Download as pptx, pdf, or txt
You might also like
- FGI-Guidelines 2014 HOPnew PDFDocument466 pagesFGI-Guidelines 2014 HOPnew PDFahmed67% (3)
- 3.studi Kasus AsmaDocument2 pages3.studi Kasus AsmadelfiNo ratings yet
- NURSING CARE PLAN - Breast CancerDocument2 pagesNURSING CARE PLAN - Breast Cancerderic100% (3)
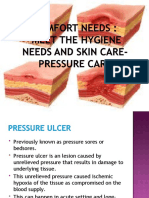
- Pressure SoreDocument3 pagesPressure SoreGhadaNo ratings yet
- 11 Chapter 2Document8 pages11 Chapter 2Muhammad Tariq RazaNo ratings yet
- Cranial Osteopathy For Babies and ChildrenDocument2 pagesCranial Osteopathy For Babies and Childrenomddoc0% (1)
- Pressure Ulcer CareDocument26 pagesPressure Ulcer CarekurapotaNo ratings yet
- Case Study Wound HealingDocument5 pagesCase Study Wound HealingINSANE LEO GAMINGNo ratings yet
- Leg UlcersDocument22 pagesLeg UlcersMarera DomnicNo ratings yet
- Case Presentation Laryngitis TB 70 TahunDocument21 pagesCase Presentation Laryngitis TB 70 TahunMegan Shanzu100% (1)
- 22 Manuscript Intestinal ObstructionDocument8 pages22 Manuscript Intestinal Obstructionkint manlangitNo ratings yet
- Enterocutaneous FistulaDocument1 pageEnterocutaneous FistulaNur FarhanaNo ratings yet
- Intussusception: Prepared By: Aisha H. AlaghaDocument20 pagesIntussusception: Prepared By: Aisha H. AlaghaaiooshaNo ratings yet
- Betty Neuman Health Care System ModelDocument13 pagesBetty Neuman Health Care System ModelJoshua BalladNo ratings yet
- Riaz Gul AHN Unit 1Document106 pagesRiaz Gul AHN Unit 1Riaz Gul RindNo ratings yet
- Final PPT SiDocument38 pagesFinal PPT SiSaad IqbalNo ratings yet
- Futuristic NursingDocument6 pagesFuturistic NursingAnusha Verghese100% (1)
- Penetrating Abdominal Trauma Emergency ManagementDocument29 pagesPenetrating Abdominal Trauma Emergency Managementanjali singhNo ratings yet
- Triage and Disaster: Nur Masyeerah Abdul JalilDocument22 pagesTriage and Disaster: Nur Masyeerah Abdul JalilnavenNo ratings yet
- Burns Assessment - TeachMeSurgeryDocument5 pagesBurns Assessment - TeachMeSurgeryLaroui HoNo ratings yet
- Amputation BedDocument15 pagesAmputation Bedshrijitkalepatil45No ratings yet
- Obstetric Operations and Procedures - CompleteDocument46 pagesObstetric Operations and Procedures - CompleteMax ZealNo ratings yet
- Unit 3 Dev Psy-InfancyDocument31 pagesUnit 3 Dev Psy-InfancySikander MalikNo ratings yet
- Skin Integrity and Wound CareDocument47 pagesSkin Integrity and Wound CareCHALIE MEQUNo ratings yet
- Colostomy CareDocument2 pagesColostomy CareMel RodolfoNo ratings yet
- 2 Assisting Clients To Use Incentive Spirometer DosdosDocument3 pages2 Assisting Clients To Use Incentive Spirometer DosdosBianca Mikaela DosdosNo ratings yet
- MastitisDocument35 pagesMastitisRestu AWNo ratings yet
- Fetal Head MalpositionDocument31 pagesFetal Head Malpositionzamurd76100% (1)
- Wound Healing and Wound CareDocument15 pagesWound Healing and Wound CareNinaNo ratings yet
- Bone Tumor: A. Nithya 1 Year M.SC (Nursing)Document46 pagesBone Tumor: A. Nithya 1 Year M.SC (Nursing)nithya nithyaNo ratings yet
- Central Venous PressureDocument10 pagesCentral Venous PressureAngelo ArquizaNo ratings yet
- Colostomy CareDocument4 pagesColostomy CareRhenzes HaraNo ratings yet
- Female Reproductive System Assessment22Document12 pagesFemale Reproductive System Assessment22pravina praviNo ratings yet
- Hiatal Hernia: BY MR, Vinay KumarDocument27 pagesHiatal Hernia: BY MR, Vinay KumarVinay KumarNo ratings yet
- A Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiDocument4 pagesA Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Penetrating Abdominal TraumaDocument67 pagesPenetrating Abdominal TraumarizkaNo ratings yet
- Esophageal VaricesDocument4 pagesEsophageal VaricesSnapeSnapeNo ratings yet
- Presentation1 Cervical BiopsyDocument14 pagesPresentation1 Cervical BiopsyChanta MaharjanNo ratings yet
- Cholecystitis IntroductionDocument4 pagesCholecystitis IntroductionJechelle Ann Pabustan Martin-BoniquitNo ratings yet
- Notes HemorrhoidsDocument4 pagesNotes HemorrhoidsSanthu Su100% (1)
- Unit IV Power & Politics in NursingDocument18 pagesUnit IV Power & Politics in NursingSHAFIQNo ratings yet
- Position of PatientDocument47 pagesPosition of PatientMuhammad Al-azzizNo ratings yet
- Procedure For DefibrillationDocument6 pagesProcedure For DefibrillationTri RatnawatiNo ratings yet
- Thromboltic TherapyDocument19 pagesThromboltic Therapyhanimozaghi100% (1)
- CVPDocument23 pagesCVPShalini KaluraNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- Pressure Ulcers: by Mr. M. Shivanandha ReddyDocument35 pagesPressure Ulcers: by Mr. M. Shivanandha ReddyDr Ali100% (2)
- Assessing AbdomenDocument115 pagesAssessing AbdomenKris TinaNo ratings yet
- Futuristic NursingDocument14 pagesFuturistic NursingPooja JanghelNo ratings yet
- Futuristic NursingpptDocument98 pagesFuturistic NursingpptmariaNo ratings yet
- Seizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HDocument70 pagesSeizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HRohini RaiNo ratings yet
- Types of Skin Traction PresentationDocument16 pagesTypes of Skin Traction PresentationZerjohn Seniorom100% (1)
- Assignment ON MyelographyDocument12 pagesAssignment ON MyelographyDiana CharaNo ratings yet
- SarcomaDocument2 pagesSarcomaedrichaNo ratings yet
- Nursing Care Plans For Diabetes MellitusDocument12 pagesNursing Care Plans For Diabetes MellitusPuteri AzmanNo ratings yet
- Muscle Strength TestingDocument3 pagesMuscle Strength TestingGiselle Chloe Baluya ico100% (1)
- Colostomy IrrigationDocument2 pagesColostomy IrrigationAudreySalvadorNo ratings yet
- PeritonitisDocument21 pagesPeritonitisVaibhav Karoliya100% (1)
- Care of Bedridden PatientDocument2 pagesCare of Bedridden PatientBrendaJooYeeNo ratings yet
- Core Competencies in Nursing-1Document11 pagesCore Competencies in Nursing-1yakapmNo ratings yet
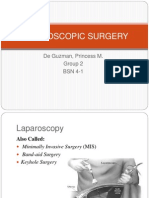
- Laparoscopic SurgeryDocument16 pagesLaparoscopic Surgeryprincess-mendoza-de-guzman-808No ratings yet
- Physiological Changes During PregnancyDocument24 pagesPhysiological Changes During PregnancyerlinNo ratings yet
- Gynecological Operation and Nursing ManagementDocument29 pagesGynecological Operation and Nursing Managementhawra alsaadNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- A Simple Guide to Cholecystitis, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Cholecystitis, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Clinical ReasoningDocument18 pagesClinical ReasoningAna IlmanianNo ratings yet
- IntussusceptionDocument10 pagesIntussusceptionhya2284No ratings yet
- Humms 11 Pasay Diass s2 q1 w4Document20 pagesHumms 11 Pasay Diass s2 q1 w4Victoria De Los SantosNo ratings yet
- Self Assessment ToolDocument25 pagesSelf Assessment ToolReinald Raven Guerrero100% (3)
- Cracked Tooth SyndromeDocument4 pagesCracked Tooth SyndromeANUBHANo ratings yet
- Color TherapyDocument2 pagesColor TherapyMasoom FarishtahNo ratings yet
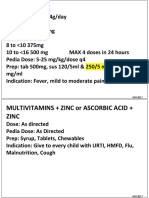
- Common RHU DrugsDocument56 pagesCommon RHU DrugsAlna Shelah IbañezNo ratings yet
- Mini Research Hosp Selayang FuDocument38 pagesMini Research Hosp Selayang FuahmadafifuddinNo ratings yet
- An Overview of Management of Dehydration in Paediatric Age GroupDocument3 pagesAn Overview of Management of Dehydration in Paediatric Age Grouppriyanka2No ratings yet
- Cognitive-Behavioral Treatment of Panic Disorder With AgoraphobiaDocument12 pagesCognitive-Behavioral Treatment of Panic Disorder With Agoraphobiawan nazrolNo ratings yet
- Vagina: 12.1 AnatomyDocument17 pagesVagina: 12.1 AnatomyMarathondy Al FahmiNo ratings yet
- Rehabilitasi AGA AGBDocument40 pagesRehabilitasi AGA AGBalwy sugiartoNo ratings yet
- Marriage Guidance Practice: CounsellingDocument3 pagesMarriage Guidance Practice: CounsellingNata AjahhNo ratings yet
- Spa TreatmentsDocument2 pagesSpa TreatmentsJanhavi SoniNo ratings yet
- Generic Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Document4 pagesGeneric Name: Quinupristin/Dalfopristin - Injection (Kwin-ue-PRIS-tin/DAL-foe-PRIS-tin)Jrose CuerpoNo ratings yet
- Reading ComprehensionDocument6 pagesReading ComprehensionNurul Akmal LokmanNo ratings yet
- MCQ PneuDocument60 pagesMCQ PneuYanesh Bishundat0% (1)
- Tatalaksana Abses HeparDocument6 pagesTatalaksana Abses HeparAdhi Rizky PutraNo ratings yet
- Daftar Obat1Document176 pagesDaftar Obat1puskesmasbancarNo ratings yet
- NCP For BronchitisDocument4 pagesNCP For BronchitisJessa Borre100% (1)
- Romsons All ProductDocument53 pagesRomsons All ProductBoyke WinterbergNo ratings yet
- QI Clinical GuidelinesDocument1 pageQI Clinical GuidelinesNkugwa Mark WilliamNo ratings yet
- Positive Psychotherapy AssignmentsDocument5 pagesPositive Psychotherapy AssignmentsAyushi GargNo ratings yet
- Goals Editable PDFDocument140 pagesGoals Editable PDFManuel Ascanio67% (3)