Download as ppt, pdf, or txt
You might also like
- The Management of DVT: Dr. Heru Sulastomo, SP - JP (K), FIHA Dr. Ahmad Yasa', SP - JP, FIHA, MkesDocument19 pagesThe Management of DVT: Dr. Heru Sulastomo, SP - JP (K), FIHA Dr. Ahmad Yasa', SP - JP, FIHA, MkesDEWI MULYANINo ratings yet
- Nursing CatalogDocument27 pagesNursing Catalogrrockel100% (1)
- Principles of Epidemiology in Public Health PracticeDocument512 pagesPrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (4)
- Pragmatic Use of NOACDocument38 pagesPragmatic Use of NOACDr. Pradip MateNo ratings yet
- S Shapiro VTE Prevention AND COVID ThrombosisUK May 2020Document22 pagesS Shapiro VTE Prevention AND COVID ThrombosisUK May 2020Ririn Efsa JutiaNo ratings yet
- VTE: 2016 ACCP Update With Best Evidence and Best PracticesDocument78 pagesVTE: 2016 ACCP Update With Best Evidence and Best Practicesagustina mereNo ratings yet
- Covid Coagulopathy Pit Papdi 2020Document46 pagesCovid Coagulopathy Pit Papdi 2020alvarocfad140699No ratings yet
- Tromboprofilaxis y TVP PDFDocument16 pagesTromboprofilaxis y TVP PDFDarío ParraNo ratings yet
- Venous Thromboembolism in MalignancyDocument3 pagesVenous Thromboembolism in MalignancyAzmi FarhadiNo ratings yet
- Thromboprophylaxis in The ICUDocument31 pagesThromboprophylaxis in The ICUdocansh100% (1)
- Management of DVTDocument46 pagesManagement of DVTSteven Hartanto Kurniawan50% (2)
- New VTE Terbaru FixDocument68 pagesNew VTE Terbaru FixSurya MahardikaNo ratings yet
- Rivaroxaban For VTEDocument35 pagesRivaroxaban For VTENur Sabriany LihawaNo ratings yet
- Venous ThromboembolismDocument118 pagesVenous ThromboembolismPrincewill SeiyefaNo ratings yet
- Agnes Lee Thrombosis PresentationDocument37 pagesAgnes Lee Thrombosis Presentationari naNo ratings yet
- Thromboembolic Disease PDFDocument5 pagesThromboembolic Disease PDFBáĦẳá Y. Ẳl-mársǾúmiNo ratings yet
- Pulmonary EmbolismDocument70 pagesPulmonary EmbolismAjana SivadechathepNo ratings yet
- Update On Clinical Management - PrivateDocument57 pagesUpdate On Clinical Management - PrivateJashveerBediNo ratings yet
- DTC Guidline 2015 ResidentsDocument60 pagesDTC Guidline 2015 ResidentsOsama alshaailiNo ratings yet
- MX of COVID-19Document49 pagesMX of COVID-19anisNo ratings yet
- Bridging AnticoagulantDocument29 pagesBridging AnticoagulantTessa OktaramdaniNo ratings yet
- Int J of Urology - 2017 - Saluja - Venous Thromboembolism Prophylaxis in Urology A ReviewDocument5 pagesInt J of Urology - 2017 - Saluja - Venous Thromboembolism Prophylaxis in Urology A ReviewsofiaNo ratings yet
- Venous Thromboembolism (VTE) : Quality DepartmentDocument28 pagesVenous Thromboembolism (VTE) : Quality DepartmentDIGITAL 143No ratings yet
- Non Pharmacological Method For Prevention and Treatment ofDocument34 pagesNon Pharmacological Method For Prevention and Treatment ofBhaskar Borgohain100% (2)
- Dr. Idar SP - PD, SP - JP DVTDocument20 pagesDr. Idar SP - PD, SP - JP DVTarnipahlawaniNo ratings yet
- DIVITI Slide Prophylaxis VTE SPPD Ringkas-1Document11 pagesDIVITI Slide Prophylaxis VTE SPPD Ringkas-1Fera NurrizaNo ratings yet
- Obstetric EmbolismDocument81 pagesObstetric Embolismmiss_izzniNo ratings yet
- Questions For UNSW Mock Biomed VivaDocument67 pagesQuestions For UNSW Mock Biomed VivaReuben TangNo ratings yet
- FR040 JuddDocument170 pagesFR040 JuddAlifiah Putri BaharuddinNo ratings yet
- Kuliah DVTDocument29 pagesKuliah DVTluluksNo ratings yet
- Venous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentDocument25 pagesVenous Thromboembolism in Urologic Surgery: Prophylaxis, Diagnosis and TreatmentapheatNo ratings yet
- Deep Vein Thrombosis & Its ProphylaxisDocument90 pagesDeep Vein Thrombosis & Its ProphylaxisPratik KumarNo ratings yet
- HAUT HMV Brazil Grand Rounds April 29 2014Document74 pagesHAUT HMV Brazil Grand Rounds April 29 2014carlosrschusterNo ratings yet
- Thromboprophylaxis in ICU: Dr. Rajnish K. JainDocument31 pagesThromboprophylaxis in ICU: Dr. Rajnish K. JainMaysson Mohamed Galal AbbasNo ratings yet
- 508 - MAPPP 2017 Presentation-Final 5-12-17Document73 pages508 - MAPPP 2017 Presentation-Final 5-12-17Joanne HoNo ratings yet
- Dokumen - Tips Deep Vein Thrombosis Mayo Clinic Venous Thrombosis Deep Vein Thrombosis inDocument47 pagesDokumen - Tips Deep Vein Thrombosis Mayo Clinic Venous Thrombosis Deep Vein Thrombosis inTeuku Ilham AkbarNo ratings yet
- Thrombus Removal After DVTDocument39 pagesThrombus Removal After DVTromany barsoomNo ratings yet
- Analisis Guias Valvulas ESCDocument9 pagesAnalisis Guias Valvulas ESCCamiloRadaNo ratings yet
- VTE Risk Assessment: DR Roopen AryaDocument26 pagesVTE Risk Assessment: DR Roopen AryaA.h.MuradNo ratings yet
- Pre Op GuidelinesDocument11 pagesPre Op GuidelinesHanif FebrianNo ratings yet
- Management of Lower-Extremity Venous Thromboembolism An Updated Review. April 2024.Document7 pagesManagement of Lower-Extremity Venous Thromboembolism An Updated Review. April 2024.myqrwd464kNo ratings yet
- Differentiated Thyroid Cancer: Presenter: DR Aakriti Athavale Moderated By: GP Capt (DR) PK SahuDocument43 pagesDifferentiated Thyroid Cancer: Presenter: DR Aakriti Athavale Moderated By: GP Capt (DR) PK SahuAakritiNo ratings yet
- VTEDocument45 pagesVTEABREHAM BUKULONo ratings yet
- Early Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskDocument4 pagesEarly Ambulation and Prevention of Post-Operative Thrombo-Embolic RiskAnderson LondoñoNo ratings yet
- Hospitalist Referring Physician PresentationDocument34 pagesHospitalist Referring Physician Presentationnorehan hassanNo ratings yet
- Treating Vte Today: Practice Your Skills: Literature ReviewDocument14 pagesTreating Vte Today: Practice Your Skills: Literature ReviewOanaNo ratings yet
- TKA CompliDocument53 pagesTKA CompliDr. Vishal singhNo ratings yet
- Anti Coagulation For Surgery GuidelineDocument3 pagesAnti Coagulation For Surgery GuidelineNur SusiawantyNo ratings yet
- Superficial Venous Thrombophlebitis: Presented by - Nader SaadDocument24 pagesSuperficial Venous Thrombophlebitis: Presented by - Nader SaadNader SaadNo ratings yet
- DVT Dr. BudiartoDocument36 pagesDVT Dr. Budiartoyori yarson tonNo ratings yet
- DVT and PEDocument56 pagesDVT and PEDefriyan RamziNo ratings yet
- Fondaparinux VTE (JCU 2018)Document54 pagesFondaparinux VTE (JCU 2018)sofiNo ratings yet
- CARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeDocument29 pagesCARDIAC CATHETERIZATION LABORATORY AN INTRODUCTORY MANUAL, University of TennesseeNavojit ChowdhuryNo ratings yet
- Care of The Post PICA (Stent)Document75 pagesCare of The Post PICA (Stent)benypermadiNo ratings yet
- Prevention of DVT/PE: Noornadia BT Yahaya 050100841Document32 pagesPrevention of DVT/PE: Noornadia BT Yahaya 050100841Nadia YahayaNo ratings yet
- Pulmonary Embolism & Deep Vein Thrombosis Definitions: Virchow's TriadDocument7 pagesPulmonary Embolism & Deep Vein Thrombosis Definitions: Virchow's TriadCitra Eva MeilyndhaNo ratings yet
- Case Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyDocument15 pagesCase Report - Deep Vein Thrombosis in Patient With Acute Heart Failure Due To Chemotherapy Induced CardiomyopathyAbdurrohman IzzuddinNo ratings yet
- Weledji 2020Document7 pagesWeledji 2020Felipe CarmonaNo ratings yet
- If HP Cancer Guide BMT ManualDocument363 pagesIf HP Cancer Guide BMT ManualZardar KNo ratings yet
- Day 4 - Presentasi VTE, Kuliah SM Okt 2012Document35 pagesDay 4 - Presentasi VTE, Kuliah SM Okt 2012Maha Satya Dwi PalgunaNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- AFP - Blok 3.4. IndoDocument36 pagesAFP - Blok 3.4. IndoadystiNo ratings yet
- Cutaneous Larval MigransDocument24 pagesCutaneous Larval MigransadystiNo ratings yet
- Erythrosquamous Diseases / Papulosquamous DiseasesDocument38 pagesErythrosquamous Diseases / Papulosquamous DiseasesadystiNo ratings yet
- Immunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityDocument35 pagesImmunization: Mei Neni S Pediatric Dept. Faculty of Medicine, Gadjah Mada UniversityadystiNo ratings yet
- Tropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaDocument95 pagesTropical and Infectious Subdivision of Internal Department Medical Faculty of Gadjah Mada University YogyakartaadystiNo ratings yet
- Venom (Insect Bite, Snake Bite, Dog Bite)Document23 pagesVenom (Insect Bite, Snake Bite, Dog Bite)adystiNo ratings yet
- Peripheral Arterial Occlusive DiseaseDocument43 pagesPeripheral Arterial Occlusive DiseaseadystiNo ratings yet
- Poisoning DecontaminationDocument14 pagesPoisoning DecontaminationadystiNo ratings yet
- Vaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionDocument26 pagesVaccine Preventable Diseases (VPDS) : Ida Safitri Laksono Dept of Child Health Infectious Disease Sub DivisionadystiNo ratings yet
- Oportunistic in ElderlyDocument19 pagesOportunistic in ElderlyadystiNo ratings yet
- Genito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaDocument78 pagesGenito Urinary Problems in Children: Bagian Ilmu Kesehatan Kulit & Kelamin Fakultas Kedokteran UGM YogyakartaadystiNo ratings yet
- Patient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentDocument27 pagesPatient Autonomy: Competent and Incompetent Patient and Research Participant To ConsentadystiNo ratings yet
- 1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesDocument67 pages1 Generation: Cefalexin Cefradin Cefadroxil Cefachlor Yes Yes Yes Yes YesadystiNo ratings yet
- Limb Salvage Edited DR PDDocument56 pagesLimb Salvage Edited DR PDadystiNo ratings yet
- Drug Abuse and OverdoseDocument31 pagesDrug Abuse and OverdoseadystiNo ratings yet
- Acute Gastric Mucosal LesionDocument19 pagesAcute Gastric Mucosal LesionadystiNo ratings yet
- Aging and Endocrine DisordersDocument23 pagesAging and Endocrine DisordersadystiNo ratings yet
- Role of Family and Social EnvironmentDocument19 pagesRole of Family and Social EnvironmentadystiNo ratings yet
- Differential Abdominal Pain - DR PututDocument28 pagesDifferential Abdominal Pain - DR PututadystiNo ratings yet
- Sexual Orientation and Sexual Disorders: DR Cecep Sugeng Kristanto, SP KJ (K)Document50 pagesSexual Orientation and Sexual Disorders: DR Cecep Sugeng Kristanto, SP KJ (K)adystiNo ratings yet
- Upper Gastrointestinal Pathology, Baru 2010Document59 pagesUpper Gastrointestinal Pathology, Baru 2010adystiNo ratings yet
- Ethics in Specific IssuesDocument11 pagesEthics in Specific IssuesadystiNo ratings yet
- Anxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDDocument38 pagesAnxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDadystiNo ratings yet
- Personality Disorder and Management Block 2.4: Carla R MarchiraDocument38 pagesPersonality Disorder and Management Block 2.4: Carla R MarchiraadystiNo ratings yet
- Adolescence Reproductive Health: Dicky Moch RizalDocument43 pagesAdolescence Reproductive Health: Dicky Moch RizaladystiNo ratings yet
- DERMATOTERAPIDocument55 pagesDERMATOTERAPIPutri Windiani Haryono HNo ratings yet
- Presentacion Imm5753eDocument1 pagePresentacion Imm5753eerev_20No ratings yet
- 3.6 Pharmaceutical Formulations (Theory)Document2 pages3.6 Pharmaceutical Formulations (Theory)rajeshNo ratings yet
- PROPOSAL PIT PAMKI LOMBOK 2023 NewDocument17 pagesPROPOSAL PIT PAMKI LOMBOK 2023 Newirgie pradiptaNo ratings yet
- A Case Report of Cesarian Section On A DoeDocument17 pagesA Case Report of Cesarian Section On A DoeAbdirazak AlkhaalidNo ratings yet
- TSRQ CompleteDocument10 pagesTSRQ CompletedrsheapherdNo ratings yet
- Disaster TriageDocument20 pagesDisaster TriageNabella100% (1)
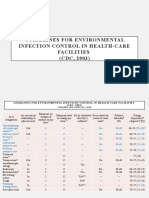
- CDC - Guidelines For Environmental Infection Control in Health-Care Facilities (CDC, 2003)Document9 pagesCDC - Guidelines For Environmental Infection Control in Health-Care Facilities (CDC, 2003)Kesehatan LingkunganNo ratings yet
- Final Adaptation Sick Young Infant Module PDFDocument76 pagesFinal Adaptation Sick Young Infant Module PDFAngelica AmandoNo ratings yet
- Nnamdi CV 2018 PDFDocument4 pagesNnamdi CV 2018 PDFUzonwanne Nnamdi OssaiNo ratings yet
- Elpido Ines Jr. MD, Mha Medical Director Elpido Ines Jr. MD, Mha Medical DirectorDocument3 pagesElpido Ines Jr. MD, Mha Medical Director Elpido Ines Jr. MD, Mha Medical Directorcriselda desistoNo ratings yet
- Asthma: DR Yusuf Adi Gunawan SPPDDocument19 pagesAsthma: DR Yusuf Adi Gunawan SPPDIan GalihNo ratings yet
- Nursing InformaticsDocument28 pagesNursing InformaticsAnusha Verghese100% (2)
- National Programme For Control of Blindness & Visual ImpairmentDocument15 pagesNational Programme For Control of Blindness & Visual ImpairmentSumon SarkarNo ratings yet
- Oakham Surgery New Patient FormDocument7 pagesOakham Surgery New Patient FormTrần Thanh ThảoNo ratings yet
- Diagnostics - Nursing ResponsibilitiesDocument9 pagesDiagnostics - Nursing ResponsibilitiesCarmellaDawn100% (3)
- Coping With Suicidal ThoughtsDocument7 pagesCoping With Suicidal Thoughtsmail4079No ratings yet
- Root Canal Treatment of Mandibular Canine With Two Root Canals: A Case Report SeriesDocument4 pagesRoot Canal Treatment of Mandibular Canine With Two Root Canals: A Case Report SeriesRifky Al ThariqNo ratings yet
- Alexandra Haluska ResumeDocument2 pagesAlexandra Haluska Resumeapi-546463844No ratings yet
- Nursing Induction PPT 2Document114 pagesNursing Induction PPT 2Mukesh Choudhary Jat100% (3)
- Enzalutamida arches-JCO.19.00799Document15 pagesEnzalutamida arches-JCO.19.00799Raul BarcellonaNo ratings yet
- Anatomy of The Genitourinary TractDocument5 pagesAnatomy of The Genitourinary TractQonitaaNo ratings yet
- Surgical Nursing Final PDFDocument26 pagesSurgical Nursing Final PDFAnuj Misra100% (2)
- Your Target CustomerDocument8 pagesYour Target CustomermishratrilokNo ratings yet
- ST - Clare'S Medical Center, Inc.: 1838 Dian Street, Makati City, Metro ManilaDocument1 pageST - Clare'S Medical Center, Inc.: 1838 Dian Street, Makati City, Metro ManilaKristine TaguiamNo ratings yet
- Payment in Healthcare OrganizationsDocument12 pagesPayment in Healthcare Organizationsevans kirimiNo ratings yet
- Laurel Barnett ResumeDocument2 pagesLaurel Barnett Resumeapi-554630786No ratings yet
- Permanent Contraception Method of Male (Vasectomy)Document20 pagesPermanent Contraception Method of Male (Vasectomy)Nilakshi Barik MandalNo ratings yet