Download as pptx, pdf, or txt
You might also like
- Collins-Donnelly, Kate (2014) Starving The Anxiety Gremlin For Children Aged 5-9 A CBT Workbook On Anxiety ManagementDocument193 pagesCollins-Donnelly, Kate (2014) Starving The Anxiety Gremlin For Children Aged 5-9 A CBT Workbook On Anxiety ManagementG100% (1)
- Philosophy of LawDocument8 pagesPhilosophy of LawEm Asiddao-DeonaNo ratings yet
- Mumbai CxoDocument9 pagesMumbai CxopoonamNo ratings yet
- Bronchiectasis DesieDocument77 pagesBronchiectasis DesieAbebe GelawNo ratings yet
- BronchiectasisDocument17 pagesBronchiectasisShannon RamsumairNo ratings yet
- BronchiectasisDocument21 pagesBronchiectasisEliza ButtNo ratings yet
- Update Diagnosis and TherapyDocument29 pagesUpdate Diagnosis and TherapyRosi AmaliaNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document23 pagesChronic Obstructive Pulmonary Disease (COPD)akoeljames8543No ratings yet
- Bronchiectasis: By: Karunesh KumarDocument21 pagesBronchiectasis: By: Karunesh KumarAnkan DeyNo ratings yet
- BronchiectasisDocument20 pagesBronchiectasisSajjal JohnsonNo ratings yet
- Interstitial Lung Disease Diffuse Parenchymal Lung DiseaseDocument59 pagesInterstitial Lung Disease Diffuse Parenchymal Lung Diseaseapi-19641337100% (1)
- Suppurative Lung DIseaseDocument33 pagesSuppurative Lung DIseaseNur Liyana Ahmad ZakiNo ratings yet
- Surgical Aspects of Pulmonary Infections: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonDocument60 pagesSurgical Aspects of Pulmonary Infections: Kibrom Gebreselassie, MD, FCS-ECSA Cardiovascular and Thoracic SurgeonVincent SerNo ratings yet
- CopdDocument89 pagesCopdVijayalaxmi KathareNo ratings yet
- Mr. Maheboob 1 Year M.SC Nursing Govt College of Nursing HolenarsipurDocument44 pagesMr. Maheboob 1 Year M.SC Nursing Govt College of Nursing HolenarsipurDr Tahira NihalNo ratings yet
- Cystic FibrosisDocument45 pagesCystic FibrosisAbong Che InnocentNo ratings yet
- Nursing InterventionsDocument68 pagesNursing Interventionsash aliNo ratings yet
- Diffuse Pulmonary DiseasesDocument19 pagesDiffuse Pulmonary DiseasessivaNo ratings yet
- BRONCHIECTASISDocument19 pagesBRONCHIECTASISAbong Che InnocentNo ratings yet
- Bronchiectasis - AiimsrisDocument118 pagesBronchiectasis - AiimsrisElteyb Nor eldaimNo ratings yet
- Disorders of The Respiratory SystemDocument58 pagesDisorders of The Respiratory SystemgogoNo ratings yet
- Chapter 15 - The LungDocument17 pagesChapter 15 - The LungAgnieszka WisniewskaNo ratings yet
- RESTRICTIVE LUNG DISEASES (Autosaved)Document40 pagesRESTRICTIVE LUNG DISEASES (Autosaved)Dr. Rabail MalikNo ratings yet
- Chronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesDocument59 pagesChronic Obstructive Lung Diseases and Chronic Restrictive Lung DiseasesGEORGENo ratings yet
- Bronchiectasis & AtelektasisDocument39 pagesBronchiectasis & AtelektasisFalensia Dwita LestariNo ratings yet
- Respiratory DiseasesDocument58 pagesRespiratory Diseasesajsjs13No ratings yet
- Interstitial Lung Disease (ILD)Document42 pagesInterstitial Lung Disease (ILD)AkhilaNo ratings yet
- Chronic Obstructive Disease by HibaDocument38 pagesChronic Obstructive Disease by HibahibaNo ratings yet
- Suppurative Lung Diseases.Document37 pagesSuppurative Lung Diseases.Salman KhanNo ratings yet
- PneumoniaDocument66 pagesPneumoniasamakayigrace808No ratings yet
- Bronchiectasis OkDocument60 pagesBronchiectasis OkImmanuelNo ratings yet
- BronchiectasisDocument17 pagesBronchiectasisBaiqLinaAnggrianNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- BronchiectasisDocument14 pagesBronchiectasisNipul MondolNo ratings yet
- Bronchiectas IS: Dr.B.Chakradhar MD Assistant Professor Dept of Respiratory MedicineDocument40 pagesBronchiectas IS: Dr.B.Chakradhar MD Assistant Professor Dept of Respiratory MedicineChakradhar ChakrreNo ratings yet
- Surgery & Pediatrics SurgeryDocument111 pagesSurgery & Pediatrics SurgeryHIMANSHU GUPTANo ratings yet
- Chronic Obstructive Pulmonary Disease: TH NDDocument22 pagesChronic Obstructive Pulmonary Disease: TH NDSuhaila Naif NasserNo ratings yet
- PNEUMONIASDocument25 pagesPNEUMONIASfrankozed1No ratings yet
- Dr. M Abdur Rahim M.D.,: Asst. Professor of MedicineDocument59 pagesDr. M Abdur Rahim M.D.,: Asst. Professor of Medicinemushtaq_23No ratings yet
- Lecture Lung Diseases-1 Eng 2016-11-23Document92 pagesLecture Lung Diseases-1 Eng 2016-11-23ramtinNo ratings yet
- Lesson25 (2) - Management of Chronic CoughDocument27 pagesLesson25 (2) - Management of Chronic CoughAditi JainNo ratings yet
- Pathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenDocument22 pagesPathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenAlexander Santiago ParelNo ratings yet
- BronchiectasisDocument24 pagesBronchiectasisMuhammad HaziqNo ratings yet
- PatomekanismeDocument18 pagesPatomekanismeEdwin Pasha Jr.No ratings yet
- Bronchiectasis - Ppt-Medina Presentation2Document25 pagesBronchiectasis - Ppt-Medina Presentation2chebetnaomi945No ratings yet
- Day 5 Respiratory DiseaseDocument71 pagesDay 5 Respiratory DiseaseRamzen Raphael DomingoNo ratings yet
- Cystic FibrosisDocument26 pagesCystic FibrosisEliza ButtNo ratings yet
- Brochiectasis & Atelectasis: Erwin AriefDocument77 pagesBrochiectasis & Atelectasis: Erwin AriefAlfiana RahmanNo ratings yet
- Asthma: Pre by Lect. ZAHID REHMAN Ipms (Kmu)Document29 pagesAsthma: Pre by Lect. ZAHID REHMAN Ipms (Kmu)SHAFI ULLAHNo ratings yet
- 2.6.3 - BronchiectasisDocument11 pages2.6.3 - BronchiectasiskaryndpNo ratings yet
- Bronchiectasis: Yuping GuoDocument75 pagesBronchiectasis: Yuping GuoAmeliaNo ratings yet
- B&lung AbscessDocument21 pagesB&lung Abscessnathan asfahaNo ratings yet
- BronchiectasisDocument21 pagesBronchiectasisMuhammad Iyhan NuriansyahNo ratings yet
- Lower Respiratory InfectionDocument71 pagesLower Respiratory Infectionpaulyn ramos100% (1)
- BronchiectasisDocument30 pagesBronchiectasisMark Gizle PapagayoNo ratings yet
- Pneumonia 150514133315 Lva1 App6892Document34 pagesPneumonia 150514133315 Lva1 App6892SadiaNo ratings yet
- Acute BronchitisDocument26 pagesAcute Bronchitiswwd2m29xr7No ratings yet
- Chapter Title: Pulmonary Disease ManagementDocument5 pagesChapter Title: Pulmonary Disease ManagementCharisa Antonette HuelvaNo ratings yet
- Lower Airway Dysfunctions: Margaret Xaira R. Mercado, RNDocument52 pagesLower Airway Dysfunctions: Margaret Xaira R. Mercado, RNMargaret Xaira Rubio MercadoNo ratings yet
- Bronchoobstructive SyndromeDocument45 pagesBronchoobstructive SyndromeNahanNo ratings yet
- BronchiectasisDocument25 pagesBronchiectasisDewi PermatasariNo ratings yet
- Aquire Pathology of Respiratory SystemDocument96 pagesAquire Pathology of Respiratory SystemBasit HussainNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Congenital Talipes EquinovarusDocument11 pagesCongenital Talipes EquinovarusOeyi Mutia SatifaNo ratings yet
- Neurogenic BladderDocument14 pagesNeurogenic BladderOeyi Mutia SatifaNo ratings yet
- Spina BifidaDocument9 pagesSpina BifidaOeyi Mutia SatifaNo ratings yet
- Hydrocephalus WPS OfficeDocument16 pagesHydrocephalus WPS OfficeOeyi Mutia SatifaNo ratings yet
- Family Apgar: Almost Always (2) Some of The Time (1) Hardly EverDocument2 pagesFamily Apgar: Almost Always (2) Some of The Time (1) Hardly EverOeyi Mutia Satifa100% (1)
- LO 6 PolisitemiaDocument5 pagesLO 6 PolisitemiaOeyi Mutia SatifaNo ratings yet
- LO 2 Amenorea Dan DismenoreaDocument8 pagesLO 2 Amenorea Dan DismenoreaOeyi Mutia SatifaNo ratings yet
- The Residences at Greenbelt Manila Tower 1-Bedroom For Sale 24DDocument2 pagesThe Residences at Greenbelt Manila Tower 1-Bedroom For Sale 24DJP ReyesNo ratings yet
- Empower 2e B1+ Word List GermanDocument94 pagesEmpower 2e B1+ Word List GermanwaiNo ratings yet
- Goldfarb School of Nursing at Barnes-Jewish College Textbooks - Summer 2020Document6 pagesGoldfarb School of Nursing at Barnes-Jewish College Textbooks - Summer 2020brad0% (1)
- Kid Friendly 8th Grade California State StandardsDocument2 pagesKid Friendly 8th Grade California State StandardsEmily Q. LiuNo ratings yet
- ATPAR ReviewerDocument25 pagesATPAR ReviewerJohn Paul BuliyatNo ratings yet
- Lessonplans Self ProtectionDocument6 pagesLessonplans Self ProtectionteacherasyikinNo ratings yet
- C5. Catholic Vicar Apostolic of The Mt. Province v. Court of Appeals, 165 SCRA 515Document5 pagesC5. Catholic Vicar Apostolic of The Mt. Province v. Court of Appeals, 165 SCRA 515dondzNo ratings yet
- Asso V EnergyDocument38 pagesAsso V Energyarriane joy insularNo ratings yet
- Cambridge, 2nd Ed.-Petty Cash BookDocument3 pagesCambridge, 2nd Ed.-Petty Cash BookShannen LyeNo ratings yet
- Managing Clean Core For SAP S4HANA Cloud NotesDocument59 pagesManaging Clean Core For SAP S4HANA Cloud NotesGLEN KGATLANo ratings yet
- Secret Tradition in Freemasonry. ARTHUR EDWARD WAITE PDFDocument488 pagesSecret Tradition in Freemasonry. ARTHUR EDWARD WAITE PDFZárate89% (9)
- The Power of Good WorksDocument5 pagesThe Power of Good WorksRyan Bladimer RubioNo ratings yet
- FMGE Recall 1Document46 pagesFMGE Recall 1Ritik BhardwajNo ratings yet
- Discovering Computers Enhanced Edition ©2017: Introducing Today's TechnologiesDocument37 pagesDiscovering Computers Enhanced Edition ©2017: Introducing Today's TechnologiesKent PerezNo ratings yet
- Twelve Metaphors For JournalismDocument5 pagesTwelve Metaphors For JournalismMarla SanidNo ratings yet
- 2019 How Planetary Systems FormDocument5 pages2019 How Planetary Systems FormFavianna Colón IrizarryNo ratings yet
- Chapter IIIDocument3 pagesChapter IIIRenan S. GuerreroNo ratings yet
- Chemical Analysis of Caustic Soda and Caustic Potash (Sodium Hydroxide and Potassium Hydroxide)Document16 pagesChemical Analysis of Caustic Soda and Caustic Potash (Sodium Hydroxide and Potassium Hydroxide)wilfred gomezNo ratings yet
- Government of Khyber Pakhtunkhwa: Project Title: Public Policy & Social Protection Reforms UnitDocument2 pagesGovernment of Khyber Pakhtunkhwa: Project Title: Public Policy & Social Protection Reforms UnitSafiurrehmanNo ratings yet
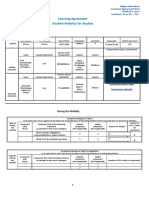
- Learning Agreement During The MobilityDocument3 pagesLearning Agreement During The MobilityVictoria GrosuNo ratings yet
- Dan Webb Concealment GradeDocument2 pagesDan Webb Concealment Gradeapi-565691734No ratings yet
- Regulating Social Media in The Global South by Zahra TakhshidDocument56 pagesRegulating Social Media in The Global South by Zahra TakhshidJosé Luis SilveroNo ratings yet
- Introduction To Law 1.: Meaning and Definition of LawDocument33 pagesIntroduction To Law 1.: Meaning and Definition of LawArthur p90No ratings yet
- Underwood C. P., "HVAC Control Systems, Modelling Analysis and Design" RoutledgeDocument2 pagesUnderwood C. P., "HVAC Control Systems, Modelling Analysis and Design" Routledgeatif shaikhNo ratings yet
- Keraplast Wound Care BrochureDocument4 pagesKeraplast Wound Care BrochureclventuriniNo ratings yet
- E-Vehicle Article FinalDocument22 pagesE-Vehicle Article Finalvishnu varthanNo ratings yet
- 1 Miner: Source: University of Manchester Institute of Science and Technology (UK)Document2 pages1 Miner: Source: University of Manchester Institute of Science and Technology (UK)NI WAYAN KERTINo ratings yet