Download as pptx, pdf, or txt
You might also like
- Healthy Choices Healthy Living: Talking About CancerDocument15 pagesHealthy Choices Healthy Living: Talking About CancerStarboyNo ratings yet
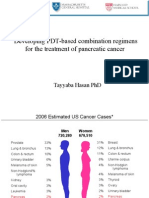
- Developing PDT-based Combination Regimens For The Treatment of Pancreatic CancerDocument33 pagesDeveloping PDT-based Combination Regimens For The Treatment of Pancreatic CancerFirdosh DekhaiyaNo ratings yet
- Healthy Choices Healthy Living: Talking About CancerDocument15 pagesHealthy Choices Healthy Living: Talking About CancerMila MarkovskaNo ratings yet
- Oncology 101: Cancer BasicsDocument74 pagesOncology 101: Cancer BasicsMary Rose Jose GragasinNo ratings yet
- Kanker Payudara: Epidemiologi Penyebab Dan Faktor Resiko Gejala Dan Tanda Stadium Tindak LanjutDocument46 pagesKanker Payudara: Epidemiologi Penyebab Dan Faktor Resiko Gejala Dan Tanda Stadium Tindak LanjutAulia DYAH FEBRIANTINo ratings yet
- En Neoplasia5 KulkaDocument62 pagesEn Neoplasia5 KulkaKevin IpuzNo ratings yet
- DR - Gorijavolu Durgaprasad, DR - Juturu PrasanthiDocument6 pagesDR - Gorijavolu Durgaprasad, DR - Juturu PrasanthiFrankly VRHNo ratings yet
- 5000 Most Common WordsDocument55 pages5000 Most Common WordsChoi DongYiNo ratings yet
- Lecture 11-Common Solid TumorsDocument57 pagesLecture 11-Common Solid TumorsAliArabiNo ratings yet
- Kanker Growtf Factor Dan Tirosin KinaseDocument142 pagesKanker Growtf Factor Dan Tirosin KinaseNovi KhamiliaNo ratings yet
- Breast Cancer ReviewDocument101 pagesBreast Cancer ReviewByron Orlando Sanchez RomeroNo ratings yet
- Pancreas CancerDocument66 pagesPancreas CancerPaulo Henrique Haß FilhoNo ratings yet
- Materi Prof Andri - Kanker ServiksDocument58 pagesMateri Prof Andri - Kanker ServiksAnonymous WXQKCLL3No ratings yet
- Early Detection of Breast Cancer Oleh DR EnosDocument78 pagesEarly Detection of Breast Cancer Oleh DR EnosKaka SlengNo ratings yet
- L13 OncologyDocument42 pagesL13 OncologyHengkai NeoNo ratings yet
- Clinical Manifestations, Diagnosis, and Staging of Exocrine Pancreatic Cancer - UpToDateDocument59 pagesClinical Manifestations, Diagnosis, and Staging of Exocrine Pancreatic Cancer - UpToDateVinicius VieiraNo ratings yet
- Lesson 4: Virtual Lab: Cell Reproduction: How Can Cancer Cells Be Recognized?Document2 pagesLesson 4: Virtual Lab: Cell Reproduction: How Can Cancer Cells Be Recognized?Minh Nguyen DucNo ratings yet
- CancerDocument22 pagesCancerPATRICK MARK FLORESNo ratings yet
- Colorectal Carcinoma-Anatomy To Management: by Dr. Ayush GargDocument99 pagesColorectal Carcinoma-Anatomy To Management: by Dr. Ayush Gargckyew64No ratings yet
- An Introduction To CancerDocument42 pagesAn Introduction To CancerAmjadRashidNo ratings yet
- Pancreascancer 140820083912 Phpapp01Document55 pagesPancreascancer 140820083912 Phpapp01enam professorNo ratings yet
- About Pancreatic CancerDocument8 pagesAbout Pancreatic Cancersummerland_5No ratings yet
- Epidemiology of CancerDocument2 pagesEpidemiology of CancerLilian LópezNo ratings yet
- 17 Educating Youth Presentation 1Document15 pages17 Educating Youth Presentation 1genellemaarteNo ratings yet
- Cervix Uteri: Source: Globocan 2020Document2 pagesCervix Uteri: Source: Globocan 2020nour abdallaNo ratings yet
- BooDocument2 pagesBooabubakkarahmedNo ratings yet
- Serial No. Types of C 1 Skin Cance 2 Breast Can 3 Lungs Canc 4 Cervical Ca 5 Colorectal 6 Blood Canc 7 Gastric Can 8 Brain Canc 9 EsophagealDocument2 pagesSerial No. Types of C 1 Skin Cance 2 Breast Can 3 Lungs Canc 4 Cervical Ca 5 Colorectal 6 Blood Canc 7 Gastric Can 8 Brain Canc 9 EsophagealabubakkarahmedNo ratings yet
- Neoplaziile Colonice: Lucian NegreanuDocument55 pagesNeoplaziile Colonice: Lucian NegreanuLeonte AncutaNo ratings yet
- Uncontrolled Cell Division: CancerDocument35 pagesUncontrolled Cell Division: Cancerkingkola36No ratings yet
- Answers To The Journal QuestionsDocument1 pageAnswers To The Journal QuestionsDaniel LinoNo ratings yet
- Globocan Lung CancerDocument2 pagesGlobocan Lung CancerAlexander AdrielNo ratings yet
- Kolorektal & Anus: Dr. Yusmaidi, SP.BDocument104 pagesKolorektal & Anus: Dr. Yusmaidi, SP.BAsmorowatiNo ratings yet
- 8 - Gynecological CancersDocument98 pages8 - Gynecological CancersAlexa RodriguezNo ratings yet
- Colorectal Carcinoma: Colorectal Carcinoma (CRC) Is The Most Common Cancer of The Gastrointestinal Tract and TheDocument14 pagesColorectal Carcinoma: Colorectal Carcinoma (CRC) Is The Most Common Cancer of The Gastrointestinal Tract and TheYTNo ratings yet
- Stomach: Source: Globocan 2020Document2 pagesStomach: Source: Globocan 2020Hizba RidhakaNo ratings yet
- National Cancer Control Programmes in ThailandDocument93 pagesNational Cancer Control Programmes in ThailandIndonesian Journal of CancerNo ratings yet
- O BGYNDocument84 pagesO BGYNselvie87100% (2)
- Screening Leaders Outreach LectureDocument40 pagesScreening Leaders Outreach LecturekishorechandraNo ratings yet
- 20 Breast Fact SheetDocument2 pages20 Breast Fact Sheetyuliaindahp18No ratings yet
- Ultrasound Screening and Diagnosis of PASDDocument54 pagesUltrasound Screening and Diagnosis of PASDKartika AdhitaNo ratings yet
- 4 Esophagus 2018Document55 pages4 Esophagus 2018a20-0353-958No ratings yet
- Intraductal Papillary Carcinoma Payudara: Temuan Pada Pencitraan UltrasonografiDocument6 pagesIntraductal Papillary Carcinoma Payudara: Temuan Pada Pencitraan UltrasonografiBastiaanNo ratings yet
- Carcinoma StomachDocument128 pagesCarcinoma StomachAnoop TNo ratings yet
- Tumor Saluran Cerna AtasDocument85 pagesTumor Saluran Cerna Atasnawal asmadiNo ratings yet
- Kanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangDocument32 pagesKanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangRakhmiNo ratings yet
- Prof - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical CollegeDocument79 pagesProf - Amer Eltwati Ben Irhuma Consultant Surgeon Sebha Medical Collegeckyew64100% (1)
- 6 Oesophagus Fact SheetDocument2 pages6 Oesophagus Fact SheetHizba RidhakaNo ratings yet
- Emory Reynolds Program Colon Cancer Resource ModuleDocument45 pagesEmory Reynolds Program Colon Cancer Resource ModulealbertontaolaNo ratings yet
- Acute Pancreatic RGB 2023Document16 pagesAcute Pancreatic RGB 2023NohemaVMNo ratings yet
- Kuliah Kelainan PayudaraDocument44 pagesKuliah Kelainan PayudaradewiswahyuNo ratings yet
- Passmrcog Patho, Embryo 2016Document171 pagesPassmrcog Patho, Embryo 2016Mona HelouNo ratings yet
- CancerDocument15 pagesCancerAficionadoNo ratings yet
- Breast Cancer: MembersDocument15 pagesBreast Cancer: MembersEstefany LopezNo ratings yet
- Kara CancerDocument45 pagesKara CancerLinux MintNo ratings yet
- Periampullary CarcinomaDocument35 pagesPeriampullary Carcinomaminnalesri100% (2)
- Ca MammaeDocument43 pagesCa MammaeAnonymous F0eeZBMKNo ratings yet
- Pancreatic Cancer: by Moaz MehboobDocument18 pagesPancreatic Cancer: by Moaz MehboobMUHAMMAD HAMZA IRSHADNo ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document30 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- (GYNE) Neoplastic Diseases of The Ovary-Dr. Dueñas (Parbs)Document10 pages(GYNE) Neoplastic Diseases of The Ovary-Dr. Dueñas (Parbs)adrian kristopher dela cruzNo ratings yet
- Breast Cancer Rehabilitation: A Critical Review of Clinical Practice Guidelines and Evidence-Based Medicine in LiteratureDocument10 pagesBreast Cancer Rehabilitation: A Critical Review of Clinical Practice Guidelines and Evidence-Based Medicine in LiteratureDeborah SalinasNo ratings yet
- Transformation and Oncogenesis: Biology W3310/4310 Virology Spring 2016Document56 pagesTransformation and Oncogenesis: Biology W3310/4310 Virology Spring 2016kashif manzoorNo ratings yet
- 500 Medical Surgical Sample QuestionDocument323 pages500 Medical Surgical Sample QuestionElizabella Henrietta TanaquilNo ratings yet
- Test Bank For Pathology For The Physical Therapist Assistant 1st Edition by GoodmanDocument5 pagesTest Bank For Pathology For The Physical Therapist Assistant 1st Edition by GoodmanCheryl Lott100% (37)
- Ebook Eliminate Cancers Favorite Building Block Ty Bollinger TTAC PDFDocument32 pagesEbook Eliminate Cancers Favorite Building Block Ty Bollinger TTAC PDFmilanmanijakNo ratings yet
- Types of Ovarian CancerDocument5 pagesTypes of Ovarian Cancerوسام وميض عبدالله CNo ratings yet
- Replay TamplatesDocument23 pagesReplay TamplatesDhiraj PalNo ratings yet
- In Pa Števila in Protokol Za Zdravljenje Določene BolezniDocument26 pagesIn Pa Števila in Protokol Za Zdravljenje Določene BolezniImmortal Suzy Q100% (2)
- GL Principles and Practice of PET-CT Part 1Document101 pagesGL Principles and Practice of PET-CT Part 1Alejandra CorkNo ratings yet
- Basic and Clinical Endocrinology Up-To-DateDocument360 pagesBasic and Clinical Endocrinology Up-To-DateIrina Isac0% (1)
- 180 Critical IllnessDocument7 pages180 Critical IllnessAudrey ThenNo ratings yet
- Over Coming Can Cer: Books by Ian GawlerDocument2 pagesOver Coming Can Cer: Books by Ian Gawlersimonramon177907No ratings yet
- Death by Diet - Barefoot, Robert RDocument228 pagesDeath by Diet - Barefoot, Robert RAnonymous gwFqQcnaX100% (5)
- Week 1 Health Determinents 122Document27 pagesWeek 1 Health Determinents 122maureen njeruNo ratings yet
- Zimbabwe - Medical - CPIN - v2.0 - GOV - UKDocument39 pagesZimbabwe - Medical - CPIN - v2.0 - GOV - UKsammy redganjiNo ratings yet
- Maltepe University International Student Congress Medicine 2019Document4 pagesMaltepe University International Student Congress Medicine 2019Sezen YılmazNo ratings yet
- BoneDocument5 pagesBoneTaha IsmailNo ratings yet
- Aghamohammadi Et Al 2016 WEB OF SCIENCE Integrative Cancer TherapiesDocument9 pagesAghamohammadi Et Al 2016 WEB OF SCIENCE Integrative Cancer Therapiesemmanuelle leal capelliniNo ratings yet
- Wa0004.Document20 pagesWa0004.Mayra AlejandraNo ratings yet
- Guidelines For Surgery in The HIV Patient: Samuel Smit, MB CHB, M Med (Surg)Document8 pagesGuidelines For Surgery in The HIV Patient: Samuel Smit, MB CHB, M Med (Surg)Afkar30No ratings yet
- Breast Case ProformaDocument2 pagesBreast Case ProformaSyed FirdozNo ratings yet
- Psycho-Oncology - 2018 - Holland - Psycho Oncology Overview Obstacles and OpportunitiesDocument13 pagesPsycho-Oncology - 2018 - Holland - Psycho Oncology Overview Obstacles and OpportunitiesRegina100% (1)
- Radiobiology DilshadDocument78 pagesRadiobiology DilshadAJAY K VNo ratings yet
- Decade Report Full Report Final-LinkedDocument250 pagesDecade Report Full Report Final-LinkedJosh Arno M SilitongaNo ratings yet
- Cancer Pain Management Literature ReviewDocument7 pagesCancer Pain Management Literature Reviewfvg2005k100% (1)
- Arnold Devries-Therapeutic Fasting (1963)Document48 pagesArnold Devries-Therapeutic Fasting (1963)Silambarasu KaruppiahNo ratings yet
- The Spiritual Nurse: Lasherr'E Osborne 2/8/2015 Article EvaluationDocument3 pagesThe Spiritual Nurse: Lasherr'E Osborne 2/8/2015 Article EvaluationLaSherreNo ratings yet
- CHOLANGIOCARCINOMADocument26 pagesCHOLANGIOCARCINOMAPremaKurnia100% (3)
- CancerDocument41 pagesCancerMae Usquisa0% (1)
- Malignant Diseases of The CervixDocument128 pagesMalignant Diseases of The Cervixnicewan0% (1)