Download as pptx, pdf, or txt
You might also like
- Renal Replacement TherapyDocument303 pagesRenal Replacement TherapyPaloma Cruz100% (9)
- Xray ReportDocument26 pagesXray Reports00uravNo ratings yet
- The Ultimate Guide To Anxiety DisordersDocument66 pagesThe Ultimate Guide To Anxiety Disordersnajaxx100% (2)
- Bagaimana Menangani Pendarahan Uterus Abnormal (PUA) Secara OptimalDocument34 pagesBagaimana Menangani Pendarahan Uterus Abnormal (PUA) Secara OptimalTalita NandiaNo ratings yet
- Teratozoospermia: Spotlight On The Main Genetic Actors in The HumanDocument31 pagesTeratozoospermia: Spotlight On The Main Genetic Actors in The HumanAdhe Cakra Mandala PutraNo ratings yet
- Mechanisms of Obesity-Induced Male Infertility PDFDocument24 pagesMechanisms of Obesity-Induced Male Infertility PDFshishir kumarNo ratings yet
- Jurnal 3Document20 pagesJurnal 3mardha tillahNo ratings yet
- Autophagy Is Upregulated in Ovarian Endometriosis A Possi - 2015 - Fertility AnDocument9 pagesAutophagy Is Upregulated in Ovarian Endometriosis A Possi - 2015 - Fertility Anjayeto4038No ratings yet
- Role of MicronizedDocument40 pagesRole of MicronizedAkhilesh KumarNo ratings yet
- Andrology - 2017 - Garbarino Azúa - Fibroblast Growth Factor 2 FGF2 Is Present in Human Spermatozoa and Is Related WithDocument9 pagesAndrology - 2017 - Garbarino Azúa - Fibroblast Growth Factor 2 FGF2 Is Present in Human Spermatozoa and Is Related WithPhuong Thy NguyenNo ratings yet
- Intl J Gynecology Obste - 2022 - Munro - The FIGO Ovulatory Disorders Classification SystemDocument20 pagesIntl J Gynecology Obste - 2022 - Munro - The FIGO Ovulatory Disorders Classification SystemMinerba MelendrezNo ratings yet
- Thin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDocument56 pagesThin Endometrium: Dr. Astha Gupta Senior Ivf and Infertility Consultant Milann Fertility, DelhiDrAstha Gupta100% (2)
- Andrology - 2019 - Huang - Effects of Folic Acid On Oligozoospermia With MTHFR Polymorphisms in Term of Seminal ParametersDocument7 pagesAndrology - 2019 - Huang - Effects of Folic Acid On Oligozoospermia With MTHFR Polymorphisms in Term of Seminal Parametersria.janitaNo ratings yet
- Gyne - Feu ReviewerDocument87 pagesGyne - Feu ReviewerKoko RoqueNo ratings yet
- Laboratory Assessment of Male Infertility - A Guide For The UrologistDocument4 pagesLaboratory Assessment of Male Infertility - A Guide For The UrologistMehmet Ali KaragözNo ratings yet
- The Use of Acupuncture With in Vitro Fertilization: Is There A Point?Document10 pagesThe Use of Acupuncture With in Vitro Fertilization: Is There A Point?lu salviaNo ratings yet
- In Cosmetology and TrichologyDocument72 pagesIn Cosmetology and TrichologySasi AttiliNo ratings yet
- TestosteronaDocument7 pagesTestosteronaTomás DíazNo ratings yet
- Novel Concepts On Pregnancy Clocks and Alarms: Redundancy and Synergy in Human ParturitionDocument26 pagesNovel Concepts On Pregnancy Clocks and Alarms: Redundancy and Synergy in Human ParturitionFedrik Monte Kristo LimbongNo ratings yet
- Comparación de Las Concentraciones de Zinc en Sangre y Plasma Seminal y Los Diversos Parámetros Espermáticos Entre Hombres Fértiles e InfértilesDocument5 pagesComparación de Las Concentraciones de Zinc en Sangre y Plasma Seminal y Los Diversos Parámetros Espermáticos Entre Hombres Fértiles e Infértileswilson vasquezNo ratings yet
- Sperm Morphological Defects Related To Environment, Lifestyle and Medical History of 1001 Male Partners of Pregnant Women From Four European CitiesDocument8 pagesSperm Morphological Defects Related To Environment, Lifestyle and Medical History of 1001 Male Partners of Pregnant Women From Four European CitiesOum BanatNo ratings yet
- Current Management of PCOSDocument46 pagesCurrent Management of PCOSFauzan MasriNo ratings yet
- Benefits of Oral Contraceptive Pill Pretreatment in Endometriosis For IVFICSI-ETDocument6 pagesBenefits of Oral Contraceptive Pill Pretreatment in Endometriosis For IVFICSI-ETardirshajiNo ratings yet
- Abnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarDocument80 pagesAbnormal Uterine Bleeding: Dr. Jasmina Begum Assistant Professor AIIMS, BhubaneswarSharoon KumarNo ratings yet
- (17417899 - Reproduction) Mitochondrial Humanin Peptide Acts As A Cytoprotective Factor in Granulosa Cell SurvivalDocument11 pages(17417899 - Reproduction) Mitochondrial Humanin Peptide Acts As A Cytoprotective Factor in Granulosa Cell SurvivalLeilane GlienkeNo ratings yet
- Del 484Document9 pagesDel 484tria nurdianaNo ratings yet
- Induksi Ovulasi RevDocument38 pagesInduksi Ovulasi RevBambang SulistyoNo ratings yet
- Kuze 1997Document8 pagesKuze 1997Sarly FebrianaNo ratings yet
- Acciones Fisiologicas y Patologicas de Los Androgenos en El OvarioDocument9 pagesAcciones Fisiologicas y Patologicas de Los Androgenos en El OvarioDaniel J Alejos CNo ratings yet
- Artigo Sobre A Osteopontina Versão OriginalDocument5 pagesArtigo Sobre A Osteopontina Versão OriginalAjaxerrorNo ratings yet
- Evaluate The Effectiveness of Structured Teaching Program Regarding Menopausal Syndrome Among The Peri Menopausal Women in Bandarulanka, Amalapuram, Andhra PradeshDocument9 pagesEvaluate The Effectiveness of Structured Teaching Program Regarding Menopausal Syndrome Among The Peri Menopausal Women in Bandarulanka, Amalapuram, Andhra PradeshInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Myoinositol: Does It Improve Sperm Mitochondrial Function and Sperm Motility?Document6 pagesMyoinositol: Does It Improve Sperm Mitochondrial Function and Sperm Motility?Anca CucuNo ratings yet
- 1977 Zini Hum-Reprod 1999Document3 pages1977 Zini Hum-Reprod 1999iridadajtiNo ratings yet
- Cme Reviewarticle: The Role of Genes in The Development of Mullerian AnomaliesDocument9 pagesCme Reviewarticle: The Role of Genes in The Development of Mullerian Anomaliesapi-54418266No ratings yet
- Cessation of Renal Morphogenesis in MiceDocument16 pagesCessation of Renal Morphogenesis in MiceWilan KrisnaNo ratings yet
- Clinco-Pathological Patterns in Women With Dysfunctional Uterine BleedingDocument7 pagesClinco-Pathological Patterns in Women With Dysfunctional Uterine BleedingAzzhr FahNo ratings yet
- 2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno TeratozoospermiaDocument12 pages2018Andrology-Colpi-European Academy of Andrology Guideline Management of Oligo Astheno Teratozoospermiakong_666064846No ratings yet
- Sperm Mitochondrial DNA DeletionDocument6 pagesSperm Mitochondrial DNA DeletionOday AL-JubooriNo ratings yet
- Kim, 2009Document4 pagesKim, 2009silviaramira1121No ratings yet
- Differential Intensity-Dependent Effects of Pulsed PEMAGDocument12 pagesDifferential Intensity-Dependent Effects of Pulsed PEMAGvayyikNo ratings yet
- Uterine Myoma - Surgical or Medical1.original.15615304794199696230846510162Document42 pagesUterine Myoma - Surgical or Medical1.original.15615304794199696230846510162Mi MaymdNo ratings yet
- Artículo Menopausia 2Document17 pagesArtículo Menopausia 2daniela otaNo ratings yet
- Watson Physio First April 07Document11 pagesWatson Physio First April 07Muhammad FahmyNo ratings yet
- Tog 12150Document10 pagesTog 12150saeed hasan saeedNo ratings yet
- Uncovering Changes in Proteomic Signature of Rat Pelvic Floor Muscles in PregnancyDocument9 pagesUncovering Changes in Proteomic Signature of Rat Pelvic Floor Muscles in PregnancySueNo ratings yet
- Regulation of Uterine Function: A Biochemical Conundrum in The Regulation of Smooth Muscle RelaxationDocument9 pagesRegulation of Uterine Function: A Biochemical Conundrum in The Regulation of Smooth Muscle Relaxationtiga sekawan sekawanNo ratings yet
- Norton2014 PDFDocument5 pagesNorton2014 PDFGladys SusantyNo ratings yet
- Scaramuzzi 2011 PDFDocument24 pagesScaramuzzi 2011 PDFKarol Mariam VelázquezNo ratings yet
- Mechanism of Action of Levonorgestrel Contraceptive ImplantsDocument8 pagesMechanism of Action of Levonorgestrel Contraceptive ImplantsaldyNo ratings yet
- MR 20 45301Document6 pagesMR 20 45301MOSTOFA SHAMIM FERDOUSNo ratings yet
- Vitamin D and PCOSDocument39 pagesVitamin D and PCOSsyafiraNo ratings yet
- Endometriosis and Human Infertility: A New Investigation Into The Role of Eutopic EndometriumDocument8 pagesEndometriosis and Human Infertility: A New Investigation Into The Role of Eutopic Endometrium12ock312No ratings yet
- Nerve Fibres Detection in Paired Eutopic and Ectopic Endometria From Women With Endometriosis - Correlation With Nerve Growth Factor ExpressionDocument19 pagesNerve Fibres Detection in Paired Eutopic and Ectopic Endometria From Women With Endometriosis - Correlation With Nerve Growth Factor ExpressionNur Ilmi SofiahNo ratings yet
- Role of Anti-Müllerian Hormone in The Pathogenesis of Polycystic Ovary SyndromeDocument9 pagesRole of Anti-Müllerian Hormone in The Pathogenesis of Polycystic Ovary SyndromeHAVIZ YUADNo ratings yet
- IJSHR50Document12 pagesIJSHR50OMKAR DANDEKARNo ratings yet
- Captura de Pantalla 2024-04-06 A La(s) 0.37.53Document14 pagesCaptura de Pantalla 2024-04-06 A La(s) 0.37.53miguelangulo63557No ratings yet
- Tubal Factor Infertility Tubal Factor Infertility: The Possible Effect of Hydrosalpinx Fluid Human EmbryosDocument15 pagesTubal Factor Infertility Tubal Factor Infertility: The Possible Effect of Hydrosalpinx Fluid Human EmbryosWaode RadmilaNo ratings yet
- Endometriosis and Human InfertilityDocument8 pagesEndometriosis and Human InfertilityUmaimah ShahabNo ratings yet
- Histopatología Testiculo VenenoDocument14 pagesHistopatología Testiculo VenenodborghiNo ratings yet
- Anti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsDocument14 pagesAnti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsSri IriantiNo ratings yet
- Ultrasound Assessment of The Polycystic Ovary: International Consensus De®nitionsDocument10 pagesUltrasound Assessment of The Polycystic Ovary: International Consensus De®nitionsArkhan HanafiNo ratings yet
- Histopathological Variations in Ameloblastoma - Cases in A Tertiary Care Center of NepalDocument7 pagesHistopathological Variations in Ameloblastoma - Cases in A Tertiary Care Center of NepalDinesh YadavNo ratings yet
- Endometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersFrom EverandEndometrial Gene Expression: An Emerging Paradigm for Reproductive DisordersJoanne Kwak-KimNo ratings yet
- Bum Run GradDocument10 pagesBum Run GradsabyasachiNo ratings yet
- BioinfusionDocument2 pagesBioinfusionapi-455767165No ratings yet
- 3) Donor Information and Education Strategies..MMVDocument22 pages3) Donor Information and Education Strategies..MMVMaica Gee100% (1)
- The Use of Pycnogenol in The Treatment of Melasma: Original ArticlesDocument5 pagesThe Use of Pycnogenol in The Treatment of Melasma: Original Articlesfreitasjonashenrique100% (1)
- Bio InstrumentationDocument424 pagesBio Instrumentationwavestar100% (1)
- General Nursing Procedures-1Document92 pagesGeneral Nursing Procedures-1Asare PrinceNo ratings yet
- Ssi Rabu, 29 Juni 2022Document49 pagesSsi Rabu, 29 Juni 2022Dhamar SetiaNo ratings yet
- M Sandamela Salivary Gland SandamelaDocument45 pagesM Sandamela Salivary Gland SandamelaRockson SamuelNo ratings yet
- Occlusal Consideration in Implant ProsthesisDocument59 pagesOcclusal Consideration in Implant ProsthesisDrFarha NazNo ratings yet
- Elc590 PS Outline SampleDocument5 pagesElc590 PS Outline SampleHumaira Saffiya100% (1)
- Narcotic Drug Act 2033Document31 pagesNarcotic Drug Act 2033Dinesh YadavNo ratings yet
- National Medical Centre Tel: 021-35380000-3 UAN.111-222-NMCDocument1 pageNational Medical Centre Tel: 021-35380000-3 UAN.111-222-NMCImran MemonNo ratings yet
- Connective TissueDocument5 pagesConnective TissuePia AbilaNo ratings yet
- Hon 2005Document5 pagesHon 2005lenirizkiNo ratings yet
- Budget and PlannDocument15 pagesBudget and PlannJoe Sabia67% (3)
- 2nd Peroxisome Metabolism 20760414Document56 pages2nd Peroxisome Metabolism 20760414Rawbeena RamtelNo ratings yet
- The Effect of Closed Kinetic Chain Exercises And.14Document7 pagesThe Effect of Closed Kinetic Chain Exercises And.14fgomez235No ratings yet
- Common Breast DiseasesDocument64 pagesCommon Breast Diseasesamirahmei100% (1)
- Urinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byDocument13 pagesUrinary Retentio Ec. Suspect BPH Hernia Scrotalis Dextra: Consultant: Dr. Ninoy Mailoa, SP.B byCentia PicalNo ratings yet
- Performance Improvement Plan 2011-2012Document7 pagesPerformance Improvement Plan 2011-2012psynpNo ratings yet
- Acupuncture: M. Kay Garcia and Joseph S. ChiangDocument1 pageAcupuncture: M. Kay Garcia and Joseph S. ChiangFaith Acu CureNo ratings yet
- K.Hema Anandhy, M.SC Nursing, PuducherryDocument53 pagesK.Hema Anandhy, M.SC Nursing, PuducherryhemihemaNo ratings yet
- 2016 Media GuideDocument125 pages2016 Media GuideFC DallasNo ratings yet
- ICRC 2014 Healthcare in DetentionDocument100 pagesICRC 2014 Healthcare in DetentionJoseOrlandoRosales100% (1)
- Ipo 21 1 034Document3 pagesIpo 21 1 034Y.rajuNo ratings yet
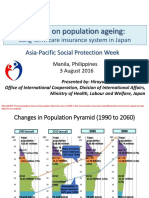
- APSP - Session 9A - Hiroyuki Yamaya - MHLWDocument8 pagesAPSP - Session 9A - Hiroyuki Yamaya - MHLWKristine PresbiteroNo ratings yet