
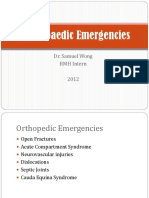
Complications of Fractures
Complications of Fractures
You might also like
- Complication of FractureDocument38 pagesComplication of FractureAshok BalwadaNo ratings yet
- Care of WoundDocument29 pagesCare of WoundAllan NEIGRIHMS80% (5)
- Complications of Multiple FracturesDocument35 pagesComplications of Multiple Fractureshello from the other sideNo ratings yet
- Complications of FracturesDocument29 pagesComplications of FracturesAlina Panciuc100% (1)
- CX of Fractures and DislocationsDocument68 pagesCX of Fractures and Dislocationsحسين سعد عبدالمهدي الوائليNo ratings yet
- Complication of Fractuers PART 1Document34 pagesComplication of Fractuers PART 1203190085.gNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic Injuriesamber tariqNo ratings yet
- (Upgraded) Complications of Fractures and ManagementDocument65 pages(Upgraded) Complications of Fractures and ManagementroroNo ratings yet
- Sss Orthopedicemergencies 2012 Final Samuel-WongDocument38 pagesSss Orthopedicemergencies 2012 Final Samuel-WongMuhammad Irham FananiNo ratings yet
- Complications of Fractures and ManagementDocument65 pagesComplications of Fractures and ManagementSemestaNo ratings yet
- Complicationsoffractures 120127084025 Phpapp02Document62 pagesComplicationsoffractures 120127084025 Phpapp02Aaliyah ShaikhNo ratings yet
- 5-Fracture 3fDocument22 pages5-Fracture 3fRadwa TalaatNo ratings yet
- Orthopedic EmergenciesDocument63 pagesOrthopedic EmergenciesNasser AlQadhibNo ratings yet
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Complications of FractureDocument19 pagesComplications of FractureEsome Sharma100% (1)
- COMPARTMENT SYNDROMEv FinalDocument56 pagesCOMPARTMENT SYNDROMEv Finalbhavikaagarwal07No ratings yet
- Orthopedic EmergencyDocument94 pagesOrthopedic EmergencyZenith100% (1)
- 2 - Local Complications of Fractures - D3Document26 pages2 - Local Complications of Fractures - D3Zainul FatimahNo ratings yet
- Complications of FracturesDocument68 pagesComplications of FracturesChenna Kesava100% (1)
- Orthopedic Emergency EnglishDocument64 pagesOrthopedic Emergency EnglishmegaNo ratings yet
- AMPUTATIONDocument73 pagesAMPUTATIONmohammad farhanNo ratings yet
- Notes On AmputationsDocument3 pagesNotes On AmputationsShaileeNo ratings yet
- Orthopaedics Prof Exam November 2019Sarah1439C1Document12 pagesOrthopaedics Prof Exam November 2019Sarah1439C1Navid BabluNo ratings yet
- Bone Healing, Complications, Compartment SyndromeDocument94 pagesBone Healing, Complications, Compartment SyndromenhfbyqvgwhNo ratings yet
- نسخة Blood 1Document29 pagesنسخة Blood 1KyunaNo ratings yet
- Complicationsoffractures 120127084025 Phpapp02Document51 pagesComplicationsoffractures 120127084025 Phpapp02Pradeep KothadiaNo ratings yet
- Complications of FracturesDocument18 pagesComplications of Fracturesallthingali217No ratings yet
- 3 Complications of FracturesDocument101 pages3 Complications of Fracturesq77gkyhzs4No ratings yet
- Compartment SyndromeDocument13 pagesCompartment SyndromebismahNo ratings yet
- 2 - Vascular InjuryDocument6 pages2 - Vascular Injuryمحمد عماد عليNo ratings yet
- Orthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SDocument17 pagesOrthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SlanghalilafaNo ratings yet
- Aracnoditis PDFDocument18 pagesAracnoditis PDFArockia Albert JerosonNo ratings yet
- Compartment Syndrome AndreDocument40 pagesCompartment Syndrome AndreOlivia Christy KaihatuNo ratings yet
- Muscloskeletal System (Disorders) .Document27 pagesMuscloskeletal System (Disorders) .Younas BhattiNo ratings yet
- Complications of FracturesDocument19 pagesComplications of Fracturesمحمد رأفتNo ratings yet
- Dr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010Document53 pagesDr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010yuliaoksiyulanda ingeniopadangNo ratings yet
- Surgery On Vessels and Nerfs 2020Document49 pagesSurgery On Vessels and Nerfs 2020Timbur IgorNo ratings yet
- Compartment SyndromeDocument67 pagesCompartment SyndromeashokNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeKezia TambunanNo ratings yet
- Fracture Complications PDFDocument3 pagesFracture Complications PDFlemootpNo ratings yet
- Vascular Trauma: Episode OverviewDocument11 pagesVascular Trauma: Episode OverviewwatimelawatiNo ratings yet
- Orthopedic InjuriesDocument27 pagesOrthopedic InjuriesvikramNo ratings yet
- Compartment Syndrome ForearmDocument2 pagesCompartment Syndrome ForearmHein Aung ZawNo ratings yet
- Spinal Cord InjuryDocument13 pagesSpinal Cord Injurypaul_allan17No ratings yet
- MCQ DegenerationDocument4 pagesMCQ Degenerationdrng48No ratings yet
- Clinical Features and Diagnosis of FracturesDocument43 pagesClinical Features and Diagnosis of FracturesChenna Kesava100% (2)
- Lecture 1&2Document10 pagesLecture 1&2Irfan NashadNo ratings yet
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Complications of FractureDocument40 pagesComplications of Fracturemohammad farhanNo ratings yet
- Tareq MH Bu SalehDocument38 pagesTareq MH Bu Salehloya4everNo ratings yet
- Unit 4 Nursing Care of Clients With Musculoskeletal DisordersDocument100 pagesUnit 4 Nursing Care of Clients With Musculoskeletal DisordersE. Tito Julianda SinagaNo ratings yet
- Ompartment Syndrome: DR. Karrar Abdul Sattar Jaber Orthopedic Surgeon Arabic & Iraqi Board F.A.C.M.S - F.I.C.M.SDocument13 pagesOmpartment Syndrome: DR. Karrar Abdul Sattar Jaber Orthopedic Surgeon Arabic & Iraqi Board F.A.C.M.S - F.I.C.M.Sحسين رسول ناجيNo ratings yet
- Bone FractureDocument25 pagesBone FractureDaramola JuwonNo ratings yet
- Fat Embolism and Compartment SyndromeDocument19 pagesFat Embolism and Compartment SyndromeAbdulsalam DostNo ratings yet
- Week 10 - Hypertension, Atherosclerosis, ArrhythmiaDocument14 pagesWeek 10 - Hypertension, Atherosclerosis, Arrhythmiashivani patel100% (1)
- Ulcers, The Diabetic FootDocument10 pagesUlcers, The Diabetic FootmuhammadridhwanNo ratings yet
- JOINTS2Document61 pagesJOINTS2api-19916399No ratings yet
- Diagnostic Imaging - 12 - Regional Pathologies and Evaluation - Tendon - Muscle - Cartilage - Nerve - Prof - Dr.i̇smet TAMERDocument18 pagesDiagnostic Imaging - 12 - Regional Pathologies and Evaluation - Tendon - Muscle - Cartilage - Nerve - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Kompartemen SindromDocument9 pagesKompartemen SindromPutri PratiwiNo ratings yet
- 2016 Psychaitric Nursing Problem StatementsDocument10 pages2016 Psychaitric Nursing Problem StatementsMAHESH KOUJALAGI100% (1)
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- SDL R VS OldDocument6 pagesSDL R VS Oldsejal3vijNo ratings yet
- SIM ScienceDocument37 pagesSIM ScienceEllech YamNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Chlamydia TrachomatisDocument7 pagesChlamydia TrachomatisDewi SetiawatiNo ratings yet
- 2020 Journal Basic and Clinical Physiology and PharmacologyDocument10 pages2020 Journal Basic and Clinical Physiology and PharmacologytsamoNo ratings yet
- Why Is Development of New Treatments Necessary For Myasthenia Gravis? Recent Advances in Clinical TrialsDocument5 pagesWhy Is Development of New Treatments Necessary For Myasthenia Gravis? Recent Advances in Clinical TrialsRameshKrishnanNo ratings yet
- 11 Physical Education Chapter 12Document9 pages11 Physical Education Chapter 12Pankaj BroNo ratings yet
- Maternity Benefits Requirements DocsDocument2 pagesMaternity Benefits Requirements DocsGladys April CatarojaNo ratings yet
- Monika Fleckenstein Age Related Macular Degeneration ADocument11 pagesMonika Fleckenstein Age Related Macular Degeneration Afrwf8j7dr4No ratings yet
- Practice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelDocument4 pagesPractice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelSamprita DuttaNo ratings yet
- Levels of Critical Care For Adult Patients (ReviseDocument12 pagesLevels of Critical Care For Adult Patients (Revisejtsk2No ratings yet
- Ipap SchizDocument1 pageIpap SchizDragutin PetrićNo ratings yet
- Nutri Most H CL Whole Body DetoxDocument4 pagesNutri Most H CL Whole Body DetoxdeylafeisNo ratings yet
- Dr. Gupta Says, No One Must Die of Cancer Except Out of CarelessnessDocument2 pagesDr. Gupta Says, No One Must Die of Cancer Except Out of CarelessnessMyrelle Da Jose Sario0% (1)
- Dept of Molecular Biology and Cytogenetics Central - Laboratory, PBMH, KimsDocument1 pageDept of Molecular Biology and Cytogenetics Central - Laboratory, PBMH, KimsashishNo ratings yet
- Low Dose Dexamethasone Suppression TestDocument2 pagesLow Dose Dexamethasone Suppression Testsanham100% (1)
- Cross Sectional Imaging Nuclear Medicine: Dr. Leeann Pack Dipl. AcvrDocument51 pagesCross Sectional Imaging Nuclear Medicine: Dr. Leeann Pack Dipl. AcvrShashi BhushanNo ratings yet
- Tpuc 501Document4 pagesTpuc 501hairiNo ratings yet
- Unit 4 Word Circulatory SystemDocument26 pagesUnit 4 Word Circulatory SystemChandan Shah100% (2)
- ORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxDocument11 pagesORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxYvonne ChristieNo ratings yet
- Self-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaDocument13 pagesSelf-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaArif IrpanNo ratings yet
- Fetish Is MeDocument7 pagesFetish Is MeErna YuliantiNo ratings yet
- Published Shally IJARDocument8 pagesPublished Shally IJARJOSLINNo ratings yet
- CAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentDocument35 pagesCAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentAnonymous KgUtPlkjNo ratings yet
- OsteosarcomaDocument87 pagesOsteosarcomaCob CornNo ratings yet
- Pathogenesis and RX of CovidDocument11 pagesPathogenesis and RX of CovidYawer Yousuf100% (4)
- Brolucizumab in Neovascular Age Related Macular Degeneration and Diabetic Macular EdemaDocument17 pagesBrolucizumab in Neovascular Age Related Macular Degeneration and Diabetic Macular EdemaKang LimbaNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- Complication of FractureDocument38 pagesComplication of FractureAshok BalwadaNo ratings yet
- Care of WoundDocument29 pagesCare of WoundAllan NEIGRIHMS80% (5)
- Complications of Multiple FracturesDocument35 pagesComplications of Multiple Fractureshello from the other sideNo ratings yet
- Complications of FracturesDocument29 pagesComplications of FracturesAlina Panciuc100% (1)
- CX of Fractures and DislocationsDocument68 pagesCX of Fractures and Dislocationsحسين سعد عبدالمهدي الوائليNo ratings yet
- Complication of Fractuers PART 1Document34 pagesComplication of Fractuers PART 1203190085.gNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic Injuriesamber tariqNo ratings yet
- (Upgraded) Complications of Fractures and ManagementDocument65 pages(Upgraded) Complications of Fractures and ManagementroroNo ratings yet
- Sss Orthopedicemergencies 2012 Final Samuel-WongDocument38 pagesSss Orthopedicemergencies 2012 Final Samuel-WongMuhammad Irham FananiNo ratings yet
- Complications of Fractures and ManagementDocument65 pagesComplications of Fractures and ManagementSemestaNo ratings yet
- Complicationsoffractures 120127084025 Phpapp02Document62 pagesComplicationsoffractures 120127084025 Phpapp02Aaliyah ShaikhNo ratings yet
- 5-Fracture 3fDocument22 pages5-Fracture 3fRadwa TalaatNo ratings yet
- Orthopedic EmergenciesDocument63 pagesOrthopedic EmergenciesNasser AlQadhibNo ratings yet
- AmputationDocument51 pagesAmputationStar CruiseNo ratings yet
- Complications of FractureDocument19 pagesComplications of FractureEsome Sharma100% (1)
- COMPARTMENT SYNDROMEv FinalDocument56 pagesCOMPARTMENT SYNDROMEv Finalbhavikaagarwal07No ratings yet
- Orthopedic EmergencyDocument94 pagesOrthopedic EmergencyZenith100% (1)
- 2 - Local Complications of Fractures - D3Document26 pages2 - Local Complications of Fractures - D3Zainul FatimahNo ratings yet
- Complications of FracturesDocument68 pagesComplications of FracturesChenna Kesava100% (1)
- Orthopedic Emergency EnglishDocument64 pagesOrthopedic Emergency EnglishmegaNo ratings yet
- AMPUTATIONDocument73 pagesAMPUTATIONmohammad farhanNo ratings yet
- Notes On AmputationsDocument3 pagesNotes On AmputationsShaileeNo ratings yet
- Orthopaedics Prof Exam November 2019Sarah1439C1Document12 pagesOrthopaedics Prof Exam November 2019Sarah1439C1Navid BabluNo ratings yet
- Bone Healing, Complications, Compartment SyndromeDocument94 pagesBone Healing, Complications, Compartment SyndromenhfbyqvgwhNo ratings yet
- نسخة Blood 1Document29 pagesنسخة Blood 1KyunaNo ratings yet
- Complicationsoffractures 120127084025 Phpapp02Document51 pagesComplicationsoffractures 120127084025 Phpapp02Pradeep KothadiaNo ratings yet
- Complications of FracturesDocument18 pagesComplications of Fracturesallthingali217No ratings yet
- 3 Complications of FracturesDocument101 pages3 Complications of Fracturesq77gkyhzs4No ratings yet
- Compartment SyndromeDocument13 pagesCompartment SyndromebismahNo ratings yet
- 2 - Vascular InjuryDocument6 pages2 - Vascular Injuryمحمد عماد عليNo ratings yet
- Orthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SDocument17 pagesOrthopaedic Surgery Study Guide FOR Medical Students, R1S and R2SlanghalilafaNo ratings yet
- Aracnoditis PDFDocument18 pagesAracnoditis PDFArockia Albert JerosonNo ratings yet
- Compartment Syndrome AndreDocument40 pagesCompartment Syndrome AndreOlivia Christy KaihatuNo ratings yet
- Muscloskeletal System (Disorders) .Document27 pagesMuscloskeletal System (Disorders) .Younas BhattiNo ratings yet
- Complications of FracturesDocument19 pagesComplications of Fracturesمحمد رأفتNo ratings yet
- Dr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010Document53 pagesDr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010yuliaoksiyulanda ingeniopadangNo ratings yet
- Surgery On Vessels and Nerfs 2020Document49 pagesSurgery On Vessels and Nerfs 2020Timbur IgorNo ratings yet
- Compartment SyndromeDocument67 pagesCompartment SyndromeashokNo ratings yet
- Acute Limb Ischemia: Clinical PracticeDocument9 pagesAcute Limb Ischemia: Clinical PracticeKezia TambunanNo ratings yet
- Fracture Complications PDFDocument3 pagesFracture Complications PDFlemootpNo ratings yet
- Vascular Trauma: Episode OverviewDocument11 pagesVascular Trauma: Episode OverviewwatimelawatiNo ratings yet
- Orthopedic InjuriesDocument27 pagesOrthopedic InjuriesvikramNo ratings yet
- Compartment Syndrome ForearmDocument2 pagesCompartment Syndrome ForearmHein Aung ZawNo ratings yet
- Spinal Cord InjuryDocument13 pagesSpinal Cord Injurypaul_allan17No ratings yet
- MCQ DegenerationDocument4 pagesMCQ Degenerationdrng48No ratings yet
- Clinical Features and Diagnosis of FracturesDocument43 pagesClinical Features and Diagnosis of FracturesChenna Kesava100% (2)
- Lecture 1&2Document10 pagesLecture 1&2Irfan NashadNo ratings yet
- Complications of FracturesDocument13 pagesComplications of FracturesmilananandNo ratings yet
- Complications of FractureDocument40 pagesComplications of Fracturemohammad farhanNo ratings yet
- Tareq MH Bu SalehDocument38 pagesTareq MH Bu Salehloya4everNo ratings yet
- Unit 4 Nursing Care of Clients With Musculoskeletal DisordersDocument100 pagesUnit 4 Nursing Care of Clients With Musculoskeletal DisordersE. Tito Julianda SinagaNo ratings yet
- Ompartment Syndrome: DR. Karrar Abdul Sattar Jaber Orthopedic Surgeon Arabic & Iraqi Board F.A.C.M.S - F.I.C.M.SDocument13 pagesOmpartment Syndrome: DR. Karrar Abdul Sattar Jaber Orthopedic Surgeon Arabic & Iraqi Board F.A.C.M.S - F.I.C.M.Sحسين رسول ناجيNo ratings yet
- Bone FractureDocument25 pagesBone FractureDaramola JuwonNo ratings yet
- Fat Embolism and Compartment SyndromeDocument19 pagesFat Embolism and Compartment SyndromeAbdulsalam DostNo ratings yet
- Week 10 - Hypertension, Atherosclerosis, ArrhythmiaDocument14 pagesWeek 10 - Hypertension, Atherosclerosis, Arrhythmiashivani patel100% (1)
- Ulcers, The Diabetic FootDocument10 pagesUlcers, The Diabetic FootmuhammadridhwanNo ratings yet
- JOINTS2Document61 pagesJOINTS2api-19916399No ratings yet
- Diagnostic Imaging - 12 - Regional Pathologies and Evaluation - Tendon - Muscle - Cartilage - Nerve - Prof - Dr.i̇smet TAMERDocument18 pagesDiagnostic Imaging - 12 - Regional Pathologies and Evaluation - Tendon - Muscle - Cartilage - Nerve - Prof - Dr.i̇smet TAMERAly MssreNo ratings yet
- Kompartemen SindromDocument9 pagesKompartemen SindromPutri PratiwiNo ratings yet
- 2016 Psychaitric Nursing Problem StatementsDocument10 pages2016 Psychaitric Nursing Problem StatementsMAHESH KOUJALAGI100% (1)
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- SDL R VS OldDocument6 pagesSDL R VS Oldsejal3vijNo ratings yet
- SIM ScienceDocument37 pagesSIM ScienceEllech YamNo ratings yet
- 2 51 1656420123 1ijmpsdec20221Document4 pages2 51 1656420123 1ijmpsdec20221TJPRC PublicationsNo ratings yet
- Chlamydia TrachomatisDocument7 pagesChlamydia TrachomatisDewi SetiawatiNo ratings yet
- 2020 Journal Basic and Clinical Physiology and PharmacologyDocument10 pages2020 Journal Basic and Clinical Physiology and PharmacologytsamoNo ratings yet
- Why Is Development of New Treatments Necessary For Myasthenia Gravis? Recent Advances in Clinical TrialsDocument5 pagesWhy Is Development of New Treatments Necessary For Myasthenia Gravis? Recent Advances in Clinical TrialsRameshKrishnanNo ratings yet
- 11 Physical Education Chapter 12Document9 pages11 Physical Education Chapter 12Pankaj BroNo ratings yet
- Maternity Benefits Requirements DocsDocument2 pagesMaternity Benefits Requirements DocsGladys April CatarojaNo ratings yet
- Monika Fleckenstein Age Related Macular Degeneration ADocument11 pagesMonika Fleckenstein Age Related Macular Degeneration Afrwf8j7dr4No ratings yet
- Practice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelDocument4 pagesPractice Test: Biology: Body Fluids & Circulation For Live Session On 17-Nov-2018 On Neetprep Youtube ChannelSamprita DuttaNo ratings yet
- Levels of Critical Care For Adult Patients (ReviseDocument12 pagesLevels of Critical Care For Adult Patients (Revisejtsk2No ratings yet
- Ipap SchizDocument1 pageIpap SchizDragutin PetrićNo ratings yet
- Nutri Most H CL Whole Body DetoxDocument4 pagesNutri Most H CL Whole Body DetoxdeylafeisNo ratings yet
- Dr. Gupta Says, No One Must Die of Cancer Except Out of CarelessnessDocument2 pagesDr. Gupta Says, No One Must Die of Cancer Except Out of CarelessnessMyrelle Da Jose Sario0% (1)
- Dept of Molecular Biology and Cytogenetics Central - Laboratory, PBMH, KimsDocument1 pageDept of Molecular Biology and Cytogenetics Central - Laboratory, PBMH, KimsashishNo ratings yet
- Low Dose Dexamethasone Suppression TestDocument2 pagesLow Dose Dexamethasone Suppression Testsanham100% (1)
- Cross Sectional Imaging Nuclear Medicine: Dr. Leeann Pack Dipl. AcvrDocument51 pagesCross Sectional Imaging Nuclear Medicine: Dr. Leeann Pack Dipl. AcvrShashi BhushanNo ratings yet
- Tpuc 501Document4 pagesTpuc 501hairiNo ratings yet
- Unit 4 Word Circulatory SystemDocument26 pagesUnit 4 Word Circulatory SystemChandan Shah100% (2)
- ORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxDocument11 pagesORG7510 Monday 91145pm WK6 The Addiction Methodology of Bio Psychology CHRISTIEGYdocxYvonne ChristieNo ratings yet
- Self-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaDocument13 pagesSelf-Stigma and Medication Adherence Among Patients With Mental Illness Treated at Jimma University Medical Center, Southwest EthiopiaArif IrpanNo ratings yet
- Fetish Is MeDocument7 pagesFetish Is MeErna YuliantiNo ratings yet
- Published Shally IJARDocument8 pagesPublished Shally IJARJOSLINNo ratings yet
- CAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentDocument35 pagesCAGE Test Alcool, CAGE Test Droguri, Test AUDIT Pentru Alcoolism. Ce Este Adictia. Coping Si TratamentAnonymous KgUtPlkjNo ratings yet
- OsteosarcomaDocument87 pagesOsteosarcomaCob CornNo ratings yet
- Pathogenesis and RX of CovidDocument11 pagesPathogenesis and RX of CovidYawer Yousuf100% (4)
- Brolucizumab in Neovascular Age Related Macular Degeneration and Diabetic Macular EdemaDocument17 pagesBrolucizumab in Neovascular Age Related Macular Degeneration and Diabetic Macular EdemaKang LimbaNo ratings yet