Download as pptx, pdf, or txt
You might also like
- Internal Medicine 1 Conrad FischerDocument35 pagesInternal Medicine 1 Conrad Fischerjaber fathiNo ratings yet
- ECG InterpretationDocument40 pagesECG InterpretationMuhammad BadrushshalihNo ratings yet
- Dysrhythmia Instructor 2018 2 PDFDocument105 pagesDysrhythmia Instructor 2018 2 PDFtvrossyNo ratings yet
- Tutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains MalaysiaDocument56 pagesTutorial in ECG: Dr. Chew Keng Sheng Emergency Medicine Universiti Sains Malaysiafeby_valNo ratings yet
- 22 Disritmia 2018Document60 pages22 Disritmia 2018Nur akilaNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Emergency Medicine كتاب ايمرجنسي مفيد للروتيترز الجدد وملخص مفيدDocument46 pagesEmergency Medicine كتاب ايمرجنسي مفيد للروتيترز الجدد وملخص مفيدSri PoopaseNo ratings yet
- TelemetryDocument3 pagesTelemetryKelly PrattNo ratings yet
- Ecg Essentials 2 PDFDocument45 pagesEcg Essentials 2 PDFjaikishan marathe 69No ratings yet
- ECG Interpretations GoodDocument104 pagesECG Interpretations GoodaymenNo ratings yet
- Ecg Reading NotesDocument17 pagesEcg Reading NotesMarian FloresNo ratings yet
- EKG InterpretationDocument63 pagesEKG InterpretationMiriam Cindy MathullaNo ratings yet
- Cardiovascular NotesDocument23 pagesCardiovascular NotesEmily DongNo ratings yet
- Advanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineDocument88 pagesAdvanced Ekg Interpretation: Micelle J. Haydel, M.D. LSU New Orleans Emergency MedicineRoroNo ratings yet
- Cardiac Stress TestingDocument24 pagesCardiac Stress TestingRhoda Dela Torre ContrerasNo ratings yet
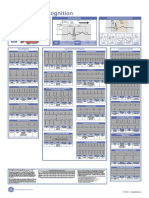
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- ACLS Class Packet PDFDocument9 pagesACLS Class Packet PDFImam GultomNo ratings yet
- The ElectrocardiogramDocument2 pagesThe ElectrocardiogramOh DehNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG GuidekaelenNo ratings yet
- ECG Dysrhthmias IIIDocument31 pagesECG Dysrhthmias IIIAmani Kayed100% (1)
- Joseph Brian L. Costiniano, MD, DPCPDocument70 pagesJoseph Brian L. Costiniano, MD, DPCPcarmsNo ratings yet
- Medicine - EKG - Lab Coat PocketsDocument1 pageMedicine - EKG - Lab Coat Pocketsskeebs23No ratings yet
- ECG ReviewDocument146 pagesECG ReviewThea DinoNo ratings yet
- Basic Ecg Reading - McuDocument63 pagesBasic Ecg Reading - McuJofandAndrea MendozaNo ratings yet
- Abnomalites of ECGDocument81 pagesAbnomalites of ECGgrreddy8364320No ratings yet
- Heart Sounds: Mitral Regurgitation Congestive Heart FailureDocument6 pagesHeart Sounds: Mitral Regurgitation Congestive Heart FailurecindyNo ratings yet
- Arrhythmia Diagnosis and ManagementDocument44 pagesArrhythmia Diagnosis and ManagementanwarNo ratings yet
- Ecg CookbookDocument2 pagesEcg CookbookCalin Popa100% (1)
- Rhythm Interpretation and Its ManagementDocument6 pagesRhythm Interpretation and Its Managementjh_ajjNo ratings yet
- ECG InterpretationDocument52 pagesECG InterpretationFranspol50% (2)
- Cardiovascular ExaminationDocument2 pagesCardiovascular ExaminationasimNo ratings yet
- Abnormal EcgDocument8 pagesAbnormal EcgM.DalaniNo ratings yet
- EkgDocument67 pagesEkgFendi Rafif Dad'sNo ratings yet
- ECG TutorialDocument40 pagesECG TutorialAnonymous HAbhRTs2TfNo ratings yet
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaNo ratings yet
- STEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3Document39 pagesSTEMI Equivalents: DR Elesia Powell-Williams Emergency Medicine Resident PGY3elesia powell100% (1)
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- Electrocardiogram (E.C.G)Document51 pagesElectrocardiogram (E.C.G)Jamuna PatelNo ratings yet
- Cranial Nerves: General CharacteristicsDocument17 pagesCranial Nerves: General CharacteristicsRiki AntoNo ratings yet
- CardiologyDocument1 pageCardiologyapi-3853472100% (2)
- Notes For Clincal CasesDocument12 pagesNotes For Clincal CasesMandeepNo ratings yet
- How To: Read ECG?Document63 pagesHow To: Read ECG?Let BNo ratings yet
- 11 Steps of ECG - Ali Alnahari PDFDocument16 pages11 Steps of ECG - Ali Alnahari PDFBìnhNo ratings yet
- Chapter - 036 Arrhythmias ClassDocument129 pagesChapter - 036 Arrhythmias ClassWisdomIsMiseryNo ratings yet
- ELECTROCARDIOGRAM by Aldrin Jayson AlmadenDocument23 pagesELECTROCARDIOGRAM by Aldrin Jayson AlmadenItsMe AJNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
- Megacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...Document1 pageMegacode Testing Checklist Scenarios 4-7-10 Tachycardia, VF, PEA, PC...krgduraiNo ratings yet
- CVS Examination 3rd MBDocument30 pagesCVS Examination 3rd MBsnowlover boyNo ratings yet
- Basic Ecg 2016Document75 pagesBasic Ecg 2016api-284503860No ratings yet
- Classification of MurmursDocument2 pagesClassification of MurmursNazneen SiddiquiNo ratings yet
- Survival GuideDocument54 pagesSurvival Guidejoeyblowey88No ratings yet
- ST Segment DepressiDocument16 pagesST Segment Depressiaya405No ratings yet
- Neurology Cram NotesDocument19 pagesNeurology Cram Notesrjh1895No ratings yet
- ECGDocument6 pagesECGMatthew MackeyNo ratings yet
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Sampling and Transport of Test MaterialDocument5 pagesSampling and Transport of Test MaterialMustafa A. DawoodNo ratings yet
- Lab 8Document28 pagesLab 8Mustafa A. DawoodNo ratings yet
- Lab - 9-Antimicrobial Agent: Assist. Lec. Wasan HatemDocument14 pagesLab - 9-Antimicrobial Agent: Assist. Lec. Wasan HatemMustafa A. DawoodNo ratings yet
- Lab 10Document14 pagesLab 10Mustafa A. DawoodNo ratings yet
- MarketingDocument110 pagesMarketingriddhi0% (1)
- Drama 30 Year Plan RittingerDocument2 pagesDrama 30 Year Plan Rittingerapi-490177257No ratings yet
- Devoir de Synthèse N°1 - Anglais - 2ème Lettres (2019-2020) Mme Rahmeni JamilaDocument5 pagesDevoir de Synthèse N°1 - Anglais - 2ème Lettres (2019-2020) Mme Rahmeni JamilaSassi LassaadNo ratings yet
- ValeoDocument4 pagesValeographmashNo ratings yet
- Measurement of Steam ConsumptionDocument5 pagesMeasurement of Steam ConsumptionkingkakingNo ratings yet
- Catalog MotoreductoareDocument20 pagesCatalog MotoreductoareNitzu Holhorea CornelNo ratings yet
- Africa Business Map 2022Document80 pagesAfrica Business Map 2022SaktiMukherjeeNo ratings yet
- Fire Awareness PresentationDocument37 pagesFire Awareness Presentationshailu178No ratings yet
- Statement of Consent: Ex: 11-Mar-1980Document2 pagesStatement of Consent: Ex: 11-Mar-1980Analyn Tagara100% (1)
- Power Calculation Drum MotorsDocument2 pagesPower Calculation Drum MotorsFitra VertikalNo ratings yet
- Date - 1 - 9 - 2024 Time - 8 - 42 - 56 - 850Document1 pageDate - 1 - 9 - 2024 Time - 8 - 42 - 56 - 850ANKUSH 87205312No ratings yet
- Black White Sampling in Quantitative Research PresentationDocument12 pagesBlack White Sampling in Quantitative Research PresentationAnna Marie Estrella PonesNo ratings yet
- Hostel RulesDocument15 pagesHostel RulesalogpgNo ratings yet
- Market Development ReportDocument121 pagesMarket Development ReportSrivinayaga XNo ratings yet
- Electromagnetic Shielding Salvatore Celozzi Full ChapterDocument56 pagesElectromagnetic Shielding Salvatore Celozzi Full Chapternorma.catron566100% (10)
- More Details About My Computer: Processor Memory (RAM) Graphics Gaming Graphics Primary Hard DiskDocument2 pagesMore Details About My Computer: Processor Memory (RAM) Graphics Gaming Graphics Primary Hard Diskapi-731169100% (1)
- Wired Dynamic Vocal Mic With CableDocument2 pagesWired Dynamic Vocal Mic With CableMarius DanielNo ratings yet
- Experimental Method of ResearchDocument21 pagesExperimental Method of ResearchCiashell LayeseNo ratings yet
- 03 350-401 - DragDrop - v3Document22 pages03 350-401 - DragDrop - v3Tak Man PONo ratings yet
- TW Supplement WSA 02-2002 V2 3 MRWA - DRAFT 05 Sewerage CodeDocument35 pagesTW Supplement WSA 02-2002 V2 3 MRWA - DRAFT 05 Sewerage CodeDivesh rahulNo ratings yet
- UnivibeDocument1 pageUnivibePablo EspinosaNo ratings yet
- Cs302-Finalterm Solved Mcqs With Refrences by DR Abdul SaboorDocument51 pagesCs302-Finalterm Solved Mcqs With Refrences by DR Abdul SaboorPervez Shaikh100% (1)
- Effective Learning StrategiesDocument5 pagesEffective Learning StrategiesRossy Milena JarabaNo ratings yet
- Article Reveiw FormatDocument18 pagesArticle Reveiw FormatSolomon FarisNo ratings yet
- How To Install Openshift On A Laptop or DesktopDocument7 pagesHow To Install Openshift On A Laptop or DesktopAymenNo ratings yet
- As 1767.2.3-1999 Insulating Liquids Test Methods - Method of Sampling Liquid DielectricsDocument8 pagesAs 1767.2.3-1999 Insulating Liquids Test Methods - Method of Sampling Liquid DielectricsSAI Global - APACNo ratings yet
- Mohit Bansal2 MRF Project ReportDocument87 pagesMohit Bansal2 MRF Project ReportMohit BansalNo ratings yet
- Bien Prononcer L'anglais: Corrigés Et ScriptsDocument43 pagesBien Prononcer L'anglais: Corrigés Et ScriptsThierry HarmannNo ratings yet
- Seiko SLH-2B Instructions ManualDocument4 pagesSeiko SLH-2B Instructions Manualsimpen84No ratings yet
- Deluxe Programmable Thermostat: Climate PerfectDocument12 pagesDeluxe Programmable Thermostat: Climate PerfectBrian TseNo ratings yet