Download as ppt, pdf, or txt
You might also like
- 2k Duolingo PlusDocument158 pages2k Duolingo PlusThomas De Doncker0% (1)
- VZ-30 Service ManualDocument32 pagesVZ-30 Service ManualJimmy Mayta100% (1)
- 2 - Survivor Personality QuizDocument2 pages2 - Survivor Personality Quizdevin mahendikaNo ratings yet
- The Cadbury Code of Best Practices Had 19 RecommendationsDocument2 pagesThe Cadbury Code of Best Practices Had 19 RecommendationsAnam Shoaib82% (11)
- LiverDocument177 pagesLiverChiiraq EugeneNo ratings yet
- 10 StomachDocument10 pages10 StomachApabrita KarmakarNo ratings yet
- Gis 1 EnglishDocument85 pagesGis 1 Englishexand861No ratings yet
- Small Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerDocument32 pagesSmall Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerMia DangaNo ratings yet
- Stomach Neoplasms: Professor Ravi KantDocument75 pagesStomach Neoplasms: Professor Ravi KantcoksiNo ratings yet
- 20.MBBS Pancreatic CancerDocument52 pages20.MBBS Pancreatic Cancermrajah95No ratings yet
- Hepatocellular CarcinomaDocument62 pagesHepatocellular CarcinomaWilliams Emmanuel AdeyeyeNo ratings yet
- Lower Gi Finals 2019Document51 pagesLower Gi Finals 2019Spring BlossomNo ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantDaniel Alfredo Tenorio GonzálezNo ratings yet
- Sajid SurgeryDocument42 pagesSajid SurgerySajidNo ratings yet
- Role of Radiotherapy For Hepatocellular CarcinomaDocument37 pagesRole of Radiotherapy For Hepatocellular CarcinomabahtiarhabibiNo ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantVasanth MalagiNo ratings yet
- Gastric CarcinomaDocument43 pagesGastric CarcinomaPragadeswaran SNo ratings yet
- Colorectal Cancer: - Dr. Suneet KhuranaDocument36 pagesColorectal Cancer: - Dr. Suneet KhuranaCarlo ToledooNo ratings yet
- CRC and Other Colorectal Disease - PPT For Senior Medical StudentsDocument37 pagesCRC and Other Colorectal Disease - PPT For Senior Medical StudentsGiovanni HenryNo ratings yet
- HEPATOMADocument30 pagesHEPATOMASemestaNo ratings yet
- Pancreatic Cancer MedscapeDocument44 pagesPancreatic Cancer MedscapePati MuresanNo ratings yet
- Pancreatic CancerDocument25 pagesPancreatic CancerAatir JavaidNo ratings yet
- Pancreatic CancerDocument4 pagesPancreatic Cancersdf100% (1)
- Gastric cancer: Zhi Hua Ran (冉志华)Document67 pagesGastric cancer: Zhi Hua Ran (冉志华)Cahaya Al-HazeenillahNo ratings yet
- Benign Liver Tumours EASL CPG Slide DeckDocument28 pagesBenign Liver Tumours EASL CPG Slide DeckdianaNo ratings yet
- Pancreas: DR Sigid Djuniawan, SPBDocument40 pagesPancreas: DR Sigid Djuniawan, SPBditaayupNo ratings yet
- Neoplasma of PankreasDocument33 pagesNeoplasma of PankreasGina Sonia RahmahNo ratings yet
- Surg 2 JaundicedDocument94 pagesSurg 2 Jaundicedapi-3728522No ratings yet
- Initial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsDocument33 pagesInitial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsClaudia YalanNo ratings yet
- Gastric Cancer: Done By: Mustafa Khalil Ibrahim Tbilisi State Medical University 4 Year, 1 Semester, 2 GroupDocument51 pagesGastric Cancer: Done By: Mustafa Khalil Ibrahim Tbilisi State Medical University 4 Year, 1 Semester, 2 Groupjordhy kaseNo ratings yet
- Gastric Cancer: Done By: Mustafa Khalil Ibrahim Tbilisi State Medical University 4 Year, 1 Semester, 2 GroupDocument51 pagesGastric Cancer: Done By: Mustafa Khalil Ibrahim Tbilisi State Medical University 4 Year, 1 Semester, 2 GroupD.A.B.M100% (1)
- Carcinoid Tumor: Marcelyn Coley Surgery IV Conference Mount Sinai School of MedicineDocument52 pagesCarcinoid Tumor: Marcelyn Coley Surgery IV Conference Mount Sinai School of Medicinedrqazi777No ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Gastric CancerDocument65 pagesGastric Canceranandtmc100% (1)
- Colorectal Cancer Colon Cancer/ Rectal Cancer: Linked To High-Fat DietDocument1 pageColorectal Cancer Colon Cancer/ Rectal Cancer: Linked To High-Fat DietIrish Eunice FelixNo ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document25 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonDocument65 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonEslam R. Almassri100% (1)
- Biliary Tumors: Cholangiocarcinoma and Cancer of The Gall BladderDocument34 pagesBiliary Tumors: Cholangiocarcinoma and Cancer of The Gall BladderBoneyJalgarNo ratings yet
- LIVER SlidesDocument144 pagesLIVER SlidesChiiraq EugeneNo ratings yet
- Inoperable Stomch CaDocument31 pagesInoperable Stomch Cadamera_vineetNo ratings yet
- Dr. Pankaj Tejasvi: Dept. of Surgery MGMMC & MYH IndoreDocument76 pagesDr. Pankaj Tejasvi: Dept. of Surgery MGMMC & MYH IndoreDang HungNo ratings yet
- Referat CA PancreasDocument25 pagesReferat CA PancreasPamela VasikhaNo ratings yet
- Cervical CancerDocument22 pagesCervical CancerfrankNo ratings yet
- Management Gastric CancerDocument76 pagesManagement Gastric Cancerwawan siswokoNo ratings yet
- 4 Esophagus 2018Document55 pages4 Esophagus 2018a20-0353-958No ratings yet
- Hepatocellular Carcinoma: Dr. Isbandiyah, SPPDDocument26 pagesHepatocellular Carcinoma: Dr. Isbandiyah, SPPDMeta ShofiaNo ratings yet
- Gastriccancer 160428190410Document54 pagesGastriccancer 160428190410Pranavi ShewaleNo ratings yet
- Gall Bladder CarcinomaDocument29 pagesGall Bladder CarcinomaUsman FarooqNo ratings yet
- Practice Essentials: Essential Update: Pancreatoduodenectomy May Be Done Without Biopsy Proof in Select CasesDocument3 pagesPractice Essentials: Essential Update: Pancreatoduodenectomy May Be Done Without Biopsy Proof in Select CasesSheila AnisaNo ratings yet
- Pancreatic Nursing Oncologic NursingDocument15 pagesPancreatic Nursing Oncologic NursingMari ManlapazNo ratings yet
- Gastric Carcinoma: Professor Ravi KantDocument44 pagesGastric Carcinoma: Professor Ravi KantAna Quintana100% (1)
- Colorectal CancerDocument6 pagesColorectal CancerAshiniNo ratings yet
- Capancreas 160907124326Document34 pagesCapancreas 160907124326Ahlam Azam, MohamedNo ratings yet
- Pancreatic Cancer: Pathophysiologic EtiologyDocument2 pagesPancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNo ratings yet
- Common Gastrointesti NAL Malignancies: Kristine Flor D. Renomeron Group 2 Schwartz ClubDocument56 pagesCommon Gastrointesti NAL Malignancies: Kristine Flor D. Renomeron Group 2 Schwartz ClubEC BaldzNo ratings yet
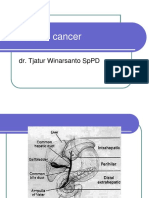
- Pancreatic Cancer: Dr. Tjatur Winarsanto SPPDDocument41 pagesPancreatic Cancer: Dr. Tjatur Winarsanto SPPDMayiz Renata LimerseNo ratings yet
- PancreatitisDocument51 pagesPancreatitisMizrab NadeemNo ratings yet
- Liver CancerDocument44 pagesLiver CancerJoyce Ann CumlatNo ratings yet
- 1-2022 Gastric CancerDocument95 pages1-2022 Gastric CancerAli Murtaza AbbasNo ratings yet
- Tumours of The Pancreas: Dr. Saleh M. Al SalamahDocument33 pagesTumours of The Pancreas: Dr. Saleh M. Al SalamahAdil ShabbirNo ratings yet
- Tumors of Pancreas DR DilberDocument51 pagesTumors of Pancreas DR Dilberdrdilber100% (2)
- Pancreaticcancer 150917114601 Lva1 App6891Document30 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- SurgeryDocument41 pagesSurgerysparkleNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- New Horizons in Appetite and The Anorexia of AgeingDocument9 pagesNew Horizons in Appetite and The Anorexia of Ageingdevin mahendikaNo ratings yet
- Cancer Treatment and Research Communications: Timotius Ivan Hariyanto, Andree KurniawanDocument10 pagesCancer Treatment and Research Communications: Timotius Ivan Hariyanto, Andree Kurniawandevin mahendikaNo ratings yet
- Night Sweats: A Systematic Review of The LiteratureDocument16 pagesNight Sweats: A Systematic Review of The Literaturedevin mahendikaNo ratings yet
- Weight Loss As A Predictor of Cancer in Primary Care A Systemati 2018Document12 pagesWeight Loss As A Predictor of Cancer in Primary Care A Systemati 2018devin mahendikaNo ratings yet
- Pathophysiology of Anorexia in The Cancer Cachexia Syndrome: Chukwuemeka Charles Ezeoke & John E. MorleyDocument16 pagesPathophysiology of Anorexia in The Cancer Cachexia Syndrome: Chukwuemeka Charles Ezeoke & John E. Morleydevin mahendikaNo ratings yet
- The Clinical Importance of Vitamin D (Cholecalciferol) : A Paradigm Shift With Implications For All Healthcare ProvidersDocument82 pagesThe Clinical Importance of Vitamin D (Cholecalciferol) : A Paradigm Shift With Implications For All Healthcare Providersdevin mahendikaNo ratings yet
- In Words: Satu Juta Delapan Ratus Ribu Delapan Ratus Lima Puluh DelapanDocument2 pagesIn Words: Satu Juta Delapan Ratus Ribu Delapan Ratus Lima Puluh Delapandevin mahendikaNo ratings yet
- Nurse Education Today: Contents Lists Available atDocument6 pagesNurse Education Today: Contents Lists Available atdevin mahendikaNo ratings yet
- (APCMS2020) Abstract Results - (ENG - PPHotel) - 2Document1 page(APCMS2020) Abstract Results - (ENG - PPHotel) - 2devin mahendikaNo ratings yet
- New Microsoft Word DocumentDocument1 pageNew Microsoft Word Documentdevin mahendikaNo ratings yet
- E CalenderDocument6 pagesE Calenderdevin mahendikaNo ratings yet
- New Microsoft Word DocumentDocument1 pageNew Microsoft Word Documentdevin mahendikaNo ratings yet
- British Deputy High Commission in KarachiDocument1 pageBritish Deputy High Commission in KarachiRaza WazirNo ratings yet
- At The AirportDocument6 pagesAt The AirportAlen KuharićNo ratings yet
- Of The Abdominal Wall, Abdominal Organs, Vasculature, Spinal Nerves and DermatomesDocument11 pagesOf The Abdominal Wall, Abdominal Organs, Vasculature, Spinal Nerves and DermatomesentistdeNo ratings yet
- Wallenberg's BlizzBaller - Diablo 2 at Diablo2Document9 pagesWallenberg's BlizzBaller - Diablo 2 at Diablo2kuntokinteNo ratings yet
- Builder - PDF (China Substitution)Document11 pagesBuilder - PDF (China Substitution)Finsen SooNo ratings yet
- Aire Premium Delta 8 Vape - 1000mg - Everything 420Document1 pageAire Premium Delta 8 Vape - 1000mg - Everything 4206hsphckmf8No ratings yet
- Training Slides HSE-OH-ST10 Biological HazardsDocument18 pagesTraining Slides HSE-OH-ST10 Biological HazardsAbdul Malik AnsariNo ratings yet
- Lecture3-Inode Table Content and InodeConversionDocument33 pagesLecture3-Inode Table Content and InodeConversionYaminiNo ratings yet
- Article Simple Sentence PDFDocument7 pagesArticle Simple Sentence PDFmaimunah0% (1)
- Module 1: Authentic Assessment in The ClassroomDocument10 pagesModule 1: Authentic Assessment in The ClassroomSir Log100% (1)
- New M Tech Programme in Computer Science and Engineering Artificial Intelligence Data Analytics Self Financing Mode Admissions 2023 - 0Document6 pagesNew M Tech Programme in Computer Science and Engineering Artificial Intelligence Data Analytics Self Financing Mode Admissions 2023 - 0Himesh KumarNo ratings yet
- Gracie Royce - Gracie Charles - Brazilian Jiu-Jitsu Self-Defense TechniquesDocument245 pagesGracie Royce - Gracie Charles - Brazilian Jiu-Jitsu Self-Defense TechniquesPedro MarizNo ratings yet
- Equity ApplicationDocument3 pagesEquity ApplicationanniesachdevNo ratings yet
- Hemo One Analyser Ise 30102023 v29Document8 pagesHemo One Analyser Ise 30102023 v29mohamedessadiNo ratings yet
- Hossein+Nouroozi+i+1+in. PMRes 2020 1Document12 pagesHossein+Nouroozi+i+1+in. PMRes 2020 1Thibault HugNo ratings yet
- DentinDocument133 pagesDentinMohammed hisham khan100% (3)
- Fire Alarm System TypesDocument8 pagesFire Alarm System TypesSusan Macaraeg50% (4)
- Proprietary & Confidential: This Is A Static Sensitive Device. Handle & Store Appropriately To Prevent Esd DamageDocument2 pagesProprietary & Confidential: This Is A Static Sensitive Device. Handle & Store Appropriately To Prevent Esd DamagePawan PalNo ratings yet
- Teff Row PlantingDocument34 pagesTeff Row Plantingmatebneh29 addisNo ratings yet
- Rashomon - WikipediaDocument18 pagesRashomon - WikipediaShareena FarooqueNo ratings yet
- Adjusting Entries, Worksheet and FSDocument26 pagesAdjusting Entries, Worksheet and FSBianca RoswellNo ratings yet
- 4045tf270 Power Unit For Gen Set (12 24v 1800rpm) Sdmo EngineDocument3 pages4045tf270 Power Unit For Gen Set (12 24v 1800rpm) Sdmo EngineRoberto MoraNo ratings yet
- Pa Pi Pu Pe Po: HandakuonDocument23 pagesPa Pi Pu Pe Po: HandakuonmnmrznNo ratings yet
- Laura Su ResumeDocument1 pageLaura Su Resumeapi-280311314No ratings yet
- Disk No. Label Comments BootDocument1 pageDisk No. Label Comments BootDavid HiddingsNo ratings yet
- At EgmrDocument1 pageAt EgmrQasim ButtNo ratings yet
- Part 2 Twentieth Century Naval Dockyards Devonport and Portsmouth Characterisation ReportDocument52 pagesPart 2 Twentieth Century Naval Dockyards Devonport and Portsmouth Characterisation ReportToby ChessonNo ratings yet