Download as pptx, pdf, or txt
You might also like
- Incontinence 6th Edition 2017 Ebook v2-1 PDFDocument2,636 pagesIncontinence 6th Edition 2017 Ebook v2-1 PDFNoemí LópezNo ratings yet
- Motivation Letter Sample For Master in MedicineDocument2 pagesMotivation Letter Sample For Master in MedicineEdy Nacarapa100% (1)
- Obsgin - Obstetrics and GynecologyDocument12 pagesObsgin - Obstetrics and GynecologyLin ling BenawanNo ratings yet
- Introduction To ObstetricsDocument27 pagesIntroduction To ObstetricsDaniel NegeriNo ratings yet
- Theories of LabourDocument22 pagesTheories of LaboursubashikNo ratings yet
- Abnormalities of The Placenta OutlineDocument7 pagesAbnormalities of The Placenta OutlineSteve ShirmpNo ratings yet
- What Is RH Sensitization During PregnancyDocument14 pagesWhat Is RH Sensitization During PregnancyKeisha Ferreze Ann QuiñonesNo ratings yet
- Eclampsia OutputDocument5 pagesEclampsia OutputhailleyannNo ratings yet
- Close Chest Tube Insertion ThoracostomyDocument15 pagesClose Chest Tube Insertion ThoracostomyMae Navidas DigdiganNo ratings yet
- Physiology of Pregnancy 050918Document75 pagesPhysiology of Pregnancy 050918Anonymous 96LTCx100% (2)
- Case StudyDocument48 pagesCase Studysimbarashe tangwadzanaNo ratings yet
- MCN Lec Fetal DevpDocument580 pagesMCN Lec Fetal DevpknotstmNo ratings yet
- Hyperemesis GravidarumDocument19 pagesHyperemesis GravidarumMohnnad Hmood AlgaraybhNo ratings yet
- NonStress TestDocument2 pagesNonStress TestRama_ichiNo ratings yet
- Cardiovascular Disorders and PregnancyDocument13 pagesCardiovascular Disorders and PregnancyMaryela Maceda GalozoNo ratings yet
- Shoulder DystociaDocument63 pagesShoulder Dystociaapi-3841435100% (3)
- Case - Eclampsia FinalDocument84 pagesCase - Eclampsia FinalKimberley Anne Santos100% (1)
- Complications of MiscarriageDocument21 pagesComplications of MiscarriagebkbkjNo ratings yet
- What Is Retained PlacentaDocument7 pagesWhat Is Retained PlacentaA Xiao Yhing TrancoNo ratings yet
- TractionDocument11 pagesTractionDenalyn Ann TormoNo ratings yet
- Gestational Trophoblastic DiseaseDocument40 pagesGestational Trophoblastic DiseaseAayupta Mohanty100% (2)
- CP Ovarian Cyst Chap5Document11 pagesCP Ovarian Cyst Chap5Katherine 'Chingboo' Leonico LaudNo ratings yet
- ContraceptivesDocument8 pagesContraceptivesRadowan AhmadNo ratings yet
- Placenta PreviaDocument17 pagesPlacenta PreviaSundari AtmanegaraNo ratings yet
- Hyperemesis GravidarumDocument16 pagesHyperemesis GravidarumBabi PanggangNo ratings yet
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocument27 pagesIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancySelma FraNo ratings yet
- Case PresDocument100 pagesCase PresJoj BagnateNo ratings yet
- Uterine Myoma, Sept, 2021Document63 pagesUterine Myoma, Sept, 2021Kerod AbebeNo ratings yet
- Pathophysiology of Molar PregnancyDocument1 pagePathophysiology of Molar PregnancyFilipinas BelzaNo ratings yet
- Upper Respiratory Tract InfectionDocument12 pagesUpper Respiratory Tract InfectionErmie BalingitNo ratings yet
- RH Disease and ABO IncompatibilityDocument21 pagesRH Disease and ABO Incompatibilityjeezislove617No ratings yet
- Abortion and Ectopic PregnancyDocument3 pagesAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNo ratings yet
- Myoma Overview, Bibliography and ObjectivesDocument5 pagesMyoma Overview, Bibliography and ObjectivesicesexyNo ratings yet
- AnencephalyDocument10 pagesAnencephalyRm LavariasNo ratings yet
- Developing Theoretical and Conceptual Frameworks and Operational Definition of TermsDocument44 pagesDeveloping Theoretical and Conceptual Frameworks and Operational Definition of TermsHTCCS BatoCamSurNo ratings yet
- History Taking of A Pregnant WomanDocument3 pagesHistory Taking of A Pregnant WomanTemahlungwaneNo ratings yet
- Obstetric Nursing Care PlanDocument12 pagesObstetric Nursing Care PlanJass Mira Bueno100% (1)
- Mercer's Maternal Role Attainment TheoryDocument7 pagesMercer's Maternal Role Attainment TheoryFrances Joei O. PEREZNo ratings yet
- Breast AbscessDocument2 pagesBreast AbscessJoanna Agustin0% (1)
- Signs and Symptoms: Pregnancy Tonic-Clonic Seizures Pre-EclampsiaDocument6 pagesSigns and Symptoms: Pregnancy Tonic-Clonic Seizures Pre-Eclampsiafidc_04283646No ratings yet
- Obstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityDocument5 pagesObstetric Maneuvers For Shoulder Dystocia and Associated Fetal MorbidityBill HarmanNo ratings yet
- Ethical Theories: Prepared By: Regine Emerald B Dela Cruz RNDocument20 pagesEthical Theories: Prepared By: Regine Emerald B Dela Cruz RNRegine Dela CruzNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- DVT in PregDocument2 pagesDVT in Pregkhadzx100% (2)
- AMTSL BrieferDocument2 pagesAMTSL BrieferNewborn2013No ratings yet
- Ectopic Pregnancy - CSDocument14 pagesEctopic Pregnancy - CSMASII100% (1)
- Lecture Notes On AphDocument41 pagesLecture Notes On AphEyob MizanNo ratings yet
- Ectopic PregnancyDocument17 pagesEctopic Pregnancyapi-3700579No ratings yet
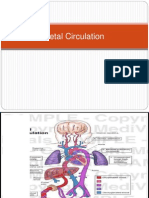
- Fetal CirculationDocument28 pagesFetal CirculationNelai GoNo ratings yet
- Health Teaching Plan For Newborn ScreeningDocument4 pagesHealth Teaching Plan For Newborn ScreeningPrincess Pauline AbrasaldoNo ratings yet
- PreeclampsiaDocument14 pagesPreeclampsiaHenny NovitasariNo ratings yet
- 6-Post-Term PregnancyDocument5 pages6-Post-Term PregnancyOmar MohammedNo ratings yet
- High Risk Pregnancy NewDocument16 pagesHigh Risk Pregnancy NewSurya SasidharanNo ratings yet
- Ectopic PregnancyDocument46 pagesEctopic PregnancyNoegi AkasNo ratings yet
- Cord ProlapseDocument22 pagesCord ProlapseJoyjet Evangelista-murilloNo ratings yet
- The High-Risk Pregnant Client:: NCM 109 Handout # 1Document3 pagesThe High-Risk Pregnant Client:: NCM 109 Handout # 1ApRil Anne BalanonNo ratings yet
- Hydatidiform MoleDocument10 pagesHydatidiform MoleLisa TurnerNo ratings yet
- Hypertension in Pregnancy CompiledDocument67 pagesHypertension in Pregnancy CompiledRaiza Love Caparas-PablicoNo ratings yet
- Placenta AcretaDocument118 pagesPlacenta AcretaPaco Vega WooNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Evo ProductDocument58 pagesEvo ProductMohammadfaroq HasanNo ratings yet
- Sweetly Mamuko Giving AdviceDocument6 pagesSweetly Mamuko Giving AdviceSweetly MamukoNo ratings yet
- Arnica and Aconite - Homeopathic Newborn CareDocument3 pagesArnica and Aconite - Homeopathic Newborn CarekhnumdumandfullofcumNo ratings yet
- 2024-06-24 Politics, Private Interests, and The Biden Administration's Deviation From Agency Regulations in The COVID-19 Pandemic (With Appendix)Document623 pages2024-06-24 Politics, Private Interests, and The Biden Administration's Deviation From Agency Regulations in The COVID-19 Pandemic (With Appendix)The FederalistNo ratings yet
- TB PolicyDocument174 pagesTB PolicyDrashua AshuaNo ratings yet
- Staff Nurse - PrintDocument8 pagesStaff Nurse - PrintMark Joseph Felicitas CuntapayNo ratings yet
- Summary of 2nd and 3rd Stages of LaborDocument2 pagesSummary of 2nd and 3rd Stages of LaborggggangNo ratings yet
- Kayleigh M Gifford Resume UpdatedDocument2 pagesKayleigh M Gifford Resume Updatedapi-498468880No ratings yet
- Naltrexone & Low-Dose NaltexoneDocument67 pagesNaltrexone & Low-Dose NaltexoneShi_DMS100% (1)
- Icmr SubmDocument2 pagesIcmr SubmShreya KhandelwalNo ratings yet
- Jurnal MataDocument7 pagesJurnal MatatrianaamaliaNo ratings yet
- (10920684 - Neurosurgical Focus) Factors Associated With Survival in Patients With MeningiomaDocument17 pages(10920684 - Neurosurgical Focus) Factors Associated With Survival in Patients With MeningiomaDarlene LebasteNo ratings yet
- Hydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaDocument80 pagesHydatidiform Mole: PGI Sia, Kevin PGI Tan, SheilaSheila Mary TanNo ratings yet
- STS ReportDocument10 pagesSTS ReportKay AbawagNo ratings yet
- White LabelDocument1 pageWhite LabelDee BelarminoNo ratings yet
- 2016 AJKD Volume 67 Issue 2 February (33) HepatorenalDocument11 pages2016 AJKD Volume 67 Issue 2 February (33) HepatorenalAnonymous Yo0mStNo ratings yet
- Acute Necrotizing PeriodontitisDocument4 pagesAcute Necrotizing PeriodontitisAzi Pertiwi HussainNo ratings yet
- 2021-08-16 MD Anderson RecordsDocument83 pages2021-08-16 MD Anderson RecordsjeffreybodinNo ratings yet
- CHCMGT005Document4 pagesCHCMGT005Pamela100% (1)
- QXR TB User GuideDocument12 pagesQXR TB User GuideBilly Omar Muñoz PeinadoNo ratings yet
- 300+ TOP CASE MANAGER Objective Questions and AnswersDocument29 pages300+ TOP CASE MANAGER Objective Questions and AnswersHANEESH JOHNNo ratings yet
- Resume Ebrahim RadinniaDocument2 pagesResume Ebrahim RadinniaSepideh MirzaeiNo ratings yet
- Rheumatoid Arthritis Diagnosed and TreatmentDocument3 pagesRheumatoid Arthritis Diagnosed and TreatmentHas SimNo ratings yet
- Artrite REATIVAsexualmente ADQUIRIDADocument10 pagesArtrite REATIVAsexualmente ADQUIRIDAYgor AlbuquerqueNo ratings yet
- Task 1: The Graph Illustrates The Amount of International Students Enrolment Who Come From and Study atDocument2 pagesTask 1: The Graph Illustrates The Amount of International Students Enrolment Who Come From and Study atĐặng Trần KhánhNo ratings yet
- RPS Podiatrist-Quick-Reference-Guide Updated 2021Document3 pagesRPS Podiatrist-Quick-Reference-Guide Updated 2021wa21No ratings yet
- Bibliografie TabelDocument4 pagesBibliografie Tabeldvcc8psv5tNo ratings yet
- Sicad QuestionnaireDocument19 pagesSicad QuestionnaireScribdTranslationsNo ratings yet