Download as pptx, pdf, or txt
You might also like
- Joining PDFDocument22 pagesJoining PDFAndreea TanaseNo ratings yet
- Ruptur OASISDocument41 pagesRuptur OASISHen DriNo ratings yet
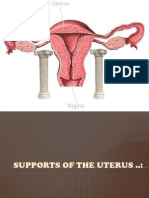
- Supports of The UterusDocument20 pagesSupports of The UterusAshwin Prem Solomon100% (1)
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
- Malignant Tumors of Uterus: DR Tahira RizwanDocument52 pagesMalignant Tumors of Uterus: DR Tahira RizwanSadia YousafNo ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiNo ratings yet
- PA Genitalia WanitaDocument100 pagesPA Genitalia WanitaBNo ratings yet
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Document559 pagesObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113No ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Twin PregnancyDocument73 pagesTwin Pregnancykrishna mandalNo ratings yet
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Spontaneous Vaginal Delivery IN Post Term PregnancyDocument55 pagesSpontaneous Vaginal Delivery IN Post Term Pregnancyr.pavinvikneshNo ratings yet
- Benign Gyecologic LesionDocument158 pagesBenign Gyecologic LesionArianne Joy C. TamarayNo ratings yet
- PCOS DR BasimaDocument18 pagesPCOS DR BasimaA.H.ANo ratings yet
- Abnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadDocument35 pagesAbnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadYazeed Asrawi0% (1)
- Topic AmenorrheaDocument23 pagesTopic AmenorrheaMohammed AbdulNo ratings yet
- Max Brinsmead MB Bs PHD May 2015Document15 pagesMax Brinsmead MB Bs PHD May 2015DrChauhan100% (1)
- Dystocia 2010Document55 pagesDystocia 2010Meigy NitalessyNo ratings yet
- Assisted Reproductive TechniquesDocument146 pagesAssisted Reproductive TechniquesGouravNo ratings yet
- Cervix Cancer Power Point With SlidesDocument41 pagesCervix Cancer Power Point With SlidesAmín JiménezNo ratings yet
- Abnormal Uterin ActionDocument65 pagesAbnormal Uterin Actionshweta raiNo ratings yet
- Abnormal Uterine Bleeding (AUB)Document45 pagesAbnormal Uterine Bleeding (AUB)asdf0% (1)
- Gynecological LaparosDocument32 pagesGynecological LaparosYosef Dwi Cahyadi Salan100% (1)
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasNo ratings yet
- Gyn & ObsDocument68 pagesGyn & ObsEsraa Almassri100% (1)
- Jaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TDocument35 pagesJaundice in Pregnancy: M2 - Fmbs DR Dohbit Sama Prof Mboudou E. TSerge TresorNo ratings yet
- Secondary AmenorrheaDocument18 pagesSecondary AmenorrheaMaria Gill100% (1)
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Menstrual Disorder and Abnormal BleedingDocument9 pagesMenstrual Disorder and Abnormal Bleedingdr_asalehNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Thromboembolic Disease in Pregnancy د.علية شعيبDocument50 pagesThromboembolic Disease in Pregnancy د.علية شعيبMohammad Belbahaith0% (1)
- Reproductive Endocrinology FinalDocument98 pagesReproductive Endocrinology FinalChino Paolo SamsonNo ratings yet
- Endometrial Hyperplasia: by Dr. Mervat AliDocument48 pagesEndometrial Hyperplasia: by Dr. Mervat AliAsh Ame100% (1)
- Benign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDocument83 pagesBenign & Precancerous Tumors of Female Genital Organs: by Assist. O.V.BakunDian Permata PutraNo ratings yet
- Early Pregnancy Problems: Presented byDocument28 pagesEarly Pregnancy Problems: Presented byMalk OmryNo ratings yet
- Mullarian AnomoliesDocument85 pagesMullarian AnomoliesPrathibha GuruguriNo ratings yet
- Early Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelDocument60 pagesEarly Pregnancy Complications: Ectopic Pregnancy Gestational Trophoblastic Disease Ji Aggasid, JanniecelmedicoNo ratings yet
- Ob - Operative ObstetricsDocument224 pagesOb - Operative Obstetricsapi-385605133% (3)
- Fertilisasi Askeb IDocument19 pagesFertilisasi Askeb IPutry Utami0% (1)
- Benign and Malignant Ovarian Tumors: Case 1Document14 pagesBenign and Malignant Ovarian Tumors: Case 1Charrie RagadiNo ratings yet
- FIGO Guidelines - Prevention and Treatment of PPH Etc1Document12 pagesFIGO Guidelines - Prevention and Treatment of PPH Etc1karinasurakusumaNo ratings yet
- Caesarean Scar Ectopic Pregnancy: Case ReportDocument3 pagesCaesarean Scar Ectopic Pregnancy: Case ReportDewi SaftariNo ratings yet
- Male InfertilityDocument57 pagesMale InfertilityUsha AnengaNo ratings yet
- Pap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.DDocument22 pagesPap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.Dshygirl72No ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Infertilityseminarppt 190718134710Document77 pagesInfertilityseminarppt 190718134710subiNo ratings yet
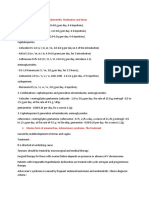
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Hypertension in Pregnancy PoltekesDocument41 pagesHypertension in Pregnancy PoltekesKhoerunnisa SeptianiNo ratings yet
- PuerperiumDocument16 pagesPuerperiumMohammed AbdNo ratings yet
- Polycystic Ovarian Syndrome: Dr. PrabhavathiDocument30 pagesPolycystic Ovarian Syndrome: Dr. PrabhavathiKasi PrasadNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- MRCOG Part 2 - March 2015 Recalls.: StatisticsDocument10 pagesMRCOG Part 2 - March 2015 Recalls.: StatisticsAmanda RahmawatiNo ratings yet
- Postpartum HemorrhageDocument20 pagesPostpartum Hemorrhagem_amroellahNo ratings yet
- Endometrial Cancer: Manuela RussuDocument38 pagesEndometrial Cancer: Manuela RussuAnonymous 0XqZUl06PmNo ratings yet
- Readings 9th NovemberDocument5 pagesReadings 9th NovemberPedroNo ratings yet
- Laser in DentistryDocument94 pagesLaser in DentistryGirirajan Arumugam100% (1)
- Guideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of AnaesthetistsDocument12 pagesGuideline On Anaesthesia and Sedation in Breastfeeding Women 2020 Guideline From The Association of Anaesthetistsantonio123valenciaNo ratings yet
- Aviation History: Lecture 7: Why Aircraft Needs To Be PressurizedDocument18 pagesAviation History: Lecture 7: Why Aircraft Needs To Be PressurizedPrem KNo ratings yet
- M.Pharm/B.Pharm Final Year Projects (Final Projects 2030)Document7 pagesM.Pharm/B.Pharm Final Year Projects (Final Projects 2030)Subhram Kumar PandaNo ratings yet
- List of Premature Ejaculation BooksDocument4 pagesList of Premature Ejaculation BooksFrank DeLucaNo ratings yet
- Module 5 Biochemistry of Tissues and PhysiologicalDocument214 pagesModule 5 Biochemistry of Tissues and PhysiologicalIna Guinar50% (2)
- Hormones and Metabolic RegulationDocument40 pagesHormones and Metabolic RegulationEka HabinaNo ratings yet
- ASSAM Total: Zone State / City City TotalDocument50 pagesASSAM Total: Zone State / City City TotalShipra BansalNo ratings yet
- Laporan Kirim DinasDocument44 pagesLaporan Kirim DinasDewi PrabawatiNo ratings yet
- Three Dimensional Evaluation On The Effect Of.7Document6 pagesThree Dimensional Evaluation On The Effect Of.7MariyamNo ratings yet
- Conduction of HeartDocument21 pagesConduction of Heartangelsundar22100% (1)
- Case TakingDocument45 pagesCase TakingHomoeopath Aamir SaleemNo ratings yet
- CeftriaxoneDocument1 pageCeftriaxonecen janber cabrillosNo ratings yet
- Extremitas Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Document2 pagesExtremitas Radiography Interpretation: Faculty of Veterinary Medicine, IPB University Telp: +62 8111191333 (Abby Pratama)Intan PradikaNo ratings yet
- Beta Reset - EEG Biofeedback Training For Pain and MoreDocument1 pageBeta Reset - EEG Biofeedback Training For Pain and MoreSadar Psychological and Sports CenterNo ratings yet
- Blunt Abdominal TraumaDocument24 pagesBlunt Abdominal TraumaDen SinyoNo ratings yet
- Crisis InterventionDocument17 pagesCrisis InterventionRaveesh KaimalNo ratings yet
- Soal Ujian Bedah Digestif Dr. Errawan RDocument4 pagesSoal Ujian Bedah Digestif Dr. Errawan RZulfikar ChaeruddinNo ratings yet
- Psychological Management of Cystic FibrosisDocument10 pagesPsychological Management of Cystic FibrosisjuniorebindaNo ratings yet
- MannitolDocument2 pagesMannitolRyan OnellNo ratings yet
- New 2008Document33 pagesNew 2008Kathryn MitchellNo ratings yet
- Jurnal Pharmaceutical CareDocument10 pagesJurnal Pharmaceutical CareSindi CarenaNo ratings yet
- Dams Lastlook Microbiology PDFDocument27 pagesDams Lastlook Microbiology PDFChauhan Monika100% (1)
- Udzbenik NeurologijazastudentestomatologijeDocument1 pageUdzbenik NeurologijazastudentestomatologijeBelmin SalihovicNo ratings yet
- What Is A Clinical TrialDocument12 pagesWhat Is A Clinical TrialkurutalaNo ratings yet
- Ophthal MnemonicsDocument22 pagesOphthal Mnemonicsjunkemail860% (1)
- Tranexamic Acid Drug StudyDocument1 pageTranexamic Acid Drug StudyEsmareldah Henry Sirue100% (1)
- Pharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, NifedipineDocument7 pagesPharm Calcium Channel Blockers (Bahar&Amy) "Vera Dialed The Calcium Channel To Buy A Knife" Verapramil, Diltizaem, Nifedipinecherrybombaz100% (4)