Download as pptx, pdf, or txt
You might also like
- ALK-positive Lung Cancer: A Moving TargetDocument16 pagesALK-positive Lung Cancer: A Moving TargetcerbulcarpatinNo ratings yet
- Patologi Anatomi: Blok 3.6 Slide TentiranDocument119 pagesPatologi Anatomi: Blok 3.6 Slide TentirankikiNo ratings yet
- Granulomatus Diseases of The Nose For 4th YearDocument68 pagesGranulomatus Diseases of The Nose For 4th YearEmaan NoorNo ratings yet
- GIT, AlemDocument224 pagesGIT, Alemmex GbrekorkosNo ratings yet
- Chapter 16 - Head and NeckDocument8 pagesChapter 16 - Head and NeckAgnieszka WisniewskaNo ratings yet
- Pathology Book For RRSDocument96 pagesPathology Book For RRSmina mounirNo ratings yet
- Respiratory PathologyDocument3 pagesRespiratory PathologyDawan SherkoNo ratings yet
- ENT Pathology: Assistan Professor Dr. Sazan Abdulwahab MirzaDocument66 pagesENT Pathology: Assistan Professor Dr. Sazan Abdulwahab MirzaMariam QaisNo ratings yet
- Viral Diseases Newcastle Disease (ND)Document47 pagesViral Diseases Newcastle Disease (ND)thanh ba matNo ratings yet
- Nasal TumorDocument20 pagesNasal TumorMahmoud ElsherbenyNo ratings yet
- Sino NasalDocument13 pagesSino NasalClaudia EpureNo ratings yet
- Pulmonary PathologyDocument134 pagesPulmonary PathologyFor ChristNo ratings yet
- Oral PathologyDocument18 pagesOral Pathologyمنتظر منشد دعاشNo ratings yet
- Neoplasms of Nose & para Nasal SinusesDocument171 pagesNeoplasms of Nose & para Nasal SinusesJulian HobbsNo ratings yet
- Benign Diseases of The Vulvavagina andDocument58 pagesBenign Diseases of The Vulvavagina andHervis FantiniNo ratings yet
- 10 - Patholog Salivar GL - PART 2Document44 pages10 - Patholog Salivar GL - PART 2Andreea RedheadNo ratings yet
- Granulo 3Document94 pagesGranulo 3Sathvika BNo ratings yet
- Salivary Gland TumoursDocument131 pagesSalivary Gland TumoursSushmithaNo ratings yet
- Non-Neoplastic Disorders: Lymphoid SystemDocument36 pagesNon-Neoplastic Disorders: Lymphoid SystemMutiana Muspita JeliNo ratings yet
- Pathophysio HPVs Fall Into Different Subgroups With A Predilection For Arising From Either Mucosal Surfaces or The SkinDocument2 pagesPathophysio HPVs Fall Into Different Subgroups With A Predilection For Arising From Either Mucosal Surfaces or The SkinOstazNo ratings yet
- Sexually Transmitted DiseasesDocument174 pagesSexually Transmitted Diseasesfroizki100% (1)
- Conjunctiva Anatomy and PhysiologyDocument101 pagesConjunctiva Anatomy and PhysiologyPurva KeswaniNo ratings yet
- MCQS CNS PathologyDocument14 pagesMCQS CNS PathologyFourth YearNo ratings yet
- Shagubs EntDocument25 pagesShagubs EntFelicianna Ashwinie StanleyNo ratings yet
- CPC 1 Jan 12 2008 DR RuengerDocument92 pagesCPC 1 Jan 12 2008 DR Ruengerkhawar93No ratings yet
- Neck TumorsDocument7 pagesNeck TumorsJose SirittNo ratings yet
- Benign and Malignant Neoplasia of URTDocument48 pagesBenign and Malignant Neoplasia of URTsahirbuleNo ratings yet
- Salivary Gland PathologyDocument2 pagesSalivary Gland PathologyJayNo ratings yet
- Malignant Epithelial Non-Odontogenic Tumors 2Document11 pagesMalignant Epithelial Non-Odontogenic Tumors 2samamustafa.2003No ratings yet
- Pathology & Pathophysiology of The Gastrointestinal TractDocument67 pagesPathology & Pathophysiology of The Gastrointestinal TractSalmanAlfarisiNo ratings yet
- DERMADocument141 pagesDERMAKenneth NuñezNo ratings yet
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini67% (6)
- Dermatology RevisionDocument6 pagesDermatology RevisionLedia EssamNo ratings yet
- Lec. 13 &14 Epithelial DisordersDocument10 pagesLec. 13 &14 Epithelial DisordersZainab Alshamary0% (1)
- Salivary Glands: Dr. Tanuj Paul BhatiaDocument83 pagesSalivary Glands: Dr. Tanuj Paul BhatiaNgnNo ratings yet
- ASOMDocument41 pagesASOMArunkumar S KumarNo ratings yet
- I.T.S Dental College, Greater Noida: Subject: Oral Pathology Lecture: Bacterial Infections:T BDocument30 pagesI.T.S Dental College, Greater Noida: Subject: Oral Pathology Lecture: Bacterial Infections:T BAMIT GUPTANo ratings yet
- Allergic and Immunologic DiseaseDocument50 pagesAllergic and Immunologic DiseaseRajkumari Sriraman100% (1)
- Precancerous Conditions of Oral CavityDocument80 pagesPrecancerous Conditions of Oral Cavitylarisabrinza12No ratings yet
- Larynx Path 2002 01 SlidesDocument140 pagesLarynx Path 2002 01 SlidesZammira MutiaNo ratings yet
- Epidermophyton (Skin, Nails) : Microsporum, TrichophytonDocument5 pagesEpidermophyton (Skin, Nails) : Microsporum, TrichophytonRoyNo ratings yet
- Nada's GI Path ReviewDocument44 pagesNada's GI Path ReviewNada Much100% (2)
- Benign and Malignant Tumors of Oral CavityDocument56 pagesBenign and Malignant Tumors of Oral CavityPawan Kumar83% (6)
- Bacterial Infections of The Oral CavityDocument212 pagesBacterial Infections of The Oral CavitydrrakbdsNo ratings yet
- SBRC DermatologyDocument83 pagesSBRC DermatologyErin HillNo ratings yet
- Neck Swellings (Compatibility Mode)Document49 pagesNeck Swellings (Compatibility Mode)vihang146No ratings yet
- BenignDocument63 pagesBenignAFREEN SADAFNo ratings yet
- Mycotic Diseases Histoplasmosis (Final)Document33 pagesMycotic Diseases Histoplasmosis (Final)hhes8116No ratings yet
- Lymphadenopathy: A. Suryaveda Aakanksha Sangwaan Aishwarya Alankar ParasharDocument21 pagesLymphadenopathy: A. Suryaveda Aakanksha Sangwaan Aishwarya Alankar ParasharfjajflkajfNo ratings yet
- SKIN Tumors With Apocrine DifferentiationDocument101 pagesSKIN Tumors With Apocrine DifferentiationchinnnababuNo ratings yet
- BoardReviewPart1B BenignHemePathDocument155 pagesBoardReviewPart1B BenignHemePathMaria Cristina Alarcon NietoNo ratings yet
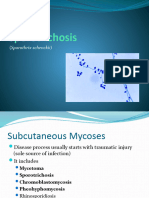
- SporotrichosisDocument32 pagesSporotrichosisRajkishor YadavNo ratings yet
- DR Meenakshi MDS Oral PathologyDocument29 pagesDR Meenakshi MDS Oral PathologyDr. Meenakshi SinghalNo ratings yet
- Mu CosaDocument222 pagesMu CosaAliImadAlKhasakiNo ratings yet
- Differential Diagnosis 1. Atopic Dermatitis History TakingDocument13 pagesDifferential Diagnosis 1. Atopic Dermatitis History TakingCocoi MellaNo ratings yet
- General Pathology of The NoseDocument25 pagesGeneral Pathology of The NoseMou Thiik MadutNo ratings yet
- D.D of Mid-Line Neck SwellingsDocument21 pagesD.D of Mid-Line Neck Swellingsmhmdalbdyny764No ratings yet
- Ilovepdf MergedDocument22 pagesIlovepdf MergedSRO oONo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Advances in Radiation Oncology in Lung Cancer 2nd EditionDocument814 pagesAdvances in Radiation Oncology in Lung Cancer 2nd EditionAna-Maria IacobutaNo ratings yet
- Inhibidores TRK en Cáncer 2019Document8 pagesInhibidores TRK en Cáncer 2019JA VelascoNo ratings yet
- Hemoptysis - CA Bronchus PDFDocument49 pagesHemoptysis - CA Bronchus PDFDarawan MirzaNo ratings yet
- IHC ProtocolsDocument438 pagesIHC Protocolsshivam jaiswalNo ratings yet
- Rodriguez Canales2016Document22 pagesRodriguez Canales2016Triaprasetya HadiNo ratings yet
- AlectinibDocument22 pagesAlectinibIoana GhirvuNo ratings yet
- A Detailed Multi-Omics Analysis of GNB2 Gene in Human CancersDocument10 pagesA Detailed Multi-Omics Analysis of GNB2 Gene in Human CancersLuliNo ratings yet
- Hitoshi Nakagama NCCJ 2018 - ANNCA - 20181023Document47 pagesHitoshi Nakagama NCCJ 2018 - ANNCA - 20181023Ardani NugrahaNo ratings yet
- Hornick Pediatric Fibroblastic-Myofibroblastic Neoplasms 10 June 1400Document93 pagesHornick Pediatric Fibroblastic-Myofibroblastic Neoplasms 10 June 1400Olteanu Dragos-NicolaeNo ratings yet
- Supplementary Table 1. A Full List of Cancer GenesDocument685 pagesSupplementary Table 1. A Full List of Cancer GenesFaruque HossainNo ratings yet
- Internal Assessment 3Document2 pagesInternal Assessment 33Tamil mullainathanNo ratings yet
- Histopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDocument4 pagesHistopathologic Analysis of Ct-Guided Core Needle Biopsy in Radiologically Detected Suspicious Mediastinal and Lung Mass: Two Years' Study in Tertiary HospitalDesiree MejicaNo ratings yet
- ESP Lisabona 2013 AbstractsDocument252 pagesESP Lisabona 2013 AbstractsstripandslipNo ratings yet
- 1 s2.0 S0169500221004062 MainDocument9 pages1 s2.0 S0169500221004062 MainandresdemedNo ratings yet
- Jurnal Kanker Paru-ParuDocument11 pagesJurnal Kanker Paru-Parufidella uccaNo ratings yet
- T Cell Lymphomas 2022 SlidesDocument62 pagesT Cell Lymphomas 2022 SlidesИван НегарэNo ratings yet
- NeuroblastomaDocument19 pagesNeuroblastomaTri Andhika Dessy WahyuniNo ratings yet
- MilliwaysDocument12 pagesMilliwaysTurtle ArtNo ratings yet
- Precision Medicine in Lung CancerDocument12 pagesPrecision Medicine in Lung Cancerswastik panditaNo ratings yet
- Repurposing of Kinase Inhibitors To Target C-Abl As PotentialDocument10 pagesRepurposing of Kinase Inhibitors To Target C-Abl As PotentialShreeya BhatNo ratings yet
- Nejmcpc 1102202Document10 pagesNejmcpc 1102202FrinkooFrinkoBNo ratings yet
- 2015 Cdi Ihc CatalogDocument75 pages2015 Cdi Ihc CatalogDavid MuñozNo ratings yet
- Diagnostic BioSystems CatalogDocument116 pagesDiagnostic BioSystems CatalogCris StefanNo ratings yet
- Jurnal Tirosin Kinase 4Document13 pagesJurnal Tirosin Kinase 4Maya SariNo ratings yet
- G. Mauger - Cours de Langue Et de Civilisation FrançaisesDocument619 pagesG. Mauger - Cours de Langue Et de Civilisation FrançaisesAdrian Mucileanu0% (1)