
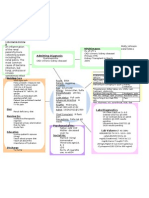
Ulcerative Colitis
Ulcerative Colitis
You might also like
- Course Plan M.SC 1 YearDocument64 pagesCourse Plan M.SC 1 YearSanthu Su89% (9)
- Unit Plan MSC Nursing 1st YearDocument19 pagesUnit Plan MSC Nursing 1st YearSanthu Su66% (29)
- Cellular and Molecular Immunology 7e Abbas TB ActivationDocument3 pagesCellular and Molecular Immunology 7e Abbas TB Activationmary100% (1)
- Course Plan M.SC 2 YearDocument93 pagesCourse Plan M.SC 2 YearSanthu Su80% (5)
- Project Proposal TitleDocument3 pagesProject Proposal TitleSlepy chngNo ratings yet
- Unit Plan MSC Nursing 2nd YearDocument12 pagesUnit Plan MSC Nursing 2nd YearSanthu Su100% (4)
- Occupational Health Lesson PlanDocument9 pagesOccupational Health Lesson PlanSanthu Su100% (5)
- Lesson Plan On Placenta PraeviaDocument14 pagesLesson Plan On Placenta PraeviaSanthu Su67% (6)
- CholecystitisDocument34 pagesCholecystitisapi-26762768100% (1)
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Anatomy and Physiology-LiverDocument2 pagesAnatomy and Physiology-Livermawel100% (1)
- NCP - Poststreptococcal GlomerulonephritisDocument12 pagesNCP - Poststreptococcal GlomerulonephritisAya BolinasNo ratings yet
- Anatomy and Physiology Related To Multiple Myelom1Document15 pagesAnatomy and Physiology Related To Multiple Myelom1Diane Kate Tobias Magno100% (1)
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- Appendicitis Nursing NotesDocument2 pagesAppendicitis Nursing NotesFreeNursingNotes33% (3)
- Case StudyDocument21 pagesCase StudyLuige AvilaNo ratings yet
- CKD PresentationDocument51 pagesCKD PresentationBasneyatPragyanNo ratings yet
- Concept Map PyelonephritisDocument1 pageConcept Map PyelonephritisMolly Hancey Johnson100% (2)
- Nursing Management: Unit Plan ON Unit - IDocument4 pagesNursing Management: Unit Plan ON Unit - ISanthu Su67% (3)
- BMLT TmuDocument50 pagesBMLT TmuSanthu SuNo ratings yet
- Lesson Plan ON ManagementDocument7 pagesLesson Plan ON ManagementSanthu Su100% (3)
- Hyperprolactinemia QuestionsDocument11 pagesHyperprolactinemia QuestionsJasmin Kae SistosoNo ratings yet
- Upper Gastrointestinal BleedingDocument24 pagesUpper Gastrointestinal BleedingDr.Sathaporn Kunnathum100% (1)
- Gastro Esophageal Reflux Disease (GERD)Document7 pagesGastro Esophageal Reflux Disease (GERD)MahaNo ratings yet
- Acute Renal FailureDocument17 pagesAcute Renal FailureDina Rasmita100% (1)
- Appendicitis (History & Examination)Document6 pagesAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- Hepatomegaly: Clinical ApproachDocument22 pagesHepatomegaly: Clinical ApproachPooja ShashidharanNo ratings yet
- Case Pres HydronephrosisDocument39 pagesCase Pres HydronephrosisLouie Dela Cruz100% (3)
- Dietary ManagementDocument26 pagesDietary ManagementGeofrey Maglalang100% (1)
- Peptic UlcerDocument5 pagesPeptic UlcerKomal KhanNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Electrolyte Imbalance 1Document3 pagesElectrolyte Imbalance 1Marius Clifford BilledoNo ratings yet
- Blunt Force Trauma-FinalDocument73 pagesBlunt Force Trauma-FinalHera Khaeyratul HisannNo ratings yet
- Case On ColitisDocument34 pagesCase On ColitisAamer SyedNo ratings yet
- NCP LymphomaDocument3 pagesNCP LymphomaJohn Emmanuel Tatad TudNo ratings yet
- CholelithiasisDocument37 pagesCholelithiasisbaby padzNo ratings yet
- PyelonephritisDocument59 pagesPyelonephritisGheyl GabrielNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- Case Study CholecystitisDocument27 pagesCase Study CholecystitisBandana RajpootNo ratings yet
- GI Bleeding - NursesDocument71 pagesGI Bleeding - Nursesapi-3760283100% (6)
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- Intestinal ObstructionDocument6 pagesIntestinal ObstructionCling Cruza0% (1)
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Upper Gastrointestinal BleedingDocument3 pagesUpper Gastrointestinal Bleedingplayaz_dan2100% (1)
- 3 Acute GastritisDocument2 pages3 Acute GastritisSuresh ThanneruNo ratings yet
- Peptic Ulcer DiseaseDocument6 pagesPeptic Ulcer DiseaseBheru LalNo ratings yet
- Liver AbscessDocument15 pagesLiver AbscessAli Aborges Jr.No ratings yet
- Cirrhosis of LiverDocument7 pagesCirrhosis of LivermOHAN.S100% (3)
- Appendicitis Case StudyDocument6 pagesAppendicitis Case StudyKimxi Chiu LimNo ratings yet
- GastritisDocument23 pagesGastritisLisnawati Nur Farida100% (1)
- PancreatitisDocument12 pagesPancreatitisjhodane100% (4)
- Summary Case Peptic Ulcer and PeritonitisDocument8 pagesSummary Case Peptic Ulcer and PeritonitissyududNo ratings yet
- Health Education - CholelithiasisDocument12 pagesHealth Education - Cholelithiasismohamad dildarNo ratings yet
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- Urolithiasis PowerpointDocument41 pagesUrolithiasis PowerpointPinkrose Chiong FabellaNo ratings yet
- Urinary RetentionDocument6 pagesUrinary Retentionjakenathanielvelasco50% (2)
- Case Study-Acute Urinary RetentionDocument10 pagesCase Study-Acute Urinary RetentionArthadian De Peralta75% (4)
- Asthma2 Case StudyDocument8 pagesAsthma2 Case StudyGlenn Asuncion PagaduanNo ratings yet
- 2 Acute CholecystitisDocument21 pages2 Acute CholecystitisEtteh MaryNo ratings yet
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionNurul Nurnita100% (1)
- Unstable AnginaDocument32 pagesUnstable AnginaMary Ann Lumbay Paye100% (2)
- CholelithiasisDocument5 pagesCholelithiasisrgflores1979100% (2)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abdominal Pain: James S Newman, M.D. The University of Texas Medical BranchDocument27 pagesAbdominal Pain: James S Newman, M.D. The University of Texas Medical BranchYudiese YouNo ratings yet
- Chronic Bowel Disease and SepsisDocument52 pagesChronic Bowel Disease and SepsisOlga Goryacheva100% (1)
- UntitledDocument69 pagesUntitledRao ImtisalNo ratings yet
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Management of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANDocument101 pagesManagement of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANMichael Baylon DueñasNo ratings yet
- Diverticulitis DiseaseDocument35 pagesDiverticulitis DiseaseYzobel Phoebe ParoanNo ratings yet
- Community Health Nursing: Unit Plan ON Unit - ViDocument5 pagesCommunity Health Nursing: Unit Plan ON Unit - ViSanthu Su100% (1)
- M.SC 2nd Year Obg Clinical Rotation PlanDocument1 pageM.SC 2nd Year Obg Clinical Rotation PlanSanthu Su67% (3)
- PHCDocument6 pagesPHCSanthu Su75% (4)
- RNTCPDocument7 pagesRNTCPSanthu Su100% (2)
- Lesson Plan ON PlanningDocument7 pagesLesson Plan ON PlanningSanthu SuNo ratings yet
- RCHDocument5 pagesRCHSanthu Su83% (6)
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Nurse Practioner Syllabus RegulationsDocument69 pagesNurse Practioner Syllabus RegulationsSanthu SuNo ratings yet
- Pancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemDocument5 pagesPancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemSanthu Su100% (2)
- Lesson Plan On Genital ProlapseDocument12 pagesLesson Plan On Genital ProlapseSanthu Su67% (3)
- Guidelines For GNM PDFDocument133 pagesGuidelines For GNM PDFJeeshanKhanNo ratings yet
- Storage of Medication (Fire Proof, Boxes Recommended) - Medications Are Stored in A Clean, Safe and Secure Environment (Recommended)Document2 pagesStorage of Medication (Fire Proof, Boxes Recommended) - Medications Are Stored in A Clean, Safe and Secure Environment (Recommended)Santhu SuNo ratings yet
- Unit III PlanningDocument60 pagesUnit III PlanningSanthu SuNo ratings yet
- Appendicitis Def - It Is An Inflammation of The AppendixDocument9 pagesAppendicitis Def - It Is An Inflammation of The AppendixSanthu SuNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- Notes Liver CirrhosisDocument10 pagesNotes Liver CirrhosisSanthu Su100% (1)
- Notes HemorrhoidsDocument4 pagesNotes HemorrhoidsSanthu Su100% (1)
- Nursing Hospital Staff Job Description AimsDocument20 pagesNursing Hospital Staff Job Description AimsSanthu Su100% (1)
- Oral Path CramDocument10 pagesOral Path CramHarjotBrarNo ratings yet
- Neamtu Marius Cristian RJME 58 3 2017Document5 pagesNeamtu Marius Cristian RJME 58 3 2017Boldeanu MVNo ratings yet
- Dysmenorrhea Definition PDFDocument14 pagesDysmenorrhea Definition PDFYogi HermawanNo ratings yet
- Eur J Echocardiogr 2010 Walker E37Document4 pagesEur J Echocardiogr 2010 Walker E37Muhammad Haryadi AdeNo ratings yet
- Surgical Diseases 1Document8 pagesSurgical Diseases 1Shubham TanwarNo ratings yet
- Goal No. Philippines Health Agenda Goals What If This Goal Is Achieved? What If This Goal Is Not Achieved? 1Document2 pagesGoal No. Philippines Health Agenda Goals What If This Goal Is Achieved? What If This Goal Is Not Achieved? 1Hiro LeeNo ratings yet
- Mallory Brearey-Resume 2021 1Document2 pagesMallory Brearey-Resume 2021 1api-507675724No ratings yet
- Acute Kidney Injury in Children: Being AWAREDocument4 pagesAcute Kidney Injury in Children: Being AWAREIrkania PasangkaNo ratings yet
- Thalidomide: Moderator: DR Swapna Jena (Asso. Professor)Document48 pagesThalidomide: Moderator: DR Swapna Jena (Asso. Professor)Siddharth DashNo ratings yet
- Part 2 First AidDocument11 pagesPart 2 First AidHana SeiadiNo ratings yet
- Complete Health HistoryDocument6 pagesComplete Health HistoryAIKA BAYANo ratings yet
- Catheters, Tubes, and Drains in The Pediatric ChestDocument60 pagesCatheters, Tubes, and Drains in The Pediatric ChestManuel PoncianNo ratings yet
- Immunohematology Harmening HIGHLIGHT 2222Document45 pagesImmunohematology Harmening HIGHLIGHT 2222flynnpunzNo ratings yet
- Gastrointestinal Operations and Technical Variations: Michael Korenkov Christoph-Thomas Germer Hauke LangDocument417 pagesGastrointestinal Operations and Technical Variations: Michael Korenkov Christoph-Thomas Germer Hauke LangBogdan Trandafir100% (2)
- TFCBT Training GuidelinesDocument3 pagesTFCBT Training GuidelinespolNo ratings yet
- AspergerDocument7 pagesAspergerapi-508605014No ratings yet
- Abses Hepar: Erina Angelia Perceptor: DR - Lukas.,Sp - PDDocument12 pagesAbses Hepar: Erina Angelia Perceptor: DR - Lukas.,Sp - PDSimon Messi SiringoringoNo ratings yet
- Mtap-Semr1-Week 2-Diabetes and Glucose MonitoringDocument9 pagesMtap-Semr1-Week 2-Diabetes and Glucose MonitoringJessoliver GalvezNo ratings yet
- Ventilators Zisline - MV200, MV300Document7 pagesVentilators Zisline - MV200, MV300d.kostrov15mtNo ratings yet
- Daftar Pustaka RibsDocument3 pagesDaftar Pustaka RibsRibka SimbolonNo ratings yet
- Classroom Daily Health Monitoring Tool For CovidDocument4 pagesClassroom Daily Health Monitoring Tool For CovidGenie Sina-on DadeaNo ratings yet
- Maternal & Child Health CareDocument51 pagesMaternal & Child Health CareBhumi ChouhanNo ratings yet
- DRUG STUDY and CASE ANALYSISDocument6 pagesDRUG STUDY and CASE ANALYSISMa. Kaile Shyla LlacarNo ratings yet
- SNAPPE-II Score For Neonatal Acute Physiology WithDocument3 pagesSNAPPE-II Score For Neonatal Acute Physiology WithwennyNo ratings yet
- Cancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORDocument7 pagesCancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORvk_204veticoNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- Ophthalmology Set 7Document5 pagesOphthalmology Set 7ajay khadeNo ratings yet



















































































































Download as pptx, pdf, or txt
You might also like
- Course Plan M.SC 1 YearDocument64 pagesCourse Plan M.SC 1 YearSanthu Su89% (9)
- Unit Plan MSC Nursing 1st YearDocument19 pagesUnit Plan MSC Nursing 1st YearSanthu Su66% (29)
- Cellular and Molecular Immunology 7e Abbas TB ActivationDocument3 pagesCellular and Molecular Immunology 7e Abbas TB Activationmary100% (1)
- Course Plan M.SC 2 YearDocument93 pagesCourse Plan M.SC 2 YearSanthu Su80% (5)
- Project Proposal TitleDocument3 pagesProject Proposal TitleSlepy chngNo ratings yet
- Unit Plan MSC Nursing 2nd YearDocument12 pagesUnit Plan MSC Nursing 2nd YearSanthu Su100% (4)
- Occupational Health Lesson PlanDocument9 pagesOccupational Health Lesson PlanSanthu Su100% (5)
- Lesson Plan On Placenta PraeviaDocument14 pagesLesson Plan On Placenta PraeviaSanthu Su67% (6)
- CholecystitisDocument34 pagesCholecystitisapi-26762768100% (1)
- Syndrome of Inappropriate Secretion of Anti Diuretic HormoneDocument39 pagesSyndrome of Inappropriate Secretion of Anti Diuretic Hormonefarmasi_hmNo ratings yet
- Anatomy and Physiology-LiverDocument2 pagesAnatomy and Physiology-Livermawel100% (1)
- NCP - Poststreptococcal GlomerulonephritisDocument12 pagesNCP - Poststreptococcal GlomerulonephritisAya BolinasNo ratings yet
- Anatomy and Physiology Related To Multiple Myelom1Document15 pagesAnatomy and Physiology Related To Multiple Myelom1Diane Kate Tobias Magno100% (1)
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Nursing Process of PneumoniaDocument5 pagesNursing Process of Pneumoniatin2x061275% (8)
- Appendicitis Nursing NotesDocument2 pagesAppendicitis Nursing NotesFreeNursingNotes33% (3)
- Case StudyDocument21 pagesCase StudyLuige AvilaNo ratings yet
- CKD PresentationDocument51 pagesCKD PresentationBasneyatPragyanNo ratings yet
- Concept Map PyelonephritisDocument1 pageConcept Map PyelonephritisMolly Hancey Johnson100% (2)
- Nursing Management: Unit Plan ON Unit - IDocument4 pagesNursing Management: Unit Plan ON Unit - ISanthu Su67% (3)
- BMLT TmuDocument50 pagesBMLT TmuSanthu SuNo ratings yet
- Lesson Plan ON ManagementDocument7 pagesLesson Plan ON ManagementSanthu Su100% (3)
- Hyperprolactinemia QuestionsDocument11 pagesHyperprolactinemia QuestionsJasmin Kae SistosoNo ratings yet
- Upper Gastrointestinal BleedingDocument24 pagesUpper Gastrointestinal BleedingDr.Sathaporn Kunnathum100% (1)
- Gastro Esophageal Reflux Disease (GERD)Document7 pagesGastro Esophageal Reflux Disease (GERD)MahaNo ratings yet
- Acute Renal FailureDocument17 pagesAcute Renal FailureDina Rasmita100% (1)
- Appendicitis (History & Examination)Document6 pagesAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- Hepatomegaly: Clinical ApproachDocument22 pagesHepatomegaly: Clinical ApproachPooja ShashidharanNo ratings yet
- Case Pres HydronephrosisDocument39 pagesCase Pres HydronephrosisLouie Dela Cruz100% (3)
- Dietary ManagementDocument26 pagesDietary ManagementGeofrey Maglalang100% (1)
- Peptic UlcerDocument5 pagesPeptic UlcerKomal KhanNo ratings yet
- Activity IntoleranceDocument6 pagesActivity IntoleranceRaidis PangilinanNo ratings yet
- Acute PancreatitisDocument7 pagesAcute PancreatitisVytheeshwaran Vedagiri100% (9)
- Electrolyte Imbalance 1Document3 pagesElectrolyte Imbalance 1Marius Clifford BilledoNo ratings yet
- Blunt Force Trauma-FinalDocument73 pagesBlunt Force Trauma-FinalHera Khaeyratul HisannNo ratings yet
- Case On ColitisDocument34 pagesCase On ColitisAamer SyedNo ratings yet
- NCP LymphomaDocument3 pagesNCP LymphomaJohn Emmanuel Tatad TudNo ratings yet
- CholelithiasisDocument37 pagesCholelithiasisbaby padzNo ratings yet
- PyelonephritisDocument59 pagesPyelonephritisGheyl GabrielNo ratings yet
- Diverticular DiseaseDocument8 pagesDiverticular Diseasenurse_enzo100% (1)
- Case Study CholecystitisDocument27 pagesCase Study CholecystitisBandana RajpootNo ratings yet
- GI Bleeding - NursesDocument71 pagesGI Bleeding - Nursesapi-3760283100% (6)
- PEPTIC ULCER DISEASE 2018 EdittedDocument43 pagesPEPTIC ULCER DISEASE 2018 EdittedJumbe MohamedNo ratings yet
- Intestinal ObstructionDocument6 pagesIntestinal ObstructionCling Cruza0% (1)
- Chronic Liver DiseaseDocument12 pagesChronic Liver DiseaseamitNo ratings yet
- Upper Gastrointestinal BleedingDocument3 pagesUpper Gastrointestinal Bleedingplayaz_dan2100% (1)
- 3 Acute GastritisDocument2 pages3 Acute GastritisSuresh ThanneruNo ratings yet
- Peptic Ulcer DiseaseDocument6 pagesPeptic Ulcer DiseaseBheru LalNo ratings yet
- Liver AbscessDocument15 pagesLiver AbscessAli Aborges Jr.No ratings yet
- Cirrhosis of LiverDocument7 pagesCirrhosis of LivermOHAN.S100% (3)
- Appendicitis Case StudyDocument6 pagesAppendicitis Case StudyKimxi Chiu LimNo ratings yet
- GastritisDocument23 pagesGastritisLisnawati Nur Farida100% (1)
- PancreatitisDocument12 pagesPancreatitisjhodane100% (4)
- Summary Case Peptic Ulcer and PeritonitisDocument8 pagesSummary Case Peptic Ulcer and PeritonitissyududNo ratings yet
- Health Education - CholelithiasisDocument12 pagesHealth Education - Cholelithiasismohamad dildarNo ratings yet
- HemorrhoidectomyDocument5 pagesHemorrhoidectomydrnareshkumar3281100% (1)
- Urolithiasis PowerpointDocument41 pagesUrolithiasis PowerpointPinkrose Chiong FabellaNo ratings yet
- Urinary RetentionDocument6 pagesUrinary Retentionjakenathanielvelasco50% (2)
- Case Study-Acute Urinary RetentionDocument10 pagesCase Study-Acute Urinary RetentionArthadian De Peralta75% (4)
- Asthma2 Case StudyDocument8 pagesAsthma2 Case StudyGlenn Asuncion PagaduanNo ratings yet
- 2 Acute CholecystitisDocument21 pages2 Acute CholecystitisEtteh MaryNo ratings yet
- Intestinal ObstructionDocument12 pagesIntestinal ObstructionNurul Nurnita100% (1)
- Unstable AnginaDocument32 pagesUnstable AnginaMary Ann Lumbay Paye100% (2)
- CholelithiasisDocument5 pagesCholelithiasisrgflores1979100% (2)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abdominal Pain: James S Newman, M.D. The University of Texas Medical BranchDocument27 pagesAbdominal Pain: James S Newman, M.D. The University of Texas Medical BranchYudiese YouNo ratings yet
- Chronic Bowel Disease and SepsisDocument52 pagesChronic Bowel Disease and SepsisOlga Goryacheva100% (1)
- UntitledDocument69 pagesUntitledRao ImtisalNo ratings yet
- PERITONITISDocument12 pagesPERITONITISHayat AL AKOUM100% (1)
- Management of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANDocument101 pagesManagement of Clients With Intestinal Disorders: - Michael D. Manglapus, BSN-RN, RM, MANMichael Baylon DueñasNo ratings yet
- Diverticulitis DiseaseDocument35 pagesDiverticulitis DiseaseYzobel Phoebe ParoanNo ratings yet
- Community Health Nursing: Unit Plan ON Unit - ViDocument5 pagesCommunity Health Nursing: Unit Plan ON Unit - ViSanthu Su100% (1)
- M.SC 2nd Year Obg Clinical Rotation PlanDocument1 pageM.SC 2nd Year Obg Clinical Rotation PlanSanthu Su67% (3)
- PHCDocument6 pagesPHCSanthu Su75% (4)
- RNTCPDocument7 pagesRNTCPSanthu Su100% (2)
- Lesson Plan ON PlanningDocument7 pagesLesson Plan ON PlanningSanthu SuNo ratings yet
- RCHDocument5 pagesRCHSanthu Su83% (6)
- LESSON PLAN Shwe Final PmsDocument14 pagesLESSON PLAN Shwe Final PmsSanthu Su100% (1)
- Nurse Practioner Syllabus RegulationsDocument69 pagesNurse Practioner Syllabus RegulationsSanthu SuNo ratings yet
- Pancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemDocument5 pagesPancreatitis: Def Pancreatitis (Inflammation of The Pancreas) Is A Serious Disorder. The Most Basic Classification SystemSanthu Su100% (2)
- Lesson Plan On Genital ProlapseDocument12 pagesLesson Plan On Genital ProlapseSanthu Su67% (3)
- Guidelines For GNM PDFDocument133 pagesGuidelines For GNM PDFJeeshanKhanNo ratings yet
- Storage of Medication (Fire Proof, Boxes Recommended) - Medications Are Stored in A Clean, Safe and Secure Environment (Recommended)Document2 pagesStorage of Medication (Fire Proof, Boxes Recommended) - Medications Are Stored in A Clean, Safe and Secure Environment (Recommended)Santhu SuNo ratings yet
- Unit III PlanningDocument60 pagesUnit III PlanningSanthu SuNo ratings yet
- Appendicitis Def - It Is An Inflammation of The AppendixDocument9 pagesAppendicitis Def - It Is An Inflammation of The AppendixSanthu SuNo ratings yet
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuNo ratings yet
- Notes Liver CirrhosisDocument10 pagesNotes Liver CirrhosisSanthu Su100% (1)
- Notes HemorrhoidsDocument4 pagesNotes HemorrhoidsSanthu Su100% (1)
- Nursing Hospital Staff Job Description AimsDocument20 pagesNursing Hospital Staff Job Description AimsSanthu Su100% (1)
- Oral Path CramDocument10 pagesOral Path CramHarjotBrarNo ratings yet
- Neamtu Marius Cristian RJME 58 3 2017Document5 pagesNeamtu Marius Cristian RJME 58 3 2017Boldeanu MVNo ratings yet
- Dysmenorrhea Definition PDFDocument14 pagesDysmenorrhea Definition PDFYogi HermawanNo ratings yet
- Eur J Echocardiogr 2010 Walker E37Document4 pagesEur J Echocardiogr 2010 Walker E37Muhammad Haryadi AdeNo ratings yet
- Surgical Diseases 1Document8 pagesSurgical Diseases 1Shubham TanwarNo ratings yet
- Goal No. Philippines Health Agenda Goals What If This Goal Is Achieved? What If This Goal Is Not Achieved? 1Document2 pagesGoal No. Philippines Health Agenda Goals What If This Goal Is Achieved? What If This Goal Is Not Achieved? 1Hiro LeeNo ratings yet
- Mallory Brearey-Resume 2021 1Document2 pagesMallory Brearey-Resume 2021 1api-507675724No ratings yet
- Acute Kidney Injury in Children: Being AWAREDocument4 pagesAcute Kidney Injury in Children: Being AWAREIrkania PasangkaNo ratings yet
- Thalidomide: Moderator: DR Swapna Jena (Asso. Professor)Document48 pagesThalidomide: Moderator: DR Swapna Jena (Asso. Professor)Siddharth DashNo ratings yet
- Part 2 First AidDocument11 pagesPart 2 First AidHana SeiadiNo ratings yet
- Complete Health HistoryDocument6 pagesComplete Health HistoryAIKA BAYANo ratings yet
- Catheters, Tubes, and Drains in The Pediatric ChestDocument60 pagesCatheters, Tubes, and Drains in The Pediatric ChestManuel PoncianNo ratings yet
- Immunohematology Harmening HIGHLIGHT 2222Document45 pagesImmunohematology Harmening HIGHLIGHT 2222flynnpunzNo ratings yet
- Gastrointestinal Operations and Technical Variations: Michael Korenkov Christoph-Thomas Germer Hauke LangDocument417 pagesGastrointestinal Operations and Technical Variations: Michael Korenkov Christoph-Thomas Germer Hauke LangBogdan Trandafir100% (2)
- TFCBT Training GuidelinesDocument3 pagesTFCBT Training GuidelinespolNo ratings yet
- AspergerDocument7 pagesAspergerapi-508605014No ratings yet
- Abses Hepar: Erina Angelia Perceptor: DR - Lukas.,Sp - PDDocument12 pagesAbses Hepar: Erina Angelia Perceptor: DR - Lukas.,Sp - PDSimon Messi SiringoringoNo ratings yet
- Mtap-Semr1-Week 2-Diabetes and Glucose MonitoringDocument9 pagesMtap-Semr1-Week 2-Diabetes and Glucose MonitoringJessoliver GalvezNo ratings yet
- Ventilators Zisline - MV200, MV300Document7 pagesVentilators Zisline - MV200, MV300d.kostrov15mtNo ratings yet
- Daftar Pustaka RibsDocument3 pagesDaftar Pustaka RibsRibka SimbolonNo ratings yet
- Classroom Daily Health Monitoring Tool For CovidDocument4 pagesClassroom Daily Health Monitoring Tool For CovidGenie Sina-on DadeaNo ratings yet
- Maternal & Child Health CareDocument51 pagesMaternal & Child Health CareBhumi ChouhanNo ratings yet
- DRUG STUDY and CASE ANALYSISDocument6 pagesDRUG STUDY and CASE ANALYSISMa. Kaile Shyla LlacarNo ratings yet
- SNAPPE-II Score For Neonatal Acute Physiology WithDocument3 pagesSNAPPE-II Score For Neonatal Acute Physiology WithwennyNo ratings yet
- Cancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORDocument7 pagesCancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORvk_204veticoNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- Ophthalmology Set 7Document5 pagesOphthalmology Set 7ajay khadeNo ratings yet