Download as pptx, pdf, or txt
You might also like
- Ophthalmology MnemonicsDocument6 pagesOphthalmology MnemonicsRaouf Soliman82% (11)
- Asthma OpdDocument59 pagesAsthma OpdJb TlntinoNo ratings yet
- Recent Developments in United Airways DiseaseDocument7 pagesRecent Developments in United Airways DiseaseStanislaus Stanley SuhermanNo ratings yet
- Prognostic Factors For Refractory Chronic Rhinosinusitis Concomitant With AsthmaDocument9 pagesPrognostic Factors For Refractory Chronic Rhinosinusitis Concomitant With AsthmaChristian VieryNo ratings yet
- MED - Interstitial Lung Disease, Final Sept08Document91 pagesMED - Interstitial Lung Disease, Final Sept08api-3856051100% (3)
- Medical Management Strategies in Acute and Chronic RhinosinusitisDocument6 pagesMedical Management Strategies in Acute and Chronic RhinosinusitisIhdinal MuktiNo ratings yet
- Estado Asmatico: September 2015Document12 pagesEstado Asmatico: September 2015Jaeline Arleth Macias EscobarNo ratings yet
- Acute Respiratory Infection: Darmawan B SetyantoDocument84 pagesAcute Respiratory Infection: Darmawan B SetyantonurhasanahNo ratings yet
- LIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Document56 pagesLIMITLESS PEDIATRICS BY DR NAVEEN - DAY 4 (Green)Biplav SinghNo ratings yet
- Lower Rspiratory Tract - Pneumonia-: BalanceDocument7 pagesLower Rspiratory Tract - Pneumonia-: BalanceSofronio OmboyNo ratings yet
- OkanoDocument8 pagesOkanostanleyNo ratings yet
- PrintDocument7 pagesPrintChandra LathifNo ratings yet
- Childhood Asthma: DR - Rodman Tarigan, Spa.,MkesDocument35 pagesChildhood Asthma: DR - Rodman Tarigan, Spa.,MkesBambang IrwansyahNo ratings yet
- Zbornik Radova I SazetakaDocument133 pagesZbornik Radova I SazetakaSophia RoseNo ratings yet
- Sitasi 14Document8 pagesSitasi 14Silvia ManurungNo ratings yet
- PneumoniaDocument34 pagesPneumoniaAbduraman NazifNo ratings yet
- AsthmaDocument79 pagesAsthmaraj patel100% (1)
- BronchioitisDocument24 pagesBronchioitismitiku aberaNo ratings yet
- Definition & Pathogenesis (Ngân) : Asthma - Current Medical Diagnosis and Treatment 2015Document4 pagesDefinition & Pathogenesis (Ngân) : Asthma - Current Medical Diagnosis and Treatment 2015everydayisagift9999No ratings yet
- Respiratory System For KidsDocument9 pagesRespiratory System For Kidssammim3418No ratings yet
- Wisman DalimuntheDocument40 pagesWisman DalimuntheJimmy AmbaritaNo ratings yet
- Complications of Allergic Rhinitis: David P. Skoner, MD Pittsburgh, PaDocument5 pagesComplications of Allergic Rhinitis: David P. Skoner, MD Pittsburgh, PawurifreshNo ratings yet
- Medicine Card 2Document4 pagesMedicine Card 2Theodore LiwonganNo ratings yet
- Lectures PPS Sinusitis - PpsDocument32 pagesLectures PPS Sinusitis - PpsAlfonso Molina RamirezNo ratings yet
- Respiratory Disorders in ChildrenDocument77 pagesRespiratory Disorders in ChildrenJharaNo ratings yet
- Acute Respiratory InfectionsDocument145 pagesAcute Respiratory InfectionsManuel VIc O. Lacaya100% (1)
- BRONKIEKTASIS BaruDocument23 pagesBRONKIEKTASIS BaruRamanda Cahya UmbarraNo ratings yet
- CRS ASMA - DeaDocument40 pagesCRS ASMA - Deadella srNo ratings yet
- Articulo Parcial 1 Urgencias Respiratorias Perros y GatosDocument23 pagesArticulo Parcial 1 Urgencias Respiratorias Perros y GatosYara Valentina Toledo ManriqueNo ratings yet
- Pulmonary Aspergillosis, What The Generalist Needs To Know - Am J Med 2020Document7 pagesPulmonary Aspergillosis, What The Generalist Needs To Know - Am J Med 2020MICHAEL AMARILLO CORREANo ratings yet
- Chronic Rhinosinusitis With Nasal Polyps: Clinical PracticeDocument9 pagesChronic Rhinosinusitis With Nasal Polyps: Clinical PracticeAnabel SagasteguiNo ratings yet
- A Guide To The Management of Acute Rhinosinusitis in Primary CareDocument4 pagesA Guide To The Management of Acute Rhinosinusitis in Primary CarecubillahhNo ratings yet
- Acute Respiratory Infection: Pediatrics of Guangxi Medical University Nong GuangminDocument62 pagesAcute Respiratory Infection: Pediatrics of Guangxi Medical University Nong GuangminSecret AgentNo ratings yet
- TCRM 2008 4 (2) 2379 - NewtonDocument6 pagesTCRM 2008 4 (2) 2379 - NewtonAndi FirdaNo ratings yet
- Indications, Efficacy, and Safety of Intranasal Corticosteriods in RhinosinusitisDocument4 pagesIndications, Efficacy, and Safety of Intranasal Corticosteriods in RhinosinusitisMilanisti22No ratings yet
- Chapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPDocument19 pagesChapter 9. Bronchial Asthma: Khaled O Hadeli MD, FCCPgireeshsachinNo ratings yet
- 118 ReviewerDocument6 pages118 ReviewerAna Rose Dela CruzNo ratings yet
- Lrti 1Document29 pagesLrti 1Falguni BhoiNo ratings yet
- Diseases of Respiratory SystemDocument23 pagesDiseases of Respiratory SystemMarchelle Fae EsmallaNo ratings yet
- Idiopathic Pulmonary FibrosisDocument47 pagesIdiopathic Pulmonary FibrosisandrewjnrNo ratings yet
- Relationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsDocument7 pagesRelationship Between Asthma and Rhinitis: Epidemiologic, Pathophysiologic, and Therapeutic AspectsStanley SuhermanNo ratings yet
- Approach To A Child With Cough and Difficulty in BreathingDocument23 pagesApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- Bronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)Document29 pagesBronchitis: Presented By:-Himanshi B. B. Sc. (N) 3 Year Gcon (Tehri)Himanshi100% (1)
- Chronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachDocument6 pagesChronic Dry Cough in Allergic Respiratory Diseases: Diagnostic and Management ApproachAaron HongreiNo ratings yet
- Case Study On CopdDocument24 pagesCase Study On CopdPawan Batth67% (3)
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- 03 Asthma FinalDocument50 pages03 Asthma FinalG SNo ratings yet
- Management of Nasal Polyposis: C. Bachert, T. RobillardDocument10 pagesManagement of Nasal Polyposis: C. Bachert, T. RobillardAnonymous il1cFm6No ratings yet
- Clear Secretion Viral Infection Yellow, Green: Bacterial!Document72 pagesClear Secretion Viral Infection Yellow, Green: Bacterial!irwiennyNo ratings yet
- 234 1164 1 SMDocument7 pages234 1164 1 SMsorayahyuraNo ratings yet
- Respiratory System DisorderDocument46 pagesRespiratory System DisorderYaniNo ratings yet
- NCM 112 Lec 2Document64 pagesNCM 112 Lec 2JIMENEZ, TRISHA MARIE D.No ratings yet
- Lower Airway Disease: Copd Ashtma Tuberculosis Pneumonia Cyst FibrosisDocument39 pagesLower Airway Disease: Copd Ashtma Tuberculosis Pneumonia Cyst FibrosisWidi Marsha FadilaNo ratings yet
- Clinically Relevant Phenotypes in Chronic RhinosinusitisDocument22 pagesClinically Relevant Phenotypes in Chronic RhinosinusitisA.No ratings yet
- Asthm 2Document34 pagesAsthm 2AbuAbdullah KhanNo ratings yet
- Ast 2Document17 pagesAst 2AbuAbdullah KhanNo ratings yet
- Asthma in The Primary Care Setting 2019 Medical Clinics of North AmericaDocument18 pagesAsthma in The Primary Care Setting 2019 Medical Clinics of North AmericaYony Morales LeonNo ratings yet
- Restrictive Lung Diseases PDFDocument49 pagesRestrictive Lung Diseases PDFwwwwwwwwwwwwwwwNo ratings yet
- Antibiotics Training ManualDocument149 pagesAntibiotics Training ManualImran MullaNo ratings yet
- Medical Mnemonic Sketches : Pulmonary DiseasesFrom EverandMedical Mnemonic Sketches : Pulmonary DiseasesNo ratings yet
- Acl Bearing 2018Document16 pagesAcl Bearing 2018LEONARDO CANDORNo ratings yet
- Instruction Manual: E48W13A-AUDocument2 pagesInstruction Manual: E48W13A-AUDanilo100% (1)
- Cheat Codes I Know at 43 That I Wish I Knew at 23Document10 pagesCheat Codes I Know at 43 That I Wish I Knew at 23Stephanie HerawatiNo ratings yet
- Utility Experiment Verifies Destructive Nature of VLF HIPOT Withstand TestingDocument4 pagesUtility Experiment Verifies Destructive Nature of VLF HIPOT Withstand Testingapricot2009No ratings yet
- Swale (Landform) - WikipediaDocument2 pagesSwale (Landform) - WikipediaMohamedNo ratings yet
- Fabrication & Performance Testing1Document27 pagesFabrication & Performance Testing1DIPAK VINAYAK SHIRBHATENo ratings yet
- Vitodens 100w wb1b SeriesDocument100 pagesVitodens 100w wb1b Seriesclaudyu_fNo ratings yet
- Network SecurityDocument47 pagesNetwork SecurityFahad Ahmad100% (1)
- Final DraftDocument5 pagesFinal Draftapi-451064930No ratings yet
- EE311A 2021 AV Slides L23Document13 pagesEE311A 2021 AV Slides L23Ananya AgarwalNo ratings yet
- GGT FluitestDocument4 pagesGGT FluitestCristian LaraNo ratings yet
- Hypnisis in PsychosomaticsDocument3 pagesHypnisis in PsychosomaticsJoseph MeyersonNo ratings yet
- Springfield Building Department Inspectional Services Notice of ViolationsDocument6 pagesSpringfield Building Department Inspectional Services Notice of ViolationsThe Republican/MassLive.comNo ratings yet
- Development of Normal Occlusion Part 2 Copy 2Document49 pagesDevelopment of Normal Occlusion Part 2 Copy 2MSA universityNo ratings yet
- 2.tfs Spring Source DDocument2 pages2.tfs Spring Source DErica DouglasNo ratings yet
- Tipe A - Test Admin Shopee ExpressDocument6 pagesTipe A - Test Admin Shopee ExpressHapsyah MarniNo ratings yet
- Writing Task 2Document50 pagesWriting Task 2Khanh Chi Pham100% (1)
- Semi Detailed Lesson Plan in TLE 77Document2 pagesSemi Detailed Lesson Plan in TLE 77Kimberly MaeNo ratings yet
- Mining Iii To Viii PDFDocument77 pagesMining Iii To Viii PDFRaja Prabhu0% (1)
- ELG 400 Comple SMDocument230 pagesELG 400 Comple SMVirginia Department of Emergency Management100% (2)
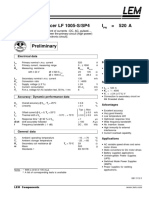
- Current Transducer LF 1005-S/SP4 I 520 ADocument2 pagesCurrent Transducer LF 1005-S/SP4 I 520 ARaul quispe quispeNo ratings yet
- RusDocument42 pagesRusОльга КалмыковаNo ratings yet
- Methods For Genetic Study of ManDocument54 pagesMethods For Genetic Study of ManNavneetNo ratings yet
- Entrep - Product ProposalDocument4 pagesEntrep - Product ProposalPrincess ArabelaNo ratings yet
- Pemberian Obat Dengan Kewaspadaan Tinggi Pada Pasien ICUDocument38 pagesPemberian Obat Dengan Kewaspadaan Tinggi Pada Pasien ICUIndriWatiNo ratings yet
- Issuance of Insanity 2Document278 pagesIssuance of Insanity 2Jonatha B SantosNo ratings yet
- Econometric Analysis of Panel Data: William Greene Department of Economics University of South FloridaDocument116 pagesEconometric Analysis of Panel Data: William Greene Department of Economics University of South Florida1111111111111-859751No ratings yet
- Conceptual Design For Leachate Treatment Plant (LTP)Document19 pagesConceptual Design For Leachate Treatment Plant (LTP)Akyas M100% (1)
- 32AC219ENDocument207 pages32AC219ENArno RaspoetNo ratings yet