
Disusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., Apt
Disusun Oleh: WIDI TASTARI (16330050) : Farmakoterapi 1 Dosen: Okpri Meila, M.Farm., Apt
You might also like
- AGA DDSEP 10 Chapter 6 QA HepatologyDocument42 pagesAGA DDSEP 10 Chapter 6 QA HepatologyHima Alqahtani0% (1)
- Cirohsis of LiverDocument29 pagesCirohsis of LiverAnonymous L95gMHSNo ratings yet
- TDM Dan Rancangan Aturan DosisDocument37 pagesTDM Dan Rancangan Aturan Dosisadelin ransunNo ratings yet
- Msds AgitaDocument6 pagesMsds Agitaika setiawatiNo ratings yet
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaNo ratings yet
- Hasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityDocument51 pagesHasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityMuhammad Yasdar BahriNo ratings yet
- Neuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanDocument41 pagesNeuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanHatta Diana TariganNo ratings yet
- GastroparesisDocument7 pagesGastroparesisapi-548943629No ratings yet
- FARMAKOEKONOMI1Document38 pagesFARMAKOEKONOMI1AbnerDNeroNo ratings yet
- Perdarahan Saluran CernaDocument46 pagesPerdarahan Saluran CernaHapsari Kartika DewiNo ratings yet
- AntihistaminDocument44 pagesAntihistaminDWI RAHMA HALIDANo ratings yet
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- CND 4.medication & Dispensing ErrorDocument32 pagesCND 4.medication & Dispensing Errorlisnawati farmasicbthNo ratings yet
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaNo ratings yet
- Farmakologi Antiagina TTMDocument83 pagesFarmakologi Antiagina TTMEpha Lumban GaolNo ratings yet
- Pengelolaan Dan Penggunaan Obat Di Rumah SakitDocument30 pagesPengelolaan Dan Penggunaan Obat Di Rumah SakitkuronohanaNo ratings yet
- JNC 6 Vs 7Document2 pagesJNC 6 Vs 7zhen33No ratings yet
- Hipertensi Emergensi (Herbesser)Document41 pagesHipertensi Emergensi (Herbesser)riski novika100% (1)
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- antiHIPERTENSI 2020Document88 pagesantiHIPERTENSI 2020nabila fikriNo ratings yet
- Kit System ManagementDocument29 pagesKit System ManagementTifa IstiwaNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- 5 - Farmakoterapi Pediatri - Dr. Nanang MunifDocument45 pages5 - Farmakoterapi Pediatri - Dr. Nanang MunifEdzhar Hasiholan100% (1)
- Hipertensi: Dr. Made Winatra Satya PutraDocument16 pagesHipertensi: Dr. Made Winatra Satya PutraMade Winatra Satya PutraNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Sirosis HatiDocument10 pagesSirosis HatisakinahNo ratings yet
- Dr. Pandu - Obat-Obat AntivirusDocument36 pagesDr. Pandu - Obat-Obat AntivirusChandraNo ratings yet
- Farmakoterapi AntihipertensiDocument37 pagesFarmakoterapi AntihipertensipkmbangilNo ratings yet
- (A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFDocument105 pages(A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFNugroho Wisnu PutroNo ratings yet
- Farmakoterapi Pada SepsisDocument36 pagesFarmakoterapi Pada SepsisNathaniaNo ratings yet
- Clinical Pharmacy The KidnyDocument34 pagesClinical Pharmacy The KidnyAta07No ratings yet
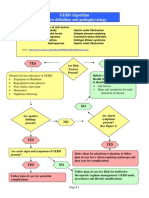
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Antikanker S1-IvcDocument72 pagesAntikanker S1-IvcNina RishantiNo ratings yet
- Sistem UrinariaDocument31 pagesSistem UrinariaAni AndrianiNo ratings yet
- Algorith UTI 20121218 PDFDocument1 pageAlgorith UTI 20121218 PDFIin fermitaNo ratings yet
- Endocrine Disorders and Its Neurologic ManifestationsDocument16 pagesEndocrine Disorders and Its Neurologic ManifestationsKuntal BhadraNo ratings yet
- Maya Septriana S.Si., Apt., M.SiDocument18 pagesMaya Septriana S.Si., Apt., M.SiNur Ima ErvianaNo ratings yet
- Pendekatan SOAP Farmasi KlinikDocument40 pagesPendekatan SOAP Farmasi KlinikmadeNo ratings yet
- Bpac Inr Poem 2006 WVDocument26 pagesBpac Inr Poem 2006 WVmrezasyahliNo ratings yet
- Leaflet TBCDocument2 pagesLeaflet TBCircakoeNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Managing Drug Suply 2017.Ppt AZIZAHDocument17 pagesManaging Drug Suply 2017.Ppt AZIZAHwandameritaNo ratings yet
- Bone and JointDocument43 pagesBone and Jointjheannie02No ratings yet
- Penyakit Arteri KoronerDocument27 pagesPenyakit Arteri KoronerchandrahidayatNo ratings yet
- Dr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: NamaDocument28 pagesDr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: Namasri handayaniNo ratings yet
- Medical Ethics Handout 2018Document37 pagesMedical Ethics Handout 2018Muhamad GaafarNo ratings yet
- Turunan Imidazoline Crodazoline oDocument2 pagesTurunan Imidazoline Crodazoline oMuhammad Syarif HidayatullahNo ratings yet
- Chrono Pharmaco LDocument46 pagesChrono Pharmaco LJaved AliNo ratings yet
- Obat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptDocument27 pagesObat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptanikNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument6 pagesAnatomi Dan Fisiologi GinjalAndy F MonroeNo ratings yet
- 275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFDocument6 pages275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFtiarasrisudarsihNo ratings yet
- Analisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanDocument14 pagesAnalisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanwahyuNo ratings yet
- Hipertensi 2Document43 pagesHipertensi 2Sri AfniNo ratings yet
- Beyond-Use-DateDocument9 pagesBeyond-Use-DateAnidraqif Hastina100% (1)
- Dialysis Drugs 2010Document56 pagesDialysis Drugs 2010mgh100% (2)
- 2 Cost Utility AnalysisDocument29 pages2 Cost Utility Analysisapi-3723612No ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection Fractionsri wahyuniNo ratings yet
- Viral HepatitisDocument6 pagesViral HepatitisAli salimNo ratings yet
- Hepatitis C: by DR Faiza SamadDocument44 pagesHepatitis C: by DR Faiza SamadMuhammad MakkiNo ratings yet
- Viral Hepatitis & HIVDocument14 pagesViral Hepatitis & HIVaymnhssn2020No ratings yet
- HBV HCV 2024Document21 pagesHBV HCV 2024keisyafulqiNo ratings yet
- PENYAKIT HATI (Uas)Document27 pagesPENYAKIT HATI (Uas)Cinsy PaskalineNo ratings yet
- Drug Induced Liver DiseaseDocument15 pagesDrug Induced Liver DiseaseMUGHALNo ratings yet
- CPLD Final ProgramDocument3 pagesCPLD Final ProgramsriNo ratings yet
- Pleted.20230901 20230927Document51 pagesPleted.20230901 20230927Fariz MuhamadNo ratings yet
- ABSTRAK-Izzatul AzmiDocument3 pagesABSTRAK-Izzatul AzmiMuhammad DzulfachriNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseRaju NiraulaNo ratings yet
- The SGOT/SGPT Ratio - An Indicator of Alcoholic Liver DiseaseDocument4 pagesThe SGOT/SGPT Ratio - An Indicator of Alcoholic Liver DiseaseSahara MaindokaNo ratings yet
- Liver FibrosisDocument29 pagesLiver FibrosisAmira HelayelNo ratings yet
- Fibroscan: Hepatitis CDocument4 pagesFibroscan: Hepatitis CMuhammad Halil GibranNo ratings yet
- Cholelytiasis 2013 2015Document37 pagesCholelytiasis 2013 2015Nurul RamadhantyNo ratings yet
- CirroseDocument6 pagesCirrosePaulinha CostaNo ratings yet
- Interpretation of FibroScanDocument16 pagesInterpretation of FibroScanAAMIRNo ratings yet
- 1 s2.0 S1665268122002186 MainDocument4 pages1 s2.0 S1665268122002186 MainJulián DuránNo ratings yet
- Cirrhosis and Its Complications: Further ReadingDocument10 pagesCirrhosis and Its Complications: Further ReadingJacob BorongNo ratings yet
- Etiologi Dan Patogenesis Ikterus,...Document103 pagesEtiologi Dan Patogenesis Ikterus,...Raditya PrimaNo ratings yet
- Tejas - Expert Ayurveda - Search - Feb 23Document130 pagesTejas - Expert Ayurveda - Search - Feb 23Priya AswaniNo ratings yet
- Enfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseDocument13 pagesEnfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseasierrNo ratings yet
- LIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageLIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportM ShafiqNo ratings yet
- Fibroscan Interpretation - Guide 2020Document2 pagesFibroscan Interpretation - Guide 2020Faisal BaigNo ratings yet
- Daftar Pustaka Referat Hep CDocument2 pagesDaftar Pustaka Referat Hep CJennifer AnatasyaNo ratings yet
- Herbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesDocument6 pagesHerbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesNariNo ratings yet
- Liver Cirrhosis: Dr. Rudy Dwi LaksonoDocument26 pagesLiver Cirrhosis: Dr. Rudy Dwi LaksonoMarthalena Simamora100% (1)
- Chapter 18 - Liver and Biliary TractDocument18 pagesChapter 18 - Liver and Biliary TractAgnieszka WisniewskaNo ratings yet
- Liver Cirrhosis: Dr. Soegiarto Gani, SPPDDocument26 pagesLiver Cirrhosis: Dr. Soegiarto Gani, SPPDmirwan bakriNo ratings yet
- Alcoholic Liver DiseaseDocument10 pagesAlcoholic Liver DiseaseNishanth ReddyNo ratings yet
- Dapus Laporan DK 4Document5 pagesDapus Laporan DK 4Stephanie Gabriella KamNo ratings yet
- Sirosis HatiDocument17 pagesSirosis HatiAndrianto WongkarNo ratings yet
- Beyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood TestsDocument18 pagesBeyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood Tests李冠No ratings yet























































































Download as pptx, pdf, or txt
You might also like
- AGA DDSEP 10 Chapter 6 QA HepatologyDocument42 pagesAGA DDSEP 10 Chapter 6 QA HepatologyHima Alqahtani0% (1)
- Cirohsis of LiverDocument29 pagesCirohsis of LiverAnonymous L95gMHSNo ratings yet
- TDM Dan Rancangan Aturan DosisDocument37 pagesTDM Dan Rancangan Aturan Dosisadelin ransunNo ratings yet
- Msds AgitaDocument6 pagesMsds Agitaika setiawatiNo ratings yet
- 01 C & D Latar Belakang GPPDocument38 pages01 C & D Latar Belakang GPPPrisma TridaNo ratings yet
- Hasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityDocument51 pagesHasyim Kasim: Nephrology and Hypertension Division, Department of Internal Medicine Medical Faculty Hasanuddin UniversityMuhammad Yasdar BahriNo ratings yet
- Neuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanDocument41 pagesNeuropathy: Departemen Neurologi FK Usu/ Rsup H. Adam Malik MedanHatta Diana TariganNo ratings yet
- GastroparesisDocument7 pagesGastroparesisapi-548943629No ratings yet
- FARMAKOEKONOMI1Document38 pagesFARMAKOEKONOMI1AbnerDNeroNo ratings yet
- Perdarahan Saluran CernaDocument46 pagesPerdarahan Saluran CernaHapsari Kartika DewiNo ratings yet
- AntihistaminDocument44 pagesAntihistaminDWI RAHMA HALIDANo ratings yet
- Farmakoterapi Pada LansiaDocument29 pagesFarmakoterapi Pada LansiaPuterinugraha Wanca ApatyaNo ratings yet
- CND 4.medication & Dispensing ErrorDocument32 pagesCND 4.medication & Dispensing Errorlisnawati farmasicbthNo ratings yet
- Farmasi Rumah SakitDocument97 pagesFarmasi Rumah SakitkuronohanaNo ratings yet
- Farmakologi Antiagina TTMDocument83 pagesFarmakologi Antiagina TTMEpha Lumban GaolNo ratings yet
- Pengelolaan Dan Penggunaan Obat Di Rumah SakitDocument30 pagesPengelolaan Dan Penggunaan Obat Di Rumah SakitkuronohanaNo ratings yet
- JNC 6 Vs 7Document2 pagesJNC 6 Vs 7zhen33No ratings yet
- Hipertensi Emergensi (Herbesser)Document41 pagesHipertensi Emergensi (Herbesser)riski novika100% (1)
- Renal PharmacologyDocument52 pagesRenal PharmacologyashrafNo ratings yet
- Prescribing Antipsychotics in Geriatric Patients:: First of 3 PartsDocument8 pagesPrescribing Antipsychotics in Geriatric Patients:: First of 3 PartsAlexRázuri100% (1)
- antiHIPERTENSI 2020Document88 pagesantiHIPERTENSI 2020nabila fikriNo ratings yet
- Kit System ManagementDocument29 pagesKit System ManagementTifa IstiwaNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- 5 - Farmakoterapi Pediatri - Dr. Nanang MunifDocument45 pages5 - Farmakoterapi Pediatri - Dr. Nanang MunifEdzhar Hasiholan100% (1)
- Hipertensi: Dr. Made Winatra Satya PutraDocument16 pagesHipertensi: Dr. Made Winatra Satya PutraMade Winatra Satya PutraNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- Sirosis HatiDocument10 pagesSirosis HatisakinahNo ratings yet
- Dr. Pandu - Obat-Obat AntivirusDocument36 pagesDr. Pandu - Obat-Obat AntivirusChandraNo ratings yet
- Farmakoterapi AntihipertensiDocument37 pagesFarmakoterapi AntihipertensipkmbangilNo ratings yet
- (A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFDocument105 pages(A) Pengembangan Obat - OBAT BIOLOGI - Ana Indrayati PDFNugroho Wisnu PutroNo ratings yet
- Farmakoterapi Pada SepsisDocument36 pagesFarmakoterapi Pada SepsisNathaniaNo ratings yet
- Clinical Pharmacy The KidnyDocument34 pagesClinical Pharmacy The KidnyAta07No ratings yet
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Antikanker S1-IvcDocument72 pagesAntikanker S1-IvcNina RishantiNo ratings yet
- Sistem UrinariaDocument31 pagesSistem UrinariaAni AndrianiNo ratings yet
- Algorith UTI 20121218 PDFDocument1 pageAlgorith UTI 20121218 PDFIin fermitaNo ratings yet
- Endocrine Disorders and Its Neurologic ManifestationsDocument16 pagesEndocrine Disorders and Its Neurologic ManifestationsKuntal BhadraNo ratings yet
- Maya Septriana S.Si., Apt., M.SiDocument18 pagesMaya Septriana S.Si., Apt., M.SiNur Ima ErvianaNo ratings yet
- Pendekatan SOAP Farmasi KlinikDocument40 pagesPendekatan SOAP Farmasi KlinikmadeNo ratings yet
- Bpac Inr Poem 2006 WVDocument26 pagesBpac Inr Poem 2006 WVmrezasyahliNo ratings yet
- Leaflet TBCDocument2 pagesLeaflet TBCircakoeNo ratings yet
- I. Farmakoterapi RasionalDocument24 pagesI. Farmakoterapi RasionalAthirah M.NoerNo ratings yet
- Managing Drug Suply 2017.Ppt AZIZAHDocument17 pagesManaging Drug Suply 2017.Ppt AZIZAHwandameritaNo ratings yet
- Bone and JointDocument43 pagesBone and Jointjheannie02No ratings yet
- Penyakit Arteri KoronerDocument27 pagesPenyakit Arteri KoronerchandrahidayatNo ratings yet
- Dr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: NamaDocument28 pagesDr. Ronald Irwanto Natadidjaja, SPPD - Kpti, Finasim: Namasri handayaniNo ratings yet
- Medical Ethics Handout 2018Document37 pagesMedical Ethics Handout 2018Muhamad GaafarNo ratings yet
- Turunan Imidazoline Crodazoline oDocument2 pagesTurunan Imidazoline Crodazoline oMuhammad Syarif HidayatullahNo ratings yet
- Chrono Pharmaco LDocument46 pagesChrono Pharmaco LJaved AliNo ratings yet
- Obat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptDocument27 pagesObat Saluran Cerna: Anjar Mahardian Kusuma, M. SC., AptanikNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument6 pagesAnatomi Dan Fisiologi GinjalAndy F MonroeNo ratings yet
- 275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFDocument6 pages275 280 Drug Related Problems Antipsikotik Pada Pasien Skizofrenia PDFtiarasrisudarsihNo ratings yet
- Analisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanDocument14 pagesAnalisis Pelayanan Terapeutik Pada Pasien Tuberkulosis Resisten Obat Di Kota MedanwahyuNo ratings yet
- Hipertensi 2Document43 pagesHipertensi 2Sri AfniNo ratings yet
- Beyond-Use-DateDocument9 pagesBeyond-Use-DateAnidraqif Hastina100% (1)
- Dialysis Drugs 2010Document56 pagesDialysis Drugs 2010mgh100% (2)
- 2 Cost Utility AnalysisDocument29 pages2 Cost Utility Analysisapi-3723612No ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection Fractionsri wahyuniNo ratings yet
- Viral HepatitisDocument6 pagesViral HepatitisAli salimNo ratings yet
- Hepatitis C: by DR Faiza SamadDocument44 pagesHepatitis C: by DR Faiza SamadMuhammad MakkiNo ratings yet
- Viral Hepatitis & HIVDocument14 pagesViral Hepatitis & HIVaymnhssn2020No ratings yet
- HBV HCV 2024Document21 pagesHBV HCV 2024keisyafulqiNo ratings yet
- PENYAKIT HATI (Uas)Document27 pagesPENYAKIT HATI (Uas)Cinsy PaskalineNo ratings yet
- Drug Induced Liver DiseaseDocument15 pagesDrug Induced Liver DiseaseMUGHALNo ratings yet
- CPLD Final ProgramDocument3 pagesCPLD Final ProgramsriNo ratings yet
- Pleted.20230901 20230927Document51 pagesPleted.20230901 20230927Fariz MuhamadNo ratings yet
- ABSTRAK-Izzatul AzmiDocument3 pagesABSTRAK-Izzatul AzmiMuhammad DzulfachriNo ratings yet
- Alcoholic Liver DiseaseDocument22 pagesAlcoholic Liver DiseaseRaju NiraulaNo ratings yet
- The SGOT/SGPT Ratio - An Indicator of Alcoholic Liver DiseaseDocument4 pagesThe SGOT/SGPT Ratio - An Indicator of Alcoholic Liver DiseaseSahara MaindokaNo ratings yet
- Liver FibrosisDocument29 pagesLiver FibrosisAmira HelayelNo ratings yet
- Fibroscan: Hepatitis CDocument4 pagesFibroscan: Hepatitis CMuhammad Halil GibranNo ratings yet
- Cholelytiasis 2013 2015Document37 pagesCholelytiasis 2013 2015Nurul RamadhantyNo ratings yet
- CirroseDocument6 pagesCirrosePaulinha CostaNo ratings yet
- Interpretation of FibroScanDocument16 pagesInterpretation of FibroScanAAMIRNo ratings yet
- 1 s2.0 S1665268122002186 MainDocument4 pages1 s2.0 S1665268122002186 MainJulián DuránNo ratings yet
- Cirrhosis and Its Complications: Further ReadingDocument10 pagesCirrhosis and Its Complications: Further ReadingJacob BorongNo ratings yet
- Etiologi Dan Patogenesis Ikterus,...Document103 pagesEtiologi Dan Patogenesis Ikterus,...Raditya PrimaNo ratings yet
- Tejas - Expert Ayurveda - Search - Feb 23Document130 pagesTejas - Expert Ayurveda - Search - Feb 23Priya AswaniNo ratings yet
- Enfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseDocument13 pagesEnfermedad Hepática Por Alcohol: Alcoholic Liver DiseaseasierrNo ratings yet
- LIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportDocument1 pageLIVER PROFILE LFT Test Report Format Example Sample Template Drlogy Lab ReportM ShafiqNo ratings yet
- Fibroscan Interpretation - Guide 2020Document2 pagesFibroscan Interpretation - Guide 2020Faisal BaigNo ratings yet
- Daftar Pustaka Referat Hep CDocument2 pagesDaftar Pustaka Referat Hep CJennifer AnatasyaNo ratings yet
- Herbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesDocument6 pagesHerbal Hepatotoxicity: Suspected Cases Assessed For Alternative CausesNariNo ratings yet
- Liver Cirrhosis: Dr. Rudy Dwi LaksonoDocument26 pagesLiver Cirrhosis: Dr. Rudy Dwi LaksonoMarthalena Simamora100% (1)
- Chapter 18 - Liver and Biliary TractDocument18 pagesChapter 18 - Liver and Biliary TractAgnieszka WisniewskaNo ratings yet
- Liver Cirrhosis: Dr. Soegiarto Gani, SPPDDocument26 pagesLiver Cirrhosis: Dr. Soegiarto Gani, SPPDmirwan bakriNo ratings yet
- Alcoholic Liver DiseaseDocument10 pagesAlcoholic Liver DiseaseNishanth ReddyNo ratings yet
- Dapus Laporan DK 4Document5 pagesDapus Laporan DK 4Stephanie Gabriella KamNo ratings yet
- Sirosis HatiDocument17 pagesSirosis HatiAndrianto WongkarNo ratings yet
- Beyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood TestsDocument18 pagesBeyond The Liver Function Tests: A Radiologist's Guide To The Liver Blood Tests李冠No ratings yet