Download as pptx, pdf, or txt
You might also like
- Mastering Your Adult ADHDDocument185 pagesMastering Your Adult ADHDNatália Matteoli Abatti100% (7)
- Trichotillomania - An ACT-Enhanced Behavior Therapy Approach (Therapist Guide) (Woods, Douglas W.,Twohig, Michael P.)Document128 pagesTrichotillomania - An ACT-Enhanced Behavior Therapy Approach (Therapist Guide) (Woods, Douglas W.,Twohig, Michael P.)Yılmaz Kafalı HelinNo ratings yet
- Mathematical Reasoning Analogies, Metaphors, and ImagesDocument393 pagesMathematical Reasoning Analogies, Metaphors, and Imageskiran nalam50% (2)
- Safren CBT-AD PDFDocument169 pagesSafren CBT-AD PDFJuan Murillo100% (4)
- Reflection Has Become An Important Concept in Nursing Nursing EssayDocument3 pagesReflection Has Become An Important Concept in Nursing Nursing EssayNavinYattiNo ratings yet
- Concept MappingDocument39 pagesConcept MappingRaquel M. Mendoza100% (2)
- Sas 1 25 2Document31 pagesSas 1 25 2KIMBERLY CABATONo ratings yet
- GOALS FOR CONDUCTING NURSING RESEARCH The Importance of Nursing Research Cannot Be Stressed EnoughDocument4 pagesGOALS FOR CONDUCTING NURSING RESEARCH The Importance of Nursing Research Cannot Be Stressed EnoughTess De VeraNo ratings yet
- Anu Unit 1 Nursing Research 2010Document101 pagesAnu Unit 1 Nursing Research 2010Radhakrishnan Govindan100% (1)
- BACHELOR IN NURSING - Docx (Reflection)Document9 pagesBACHELOR IN NURSING - Docx (Reflection)siti husniNo ratings yet
- NUPC 103: Dario M. Ragmac, RNDocument26 pagesNUPC 103: Dario M. Ragmac, RNArmie Erika JovellanosNo ratings yet
- Evidence Based Practice in NursingDocument9 pagesEvidence Based Practice in NursingSimran Chauhan100% (2)
- KT Article Questions Team Session 2 1Document6 pagesKT Article Questions Team Session 2 1api-437756187No ratings yet
- Clinical Reasoning: Linking Theory To Practice and Practice To TheoryDocument14 pagesClinical Reasoning: Linking Theory To Practice and Practice To Theorylumac1087831No ratings yet
- Research Unit I Nursing ResearchDocument37 pagesResearch Unit I Nursing ResearchSyed BuRhan Ud-DinNo ratings yet
- Evidence Based Medicine 2020septDocument82 pagesEvidence Based Medicine 2020septTinaNo ratings yet
- And Utilization of Nursing ResourcesDocument10 pagesAnd Utilization of Nursing ResourcesSimran ChauhanNo ratings yet
- Phases of Nursing ResearchDocument12 pagesPhases of Nursing ResearchAmbroseNo ratings yet
- Intro To ResearchDocument2 pagesIntro To ResearchRonel ResurricionNo ratings yet
- Hand-0ut 1 Inres PrelimsDocument7 pagesHand-0ut 1 Inres PrelimsJustin LimboNo ratings yet
- Research Activity ExampleDocument5 pagesResearch Activity ExampleJay VillasotoNo ratings yet
- Problem SolvingDocument3 pagesProblem SolvingBahaa Ahmad Assoud50% (2)
- Week4 WikikDocument8 pagesWeek4 Wikikapi-294721909No ratings yet
- Unit 1 (C) Nursing ProcessDocument43 pagesUnit 1 (C) Nursing ProcessSumaira NoreenNo ratings yet
- Ms. Chithra Chandran A. First Year MSC Nursing Govt. College of Nursing KottayamDocument54 pagesMs. Chithra Chandran A. First Year MSC Nursing Govt. College of Nursing Kottayamchithrajayakrishnan100% (1)
- Health Assessment: An: Diana Rose D. Emerenciana, RN., ManDocument72 pagesHealth Assessment: An: Diana Rose D. Emerenciana, RN., ManSM CervantesNo ratings yet
- Jayson NovellesDocument38 pagesJayson Novellesaronara dalampasiganNo ratings yet
- PICOTDocument5 pagesPICOTjorge eryNo ratings yet
- Roemenie Evidence Based Practice ExercisesDocument2 pagesRoemenie Evidence Based Practice ExercisesCristinaSohorcaNo ratings yet
- Nursing Process: Claudette Mcgregor-Coombs, MSN, ArnpDocument63 pagesNursing Process: Claudette Mcgregor-Coombs, MSN, ArnpDanou_Bennett__828No ratings yet
- Module 7 Concept IntegrationDocument14 pagesModule 7 Concept Integrationmuriel bautistaNo ratings yet
- Nursing ResearchDocument125 pagesNursing ResearchDebayn CandidatoNo ratings yet
- Facilitating Case Studies in Massage Therapy CliniDocument5 pagesFacilitating Case Studies in Massage Therapy ClinijorgenovachrolloNo ratings yet
- NURS3515 Midterm Notes YORKDocument93 pagesNURS3515 Midterm Notes YORKelizabeth.morozov03No ratings yet
- Occupational Therapy For Physical Dysfunction - Latham, Catherine A. Trombly - 1989 - Baltimore - Williams & Wilkins - 9780683083897 - Anna's ArchiveDocument652 pagesOccupational Therapy For Physical Dysfunction - Latham, Catherine A. Trombly - 1989 - Baltimore - Williams & Wilkins - 9780683083897 - Anna's Archivesaurav.das2030No ratings yet
- Cognitive Rehabilitation Programs in Schizophrenia PDFDocument26 pagesCognitive Rehabilitation Programs in Schizophrenia PDFMeindayaniNo ratings yet
- Improving Documentation Using A Nursing ModelDocument10 pagesImproving Documentation Using A Nursing ModelLaraBindeNo ratings yet
- Nursing Research Lec 09Document116 pagesNursing Research Lec 09malyn1218100% (2)
- RLE MODULE PediaDocument14 pagesRLE MODULE PediaFrancis Alfred EscaranNo ratings yet
- NUR 206 Journal Assign 1Document6 pagesNUR 206 Journal Assign 1vawters03100% (1)
- Kerry Thoirs Presentation 18 Nov 16Document13 pagesKerry Thoirs Presentation 18 Nov 16Rana EL-BakryNo ratings yet
- (Treatments That Work) Kelly J Rohan - Coping With The Seasons - A Cognitive Behavioral Approach To Seasonal Affective Disorder, Therapist Guide-Oxford University Press, USA (2008)Document152 pages(Treatments That Work) Kelly J Rohan - Coping With The Seasons - A Cognitive Behavioral Approach To Seasonal Affective Disorder, Therapist Guide-Oxford University Press, USA (2008)Jack MertensNo ratings yet
- Introduction To ResearchDocument32 pagesIntroduction To ResearchSudipta Debnath100% (1)
- MECOR LA - L1 Protocol Outline - 2018Document3 pagesMECOR LA - L1 Protocol Outline - 2018María Cristina ArveloNo ratings yet
- FDARDocument41 pagesFDARJojo Justo100% (2)
- Translation Research-Semnas FKP-30 Nov-NursDocument106 pagesTranslation Research-Semnas FKP-30 Nov-NursIzzatul KamilahNo ratings yet
- Week 6 The Research ProblemDocument12 pagesWeek 6 The Research ProblemAngela NeriNo ratings yet
- Fundies II Exam 1 Blue PrintDocument24 pagesFundies II Exam 1 Blue PrintStephanieNo ratings yet
- Mindfulness-Based Psychotherapy in Patients With oDocument10 pagesMindfulness-Based Psychotherapy in Patients With oMiriamNo ratings yet
- Introduction by SaadaDocument22 pagesIntroduction by SaadaShadrech MgeyekhwaNo ratings yet
- The Culture of Healthcare: Healthcare Processes and Decision MakingDocument11 pagesThe Culture of Healthcare: Healthcare Processes and Decision MakingHealth IT Workforce Curriculum - 2012No ratings yet
- SAS Session 15 Research 1Document4 pagesSAS Session 15 Research 1Sabrina MascardoNo ratings yet
- Nursing Research 1 OverviewDocument74 pagesNursing Research 1 Overviewgeng geng100% (1)
- Handout - Facilitating Clinical ReasoningDocument6 pagesHandout - Facilitating Clinical Reasoningdelap05No ratings yet
- 1427 - Rana Kachouh Nursing Process HammoudDocument54 pages1427 - Rana Kachouh Nursing Process HammoudRumela Ganguly ChakrabortyNo ratings yet
- Research1Document77 pagesResearch1Ces AriaNo ratings yet
- Tugas MetodologiDocument4 pagesTugas MetodologiOga 12No ratings yet
- What Is Evidence-Based Practice?Document7 pagesWhat Is Evidence-Based Practice?dennise reyesNo ratings yet
- 001 - Nida Najiyah - NURSING PROCESS AS A SCIENTIFIC METHOD IN PROBLEM SOLVING - Id.enDocument7 pages001 - Nida Najiyah - NURSING PROCESS AS A SCIENTIFIC METHOD IN PROBLEM SOLVING - Id.enChristine HevinNo ratings yet
- Research Module 1Document7 pagesResearch Module 1brianna.aldrich1004No ratings yet
- Nutrition and VitaminDocument70 pagesNutrition and VitaminTob JurNo ratings yet
- Ca Colon 6Document28 pagesCa Colon 6Tob JurNo ratings yet
- Cultivating Mindfulness of Bodhichitta c5 PDFDocument12 pagesCultivating Mindfulness of Bodhichitta c5 PDFTob JurNo ratings yet
- Proteins: DR Sonam Chhoden RDocument33 pagesProteins: DR Sonam Chhoden RTob JurNo ratings yet
- Colon Cancer Care Plan PDFDocument4 pagesColon Cancer Care Plan PDFTob JurNo ratings yet
- Finn 228Document12 pagesFinn 228Tob JurNo ratings yet
- 2016 WHO Antenatal Care Guidelines: Malaria in Pregnancy Frequently Asked Questions (FAQ)Document6 pages2016 WHO Antenatal Care Guidelines: Malaria in Pregnancy Frequently Asked Questions (FAQ)Tob JurNo ratings yet
- Ca Colon 2Document19 pagesCa Colon 2Tob JurNo ratings yet
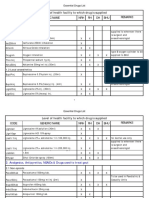
- Code Generic Name NRH RH DH BHU Remarks Level of Health Facility To Which Drug Is SuppliedDocument42 pagesCode Generic Name NRH RH DH BHU Remarks Level of Health Facility To Which Drug Is SuppliedTob JurNo ratings yet
- Antenatal Summary Visits PDFDocument2 pagesAntenatal Summary Visits PDFTob JurNo ratings yet
- G12 SLM4 Q4 Creative WritingDocument24 pagesG12 SLM4 Q4 Creative WritingrachelleNo ratings yet
- OmniGuide Kat PausoDocument103 pagesOmniGuide Kat PausoMnuel NcmNo ratings yet
- Combined Gas Law 7 E'sDocument5 pagesCombined Gas Law 7 E'sGelCess Paroan100% (1)
- FORMATDocument21 pagesFORMATAura Nica TrinidadNo ratings yet
- Relationship Between Reading Habits, University Library and Academic Performance in A Sample of Psychology StudentsDocument22 pagesRelationship Between Reading Habits, University Library and Academic Performance in A Sample of Psychology StudentsDwi MegawatiNo ratings yet
- Mbbs Curriculum BrochureDocument15 pagesMbbs Curriculum BrochureLavinia MihaiNo ratings yet
- DO - s2013 - 020 (PASBE)Document65 pagesDO - s2013 - 020 (PASBE)Debby Gel100% (2)
- Arithmetic Sequence 2Document3 pagesArithmetic Sequence 2Eric de GuzmanNo ratings yet
- Identifying Strengths and Weaknesses of The LernerDocument3 pagesIdentifying Strengths and Weaknesses of The Lernerapi-282794809No ratings yet
- Running Head: Parental Involvement in Schools 1Document21 pagesRunning Head: Parental Involvement in Schools 1api-295671216No ratings yet
- Terminal Report For Work ImmersionDocument2 pagesTerminal Report For Work Immersionfloreslorna86No ratings yet
- Cultural Functions in PracticeDocument5 pagesCultural Functions in Practiceapi-541113831100% (1)
- Creating Mature Thinkers in Interior Design: Pathways of Intellectual DevelopmentDocument20 pagesCreating Mature Thinkers in Interior Design: Pathways of Intellectual DevelopmentNate Humble Jr.No ratings yet
- CLASS 7 Final SyllabusDocument29 pagesCLASS 7 Final Syllabussuchitra sahooNo ratings yet
- PJDocument2 pagesPJPhranxies Jean BlayaNo ratings yet
- Mini Project-Students Perceptions On Online Learning During COVID-19Document13 pagesMini Project-Students Perceptions On Online Learning During COVID-19Gayatheri PerumalNo ratings yet
- Personnel Standards Guide: Maryland's Early Intervention and Preschool Special Education SystemDocument22 pagesPersonnel Standards Guide: Maryland's Early Intervention and Preschool Special Education System2PlusNo ratings yet
- 2024 - Authentic Leadership and Conflict Management Among Youth inDocument21 pages2024 - Authentic Leadership and Conflict Management Among Youth inzuraidahjulianaNo ratings yet
- DRJJ Measure Assess Evaluate ADPRIMA N More 17052012Document25 pagesDRJJ Measure Assess Evaluate ADPRIMA N More 17052012css_saidNo ratings yet
- 2023 Oct CSC649 Group Project - Evaluation FormDocument1 page2023 Oct CSC649 Group Project - Evaluation FormMUHAMMAD AMER FAIZ BIN ABDUL RAHMANNo ratings yet
- Portfolio in PTDocument200 pagesPortfolio in PTJojane lambayan100% (3)
- Philosophy of Arts EducationDocument7 pagesPhilosophy of Arts Educationjane barquin100% (1)
- Machine Learning ReportDocument16 pagesMachine Learning Reportgreywolf 18No ratings yet
- Lesson Plan in Empowerment Technology Grade 11 - Computer Systems ServicingDocument2 pagesLesson Plan in Empowerment Technology Grade 11 - Computer Systems Servicingjoey mamonNo ratings yet
- Srinivasan Services Trust: PedagogyDocument13 pagesSrinivasan Services Trust: Pedagogybala subramanianNo ratings yet
- Chapter 9 Fluency Oriented Second Language TeachingDocument21 pagesChapter 9 Fluency Oriented Second Language TeachingAhmedNo ratings yet
- ADEC - Elite Private School 2016-2017Document19 pagesADEC - Elite Private School 2016-2017Edarabia.comNo ratings yet
- SEGAMAT SPM TRIAL 2022 Paper 1Document13 pagesSEGAMAT SPM TRIAL 2022 Paper 1Zikri SyahmiNo ratings yet
- Ict Lesson Plan 2 PDFDocument2 pagesIct Lesson Plan 2 PDFReuelMichaels100% (1)