Download as pptx, pdf, or txt
You might also like
- Heart & Neck Vessel AssessmentDocument46 pagesHeart & Neck Vessel AssessmentLouise Nathalia VelasquezNo ratings yet
- Wilcox's Surgical Anatomy of The Heart 4th EdDocument391 pagesWilcox's Surgical Anatomy of The Heart 4th EdGeorgiana Golea100% (1)
- Transient Ischemic Attack and HomeopathyDocument32 pagesTransient Ischemic Attack and HomeopathyDr. Rajneesh Kumar Sharma MD HomNo ratings yet
- PigDocument34 pagesPigaa62893% (14)
- AntiHypertensives (Autosaved)Document64 pagesAntiHypertensives (Autosaved)UsamaNo ratings yet
- Lecture 24-25 - Antihypertensive AgentsDocument30 pagesLecture 24-25 - Antihypertensive AgentsJedoNo ratings yet
- Terapi Farmakologi Gagal Jantung - Sept - 2020Document58 pagesTerapi Farmakologi Gagal Jantung - Sept - 2020FAUZAN ILHAM PRATAMANo ratings yet
- Antihypertensive Drugs RTDocument41 pagesAntihypertensive Drugs RTMaherNo ratings yet
- Antihypertensives: Dr. Lucy ClunesDocument45 pagesAntihypertensives: Dr. Lucy ClunesZaqueo Gutierrez FajardoNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Hypertension Lecture3: Pharmacological TreatmentDocument25 pagesHypertension Lecture3: Pharmacological TreatmentRam NiwasNo ratings yet
- Antihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Document44 pagesAntihypertensive Drugs: S. Parasuraman, M.Pharm., PH.D.Shreya SinhaNo ratings yet
- Chaper 20 Study CardsDocument8 pagesChaper 20 Study Cardsheldai1No ratings yet
- Drugs Used in The Management of Heart Failure: DR Sindwa KanyimbaDocument29 pagesDrugs Used in The Management of Heart Failure: DR Sindwa Kanyimbaedward kaumbaNo ratings yet
- ReveweDocument119 pagesRevewehikmatullah rahimiNo ratings yet
- Drugs For CHF & Angina PDFDocument15 pagesDrugs For CHF & Angina PDFAbdullah ElsayedNo ratings yet
- Penatalaksanaan Penyulit Gagal JantungDocument17 pagesPenatalaksanaan Penyulit Gagal JantungarumNo ratings yet
- HTN Treatment DR - VishvasDocument46 pagesHTN Treatment DR - VishvasvishvasNo ratings yet
- HTN JmiDocument39 pagesHTN Jmink999999No ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- AntihipertensiDocument39 pagesAntihipertensiHarri HardiNo ratings yet
- Approach To Patient With HypertensionDocument64 pagesApproach To Patient With HypertensionAndrassy Twinkle AlineaNo ratings yet
- Inotropic Agents - Blockers Renin InhibitorsDocument19 pagesInotropic Agents - Blockers Renin InhibitorslitaNo ratings yet
- Inotropic Agents - Blockers Renin InhibitorsDocument19 pagesInotropic Agents - Blockers Renin InhibitorsTanyir MarieClaireNo ratings yet
- Curs Studenti Clase Terapeutice - 2015Document84 pagesCurs Studenti Clase Terapeutice - 2015Teodor NeaguNo ratings yet
- Aliskiren and Enalapril in Heart FailureDocument43 pagesAliskiren and Enalapril in Heart FailureKishor K AdhikariNo ratings yet
- Lecture 6 Anti HypertensionDocument40 pagesLecture 6 Anti HypertensionMNGS StudioNo ratings yet
- CHF 2Document14 pagesCHF 2Nitesh TiwariNo ratings yet
- Cvs DrugsDocument106 pagesCvs DrugsIkoona ivanNo ratings yet
- Lecture 1 antihypertensionSDSDocument7 pagesLecture 1 antihypertensionSDSSara AbbasNo ratings yet
- Heart Failure DrugsDocument35 pagesHeart Failure Drugszmr27146No ratings yet
- Angiotensin I Angiotensin II, Angiotensin-Converting Enzyme (ACE) - Vasoconstrictor Angiotensin II Stimulates Aldosterone SecretionDocument11 pagesAngiotensin I Angiotensin II, Angiotensin-Converting Enzyme (ACE) - Vasoconstrictor Angiotensin II Stimulates Aldosterone SecretionAbdullah asadNo ratings yet
- Heart Failure and DHF PDFDocument31 pagesHeart Failure and DHF PDFMahamed Wefkey OmranNo ratings yet
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- 6 CVS Lecture 5 - Drugs For Heart FailureDocument55 pages6 CVS Lecture 5 - Drugs For Heart FailureCraig DuHaneyNo ratings yet
- Antihypertensive Drugs ٠١١٦٥٨Document10 pagesAntihypertensive Drugs ٠١١٦٥٨mohnad806mNo ratings yet
- Hypertension PDFDocument57 pagesHypertension PDFrahul m dNo ratings yet
- Antihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarDocument52 pagesAntihypertensive Drugs: DR Chaitali Pattanayak Professor, Pharmacology Kims, BhubaneswarASHUTOSH KHADANGANo ratings yet
- Chapter 13 Drugs Used in Heart FailureDocument7 pagesChapter 13 Drugs Used in Heart FailureChristine Annmarie TapawanNo ratings yet
- Congestive Cardiac Failure 2021Document31 pagesCongestive Cardiac Failure 2021SaniNo ratings yet
- Antihypertensive Drugs.Document35 pagesAntihypertensive Drugs.Abdul WahabNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Anti HypretensivesDocument18 pagesAnti HypretensivesLeena AlateeqNo ratings yet
- Pharmacotherapy of HypertensionDocument52 pagesPharmacotherapy of HypertensionDrVinod Kumar Goud VemulaNo ratings yet
- Antihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityDocument71 pagesAntihypertensive Drugs: Dr/Azza Baraka Prof of Clinical Pharmacology Faculty of Medicine Alexandria UniversityMoonAIRNo ratings yet
- Terapi Hipertensi (Hipertensi Ve Disease) : Dr. Fitri SeptianingsihDocument23 pagesTerapi Hipertensi (Hipertensi Ve Disease) : Dr. Fitri SeptianingsihMaulana HasanNo ratings yet
- Curs Studenti Clase Terapeutice - 2015Document88 pagesCurs Studenti Clase Terapeutice - 2015Elie FlorrNo ratings yet
- Pharmacology of Anti Hypertensive Agents (For BPT Students)Document17 pagesPharmacology of Anti Hypertensive Agents (For BPT Students)Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- CHF 5Document2 pagesCHF 5Agus HaryantoNo ratings yet
- Chapter 11 Antihypertensive AgentsDocument11 pagesChapter 11 Antihypertensive AgentsChristine Annmarie TapawanNo ratings yet
- Asuhan Keperawatan, Pencegahan Covid-19Document68 pagesAsuhan Keperawatan, Pencegahan Covid-19Mei Catur riyantoNo ratings yet
- HypertensionDocument43 pagesHypertensionAbin PNo ratings yet
- Anoosha Roll#21Document19 pagesAnoosha Roll#21Anusha ZubairNo ratings yet
- Cardiac DrugsDocument35 pagesCardiac DrugsCristina Centurion100% (3)
- Antihypertensive Drugs: DR. DR Umi Kalssum MkesDocument58 pagesAntihypertensive Drugs: DR. DR Umi Kalssum MkesadilaalifnugrahaeniNo ratings yet
- Cardio DrugsDocument68 pagesCardio DrugsIconMaicoNo ratings yet
- Anti HypertensionDocument62 pagesAnti HypertensionHazazi Jr Love LoverpoolNo ratings yet
- Antianginal DrugsDocument19 pagesAntianginal DrugsAnusha ZubairNo ratings yet
- Bihs PDFDocument4 pagesBihs PDFFredrikus Lay Berkh MansNo ratings yet
- Pharmacologic Agents in Heart Failure: Ayman Khdair, Ph.D. Wayne State University, Michigan, USADocument41 pagesPharmacologic Agents in Heart Failure: Ayman Khdair, Ph.D. Wayne State University, Michigan, USAJalil HaddadinNo ratings yet
- Management of Heart Failure: OutlineDocument27 pagesManagement of Heart Failure: OutlineBoetik AlifiaNo ratings yet
- HypertensionDocument46 pagesHypertensionElsai EsbNo ratings yet
- Pharmacologyofccf 181227034555Document43 pagesPharmacologyofccf 181227034555MohammedMujahedNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Renal Vascular DiseasesDocument56 pagesRenal Vascular Diseasesjohny3333No ratings yet
- Science 9: Quarter 1 Circulatory SystemDocument23 pagesScience 9: Quarter 1 Circulatory Systemjelly marie floresNo ratings yet
- RPT CardioDocument2 pagesRPT CardioBrad PamnaniNo ratings yet
- Lecture 01 - CVSDocument45 pagesLecture 01 - CVSHeeb WardaNo ratings yet
- MCQ Int - MedDocument166 pagesMCQ Int - MedOmar Ahmed100% (1)
- Posterior and Anterior MediastinumDocument6 pagesPosterior and Anterior MediastinumYheng GaosaiiNo ratings yet
- 3 Nursing Care PlanDocument6 pages3 Nursing Care PlanJeyser T. GamutiaNo ratings yet
- Chirurgica.: Daftar PustakaDocument2 pagesChirurgica.: Daftar PustakaNindiaRahmaPutriNo ratings yet
- TERM 2 Chapter 8 Topical RevisionDocument74 pagesTERM 2 Chapter 8 Topical RevisionElil MathhyNo ratings yet
- Circulatory Pt. 1Document10 pagesCirculatory Pt. 1Melvin Razon Espinola Jr.No ratings yet
- Edema and FarctionDocument45 pagesEdema and FarctionGokulapriya.KNo ratings yet
- Pulse Waves 2017Document231 pagesPulse Waves 2017ConstantineSemenchukNo ratings yet
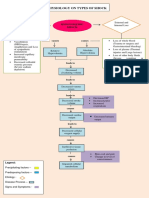
- Pathophysiology On Types of ShockDocument4 pagesPathophysiology On Types of ShockJessa Mae Alforque AsentistaNo ratings yet
- (James T. Willerson MD, Jay N. Cohn MD, James T. WDocument2,877 pages(James T. Willerson MD, Jay N. Cohn MD, James T. WHoàng LongNo ratings yet
- Monro Kellie Doctrine/ PrincipleDocument5 pagesMonro Kellie Doctrine/ PrincipleAngelu Gabrielle CastroNo ratings yet
- Pulmonic Valve DiseaseDocument22 pagesPulmonic Valve Diseasesarguss14No ratings yet
- Essay-The Need To Look Beyond Traditional Risk Factors in Medical Diagnoses Diviyashree KasiviswanathanDocument12 pagesEssay-The Need To Look Beyond Traditional Risk Factors in Medical Diagnoses Diviyashree Kasiviswanathanapi-672608340No ratings yet
- Vascular Abnormalities of SSCDocument9 pagesVascular Abnormalities of SSCCristina ElenaNo ratings yet
- Ouriel K., Rutherford R.В. - Atlas of Vascular Surgery - Basic Techniques and Exposures - ocrDocument270 pagesOuriel K., Rutherford R.В. - Atlas of Vascular Surgery - Basic Techniques and Exposures - ocr.No ratings yet
- Cardio and Hema - DR PueyoDocument161 pagesCardio and Hema - DR Pueyoapi-3735995100% (2)
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 38Document12 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 38sarasjunkNo ratings yet
- 4 5780579467025976939Document843 pages4 5780579467025976939osama hosniNo ratings yet
- Health Assessment - Cardiovascular and Peripheral Vascular SystemsDocument5 pagesHealth Assessment - Cardiovascular and Peripheral Vascular SystemsPenelope E. Davidson100% (1)
- Anatomy Myocardial InfarctionDocument5 pagesAnatomy Myocardial InfarctionLyka Milo AvilaNo ratings yet
- Nihms 1873457Document15 pagesNihms 1873457Hanssel Viramontes CastroNo ratings yet
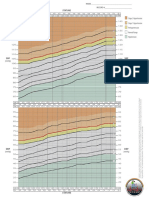
- BP Chart Girls Color WideDocument1 pageBP Chart Girls Color WidealbertNo ratings yet