCounter Fort Retaining WalljosefNo ratings yet
- History of Civil EngineerDocument3 pagesHistory of Civil EngineerErnest 1TNo ratings yet
- (L+4) +chapter+02+ Biological+Classification++NEET+Questions+Menti+++ +DPP+Document48 pages(L+4) +chapter+02+ Biological+Classification++NEET+Questions+Menti+++ +DPP+AMISHA RATHISHNo ratings yet
- Honeywell DPR 2300 and 3000Document338 pagesHoneywell DPR 2300 and 3000kmpoulosNo ratings yet
- Seed MoneyDocument8 pagesSeed MoneySirIsaacs Gh100% (1)
- Anger ManagementDocument18 pagesAnger Managementparag narkhedeNo ratings yet
- Mabcredit BrochureDocument15 pagesMabcredit BrochurealfredogoncalvesjrNo ratings yet
- Genphysics q2 Mod5Document28 pagesGenphysics q2 Mod5Mhasie Joy PondevidaNo ratings yet
- LetoffsystemsDocument109 pagesLetoffsystemsabiyNo ratings yet
- Oh! To Be Like Thee: WORDS: Thomas O. Chisholm, Pub.1897. MUSIC: William J. Kirkpatrick, 1897. Public DomainDocument1 pageOh! To Be Like Thee: WORDS: Thomas O. Chisholm, Pub.1897. MUSIC: William J. Kirkpatrick, 1897. Public DomainAlonge EmmanuelNo ratings yet
- Lecture 3Document28 pagesLecture 3Lovely ZahraNo ratings yet
- Practical 06:-Write A Program in C To Translate 2D and 3D ObjectDocument5 pagesPractical 06:-Write A Program in C To Translate 2D and 3D ObjectKhan.aliNo ratings yet
- PHD ThesisDocument232 pagesPHD Thesiskafle_yrs100% (1)
- Motion in Electric Fields: SACE Stage 2 PhysicsDocument43 pagesMotion in Electric Fields: SACE Stage 2 Physicsrampravesh kumarNo ratings yet
- Dakshinavarti ShankhDocument7 pagesDakshinavarti Shankhb_subhashis100% (1)
- Optimal Solution Using MODI - MailDocument17 pagesOptimal Solution Using MODI - MailIshita RaiNo ratings yet
- Introduction To Culinary ArtsDocument10 pagesIntroduction To Culinary ArtsNico Urieta De AdeNo ratings yet
- Buriki PresentationDocument12 pagesBuriki PresentationPutraNo ratings yet
- Lesson 3 English For Specific PurposesDocument14 pagesLesson 3 English For Specific PurposesJudith CastilloNo ratings yet
- Star Wars - Han Solo Adventures Book 2 - Han Solo's RevengeDocument84 pagesStar Wars - Han Solo Adventures Book 2 - Han Solo's Revengeshahali76100% (2)
- Role of Physiotherapy in ICUDocument68 pagesRole of Physiotherapy in ICUprasanna3k100% (2)
- BoqDocument30 pagesBoqPrashant Singh Chauhan100% (1)
- Booking Details Fares and Payment: E-Ticket and Tax Invoice - ExpressDocument2 pagesBooking Details Fares and Payment: E-Ticket and Tax Invoice - ExpressWidodo MuisNo ratings yet
- 4.5m Commercial Antenna King Post MountDocument16 pages4.5m Commercial Antenna King Post MountsahanNo ratings yet
- Prinsipal Kode Produk Nama ProdukDocument40 pagesPrinsipal Kode Produk Nama ProdukjihanvrpNo ratings yet