Download as pptx, pdf, or txt
You might also like
- Pericardial EffusionDocument35 pagesPericardial EffusionRizky Amalia WakanoNo ratings yet
- Case PresDocument44 pagesCase PresPhilia FeliceNo ratings yet
- ShockDocument68 pagesShockseries recapNo ratings yet
- Shock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalDocument47 pagesShock: Erdiansyah Zulyadaini, MD, FIHA FK Universitas Muhammadiyah Purwokerto/ RSUD Dr. Soeselo Kabupaten TegalFarah AkhwanisNo ratings yet
- Shock & Iv Fluids: Dr. Ahmed Khan Sangrasi Associate Professor, Department of Surgery, LUMHS JamshoroDocument120 pagesShock & Iv Fluids: Dr. Ahmed Khan Sangrasi Associate Professor, Department of Surgery, LUMHS JamshoroTheruna100% (1)
- Management of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaDocument77 pagesManagement of Shock in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sceinces Kochi, KeralaAETCM Emergency medicineNo ratings yet
- Pedia SGD NICUDocument62 pagesPedia SGD NICUJAIRISH YZABELLE SALVADORNo ratings yet
- Curs 3 ShockDocument78 pagesCurs 3 ShockIoana CNo ratings yet
- Case Report: Congestive Heart Failure FC III + Nonvalvular Atrial Fibrillation-Normo Ventricular ResponDocument21 pagesCase Report: Congestive Heart Failure FC III + Nonvalvular Atrial Fibrillation-Normo Ventricular ResponKarolus KetarenNo ratings yet
- Shock: Curs Studenti An ViDocument78 pagesShock: Curs Studenti An ViAnonymous dKiLqVS3L5No ratings yet
- Pericardial DiseaseDocument70 pagesPericardial DiseaseCindyNo ratings yet
- IE 01 JuneDocument82 pagesIE 01 Junediopters16200No ratings yet
- Life Threatening Hilar ShadowsDocument24 pagesLife Threatening Hilar ShadowsEBNo ratings yet
- L15-Shock & Resuscitation LectureDocument49 pagesL15-Shock & Resuscitation LectureYosra —No ratings yet
- 5 Shock PPT EnglishDocument77 pages5 Shock PPT EnglishKessi VikaneswariNo ratings yet
- PresusDocument30 pagesPresusBrian Mahendra BesmayaNo ratings yet
- Acute Limb Ischemic: Case ReportDocument24 pagesAcute Limb Ischemic: Case Reportdewigenda yusufNo ratings yet
- Shock: Disampaikan Oleh: Dr. I G A G Utara Hartawan, Span MarsDocument88 pagesShock: Disampaikan Oleh: Dr. I G A G Utara Hartawan, Span MarsNym Angga SantosaNo ratings yet
- Complicated UTI - Mario's HourDocument21 pagesComplicated UTI - Mario's HourNikki Tuazon BartolomeNo ratings yet
- Systemic Lupus Erithematosus & Marfan's SyndromeDocument74 pagesSystemic Lupus Erithematosus & Marfan's SyndromeFitriYani SimangunsoNgNo ratings yet
- Iii PBL 11-10-18Document19 pagesIii PBL 11-10-18Ahmad SobihNo ratings yet
- Cerebrovascular Disease (Autosaved)Document83 pagesCerebrovascular Disease (Autosaved)Henry BonaNo ratings yet
- Morning Report: Dept. of Internal MedicineDocument24 pagesMorning Report: Dept. of Internal MedicineAnonymous VEUa5p1INo ratings yet
- Acute Rheumatic FeverDocument37 pagesAcute Rheumatic FeverQadriyah Ramadhani100% (1)
- PPTDocument28 pagesPPTuculucullNo ratings yet
- Mitral RegurgitationDocument43 pagesMitral Regurgitationraissasafitry100% (1)
- Congestive Heart Failure (CHF) NYHA III E.C Coronary Artery Disease (OMI Anteroseptal)Document35 pagesCongestive Heart Failure (CHF) NYHA III E.C Coronary Artery Disease (OMI Anteroseptal)GP HMHNo ratings yet
- Acute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidentDocument48 pagesAcute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidenterikaNo ratings yet
- StrokeDocument74 pagesStrokeDonnaBells Hermo Labaniego100% (2)
- Hypertensive EmergenciesDocument49 pagesHypertensive EmergenciesSafa Abdualrahaman Ali HamadNo ratings yet
- Ventricel Septal DefectDocument38 pagesVentricel Septal DefectzaipullahNo ratings yet
- Dengue Fever: Nur Emira Mohammad Agus Nurul Zafirah Mohammad RamliDocument24 pagesDengue Fever: Nur Emira Mohammad Agus Nurul Zafirah Mohammad Ramlinurul akmar mohamad ramliNo ratings yet
- Cardiac Dysrhythmia in The ImmunocompromisedDocument53 pagesCardiac Dysrhythmia in The ImmunocompromisedGoogle_ajaNo ratings yet
- All That Glitters Is Not GoldDocument30 pagesAll That Glitters Is Not GoldKishan KoyaniNo ratings yet
- 2nd Activity - Patient With Cough and FeverDocument40 pages2nd Activity - Patient With Cough and FeverJethro Floyd QuintoNo ratings yet
- Good Morning Report!: Nora Switchenko MD R3Document15 pagesGood Morning Report!: Nora Switchenko MD R3Emily EresumaNo ratings yet
- Dr. Mulenga E M1Document34 pagesDr. Mulenga E M1ericNo ratings yet
- ContohmrresidenDocument53 pagesContohmrresidenFlorensia S. LarumpaaNo ratings yet
- Monitoring PerioperatipDocument54 pagesMonitoring Perioperatipjavajavu100% (1)
- Shock in Children TutorialDocument37 pagesShock in Children TutorialSsenyonga DominicNo ratings yet
- Case ReportDocument27 pagesCase ReportnurulNo ratings yet
- Approach To The Patient With Suspected Vasculitis: Supervised By: Dr. Nabil Al - Jahawi Persented By: Dr. Enas FutaisiDocument21 pagesApproach To The Patient With Suspected Vasculitis: Supervised By: Dr. Nabil Al - Jahawi Persented By: Dr. Enas FutaisiRasha mohammad100% (1)
- CHF FC III Ec Mitral StenosisDocument36 pagesCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- Cardiovascular & Hematologic SystemDocument163 pagesCardiovascular & Hematologic SystemRellie CastroNo ratings yet
- Ward Round Report10 Nov AVMDocument21 pagesWard Round Report10 Nov AVMlie antoNo ratings yet
- How To Approach Dyspnea in ED - Pramono SigitDocument29 pagesHow To Approach Dyspnea in ED - Pramono SigitLeonita DwiNo ratings yet
- Shock: DR Terence See Consultant Emergency Department, TTSHDocument72 pagesShock: DR Terence See Consultant Emergency Department, TTSHHendri Tamara YudaNo ratings yet
- IANs Presentation - Atrial Fibrillation (RMO Kerenga)Document26 pagesIANs Presentation - Atrial Fibrillation (RMO Kerenga)Samuel.MoriNo ratings yet
- Case Management: Leira Dith R. Castro, MD Presentor 1 Year Im ResidentDocument64 pagesCase Management: Leira Dith R. Castro, MD Presentor 1 Year Im ResidentAlvin Germo PasuquinNo ratings yet
- Cardiomyopathy: Kevin Anthony Mentor: Dr. Juliana Batubara, M.Ked (Ped), Sp.ADocument42 pagesCardiomyopathy: Kevin Anthony Mentor: Dr. Juliana Batubara, M.Ked (Ped), Sp.AiestiNo ratings yet
- Stroke 1Document35 pagesStroke 1Aisyah IcahNo ratings yet
- ShockDocument24 pagesShockYaacub IbrahimNo ratings yet
- Acute LeukemiaDocument29 pagesAcute LeukemiaArsalan SaeedNo ratings yet
- A Rare Cause of Reversible Cardiomyopathy PKPDocument27 pagesA Rare Cause of Reversible Cardiomyopathy PKPlichumo murryNo ratings yet
- Hypertensive Encephalopathy: By:hasmawaty BasirDocument78 pagesHypertensive Encephalopathy: By:hasmawaty BasirLexyArungTikuNo ratings yet
- VERTIGO (Compatibility Mode)Document28 pagesVERTIGO (Compatibility Mode)Franciscus BuwanaNo ratings yet
- PSBIM ReviewerDocument37 pagesPSBIM ReviewerAlsalman AnamNo ratings yet
- Scrub With CerebellitisDocument10 pagesScrub With CerebellitisdivyasatthishNo ratings yet
- Fever With HemiplegiaDocument65 pagesFever With HemiplegiaMohit JainNo ratings yet
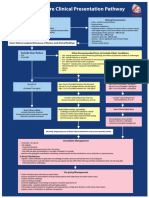
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- Secrets of PacesDocument162 pagesSecrets of PacesMohammadAbdurRahman0% (1)
- Pocket Biology (Chap-1 To 9)Document4 pagesPocket Biology (Chap-1 To 9)Fatima Habib MuzaffarNo ratings yet
- Critical Limb IschemicDocument27 pagesCritical Limb IschemicErik Judika2No ratings yet
- The Pelvis IiDocument25 pagesThe Pelvis IiFaith ChepoghishoNo ratings yet
- Journal Pre-Proof: Journal of The American Academy of DermatologyDocument56 pagesJournal Pre-Proof: Journal of The American Academy of DermatologyMădălina StamateNo ratings yet
- B-Blockers in Patients With Sepsis. Putting The Puzzle Together, Piece by PieceDocument2 pagesB-Blockers in Patients With Sepsis. Putting The Puzzle Together, Piece by Pieceluis sanchezNo ratings yet
- Diaz Flores 32 1239 1279 2017Document41 pagesDiaz Flores 32 1239 1279 2017María P SNo ratings yet
- Update On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorDocument21 pagesUpdate On The Clinical Pharmacology of Etoricoxib A Potent Cyclooxygenase2 InhibitorAnh Quoc LeNo ratings yet
- Mechanical Thrombectomy For Acute Ischemic StrokeDocument19 pagesMechanical Thrombectomy For Acute Ischemic StrokeCarlos Alfredo Vargas QuinteroNo ratings yet
- OSCE Skills 2013 1Document141 pagesOSCE Skills 2013 1Haseeb RayhanNo ratings yet
- NCM 109 Module 9Document18 pagesNCM 109 Module 9capoyljtNo ratings yet
- Mbbs Final Part IIDocument64 pagesMbbs Final Part IIVikas TekamNo ratings yet
- Diagnostics 10 00912Document12 pagesDiagnostics 10 00912amyNo ratings yet
- EMREE examGuideApplicantGuide2021 240511 205655Document48 pagesEMREE examGuideApplicantGuide2021 240511 205655AjayNo ratings yet
- Cardiovascular Lecture 2 - 2023 2024Document11 pagesCardiovascular Lecture 2 - 2023 2024inegbenosegideonNo ratings yet
- C1 Lab 3Document32 pagesC1 Lab 3anaNo ratings yet
- OSCE Marksheet 1Document7 pagesOSCE Marksheet 1Elias PetrouNo ratings yet
- Toate Bolile CardiovasculareDocument6 pagesToate Bolile CardiovasculareAnca CopreanNo ratings yet
- MAPCA'sDocument1 pageMAPCA'sFania Dora AslamyNo ratings yet
- AD8232 ECG MonitoringDocument7 pagesAD8232 ECG Monitoringsupport ubicuoNo ratings yet
- p173 PDFDocument8 pagesp173 PDFKarinaWijayantiNo ratings yet
- Introduction To Critical Care NursingDocument10 pagesIntroduction To Critical Care NursingAngielyn Ramos Oloraza100% (2)
- Low Yield Fact SheetDocument2 pagesLow Yield Fact SheetNara GhassaniNo ratings yet
- Asuhan Keperawatan HipertensiDocument30 pagesAsuhan Keperawatan HipertensiNur Ainun Afifa JumratunnisaNo ratings yet
- Tiki Taka CK CardiologyDocument46 pagesTiki Taka CK CardiologyChristian Jara100% (2)
- Thromboelastography: Clinical Application, Interpretation, and Transfusion ManagementDocument7 pagesThromboelastography: Clinical Application, Interpretation, and Transfusion ManagementMarcelliaNo ratings yet
- HyponatremiaDocument20 pagesHyponatremiamanjaruNo ratings yet
- Approach To Cyanosis in A NeonateDocument12 pagesApproach To Cyanosis in A NeonateXerxyllXyreaneLinaoNo ratings yet
- Medical Technology ReviewerDocument57 pagesMedical Technology ReviewerOng Christopher100% (2)