Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Vaccine Debate by Jennifer MargulisDocument21 pagesVaccine Debate by Jennifer Margulisv2vreader100% (1)
- Health Assessment Long Answer QuestionsDocument11 pagesHealth Assessment Long Answer QuestionsSraddha Patel50% (2)
- Management of CADDocument99 pagesManagement of CADUmesh BabuNo ratings yet
- LabetalolDocument2 pagesLabetalolUmesh BabuNo ratings yet
- Order Details PDFDocument1 pageOrder Details PDFUmesh BabuNo ratings yet
- Tetanus Information For Health Professionals 2019Document26 pagesTetanus Information For Health Professionals 2019Umesh BabuNo ratings yet
- 10 CR Killian Jamieson DiverticulumDocument2 pages10 CR Killian Jamieson DiverticulumUmesh BabuNo ratings yet
- 05 Oa Effect of LowDocument4 pages05 Oa Effect of LowUmesh BabuNo ratings yet
- 08 PC Klebsiella BacteremiaDocument1 page08 PC Klebsiella BacteremiaUmesh BabuNo ratings yet
- 13 Piid Pioneers in InfectionDocument2 pages13 Piid Pioneers in InfectionUmesh BabuNo ratings yet
- Disorders of Potassium BalanceDocument41 pagesDisorders of Potassium BalanceUmesh BabuNo ratings yet
- Chelating AgentsDocument26 pagesChelating AgentsUmesh BabuNo ratings yet
- Women With Epilepsy inDocument4 pagesWomen With Epilepsy inUmesh BabuNo ratings yet
- Japi 07.2015Document73 pagesJapi 07.2015Umesh BabuNo ratings yet
- Respiratory Disorders and Disease: Chapter 6 Passage2Document31 pagesRespiratory Disorders and Disease: Chapter 6 Passage2Umesh BabuNo ratings yet
- Epilepsy - Japi UpdateDocument59 pagesEpilepsy - Japi UpdateUmesh BabuNo ratings yet
- Clinical Approach To QuadriplegiaDocument11 pagesClinical Approach To QuadriplegiaUmesh BabuNo ratings yet
- Pitfalls in Outpatient Diabetes Management and Inpatient Glycemic ControlDocument7 pagesPitfalls in Outpatient Diabetes Management and Inpatient Glycemic ControlUmesh BabuNo ratings yet
- Jurnal GeriatriDocument4 pagesJurnal GeriatrimaxNo ratings yet
- Aravind Eye Hospital, Madurai, IndiaDocument8 pagesAravind Eye Hospital, Madurai, IndiaArka Mitra100% (2)
- Coronavirus: Say True or False Answer The Following QuestionsDocument1 pageCoronavirus: Say True or False Answer The Following QuestionsMARIONo ratings yet
- ZXVZXCVZDocument1 pageZXVZXCVZjoycechicagoNo ratings yet
- Management of Odontogenic Infection of Primary Teeth in Child That Extends To The Submandibular and Submental Space Case ReportDocument5 pagesManagement of Odontogenic Infection of Primary Teeth in Child That Extends To The Submandibular and Submental Space Case ReportMel FANo ratings yet
- BME-02 Initial Testing and EvaluationDocument2 pagesBME-02 Initial Testing and EvaluationPAPPU RANJITH KUMARNo ratings yet
- Lumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuDocument38 pagesLumbar Strain: Dr. Lipy Bhat PT Faculty, Physiotherapy SrhuKapil LakhwaraNo ratings yet
- Arogya Sanjeevani PremiumDocument16 pagesArogya Sanjeevani PremiumGiriMahaNo ratings yet
- Pharmacy Guidelines 2Document2 pagesPharmacy Guidelines 2Inas IbrahimNo ratings yet
- Annamalai University: Faculty of MedicineDocument12 pagesAnnamalai University: Faculty of MedicineDeva JCNo ratings yet
- Form Pg-Sga PDFDocument2 pagesForm Pg-Sga PDFzain syalsabilaNo ratings yet
- Idaho Medical Marijuana Act of 2022Document11 pagesIdaho Medical Marijuana Act of 2022Marijuana MomentNo ratings yet
- Drug Study AMIODARONE & PROPOFOLDocument3 pagesDrug Study AMIODARONE & PROPOFOLNIKKI CARYL ZAFRANo ratings yet
- Phillipine Herbal MedicineDocument23 pagesPhillipine Herbal MedicineCENTHREE MAGALLANESNo ratings yet
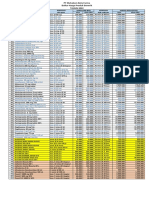
- Daftar Harga Produk Generik 2022 New (DITEMPEL)Document1 pageDaftar Harga Produk Generik 2022 New (DITEMPEL)Ade IrawanNo ratings yet
- Fabian 2Document6 pagesFabian 2przy3_14No ratings yet
- Tumor Mass - Petrovic, Jukovic... 2022Document3 pagesTumor Mass - Petrovic, Jukovic... 2022Mirela JukovicNo ratings yet
- Obstetric EmbolismDocument81 pagesObstetric Embolismmiss_izzniNo ratings yet
- Skripsi Tanpa Bab PembahasanDocument67 pagesSkripsi Tanpa Bab PembahasanUpitFlowNo ratings yet
- Treatment of Orthostatic and Postprandial Hypotension - UpToDateDocument25 pagesTreatment of Orthostatic and Postprandial Hypotension - UpToDateCipriano Di MauroNo ratings yet
- Alcohol Binge Drinking in OCDDocument2 pagesAlcohol Binge Drinking in OCDSuyash DwivediNo ratings yet
- Note On PainDocument6 pagesNote On Painbuhari rabiuNo ratings yet
- Amandaresume 1Document2 pagesAmandaresume 1api-510011907No ratings yet
- Criticool-Management of Temperature During and After Cardiac Surgery PDFDocument4 pagesCriticool-Management of Temperature During and After Cardiac Surgery PDFMrunali PatilNo ratings yet
- Home Epley HandoutsDocument4 pagesHome Epley HandoutsJohn OoNo ratings yet
- Delmar Cengage Learning Companions - Nursing Fundamentals - Caring & Clinical Decision MakingDocument3 pagesDelmar Cengage Learning Companions - Nursing Fundamentals - Caring & Clinical Decision MakingjjjNo ratings yet
- Nowledge, Attitude, and Practices Related To Cutaneous Leishmaniasis in An Endemic Focus of Cutaneous Leishmaniasis, Outhern RanDocument4 pagesNowledge, Attitude, and Practices Related To Cutaneous Leishmaniasis in An Endemic Focus of Cutaneous Leishmaniasis, Outhern RanDani Yitu MedanituNo ratings yet
- Roadmap For 2023 - 2030Document18 pagesRoadmap For 2023 - 2030creativejoburg100% (1)