
Purine Metabolism
Purine Metabolism
You might also like
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDocument84 pagesDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)
- First Aid Assess-Answer SheetDocument9 pagesFirst Aid Assess-Answer Sheettsrattan8116No ratings yet
- Disorder in Purines MetabolismDocument18 pagesDisorder in Purines MetabolismHikma PrajawatiNo ratings yet
- Degradation of PurineDocument36 pagesDegradation of PurineShrey SundriyalNo ratings yet
- Degradation of Purine PDFDocument36 pagesDegradation of Purine PDFShrey SundriyalNo ratings yet
- Gout and Purine Degradation: Arun.SDocument7 pagesGout and Purine Degradation: Arun.SarunNo ratings yet
- 2021 CHO Metabolism 1Document48 pages2021 CHO Metabolism 1xb2k9gzkc9No ratings yet
- DR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)Document20 pagesDR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)modelprof100% (2)
- (3.19) CarbosMetab (PPP, Other Sugars & GAGs)Document74 pages(3.19) CarbosMetab (PPP, Other Sugars & GAGs)pamelaNo ratings yet
- Biochem QuestionsDocument15 pagesBiochem QuestionsSamantha SerraoNo ratings yet
- Lactate PhysiologyDocument5 pagesLactate PhysiologyLee June LyngNo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine MetabolismUbaid AhmedNo ratings yet
- Uric PDFDocument28 pagesUric PDFNgân TrươngNo ratings yet
- PBL1Document2 pagesPBL1ni'New BaobaoNo ratings yet
- BP U9e Metabolism of Nucleic AcidsDocument49 pagesBP U9e Metabolism of Nucleic AcidsChristian Angelo AgbunagNo ratings yet
- ATP Production AEROBIC Metabolism: ST STDocument11 pagesATP Production AEROBIC Metabolism: ST STSiir Pwnsalot100% (1)
- GlycolysisDocument72 pagesGlycolysisaldrinramirez20No ratings yet
- 2.2 Pentose and Uronic PathwayDocument28 pages2.2 Pentose and Uronic PathwayYared gebremedhinNo ratings yet
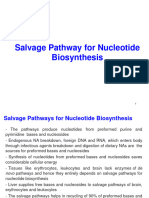
- Salvage Path Nucleotide BiosynthesisDocument20 pagesSalvage Path Nucleotide BiosynthesisBrian Adoka OmdangNo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNo ratings yet
- Disorders of Purine Nucleotide MetabolismDocument3 pagesDisorders of Purine Nucleotide MetabolismPraiseNo ratings yet
- Purine MetabolismDocument30 pagesPurine MetabolismSamarTharwatNo ratings yet
- Week 2Document48 pagesWeek 2beltranayzellheartNo ratings yet
- Lesson 5 Q4Document72 pagesLesson 5 Q4Joshua DurogaNo ratings yet
- Metabolism of Nucleoproteins Part IDocument50 pagesMetabolism of Nucleoproteins Part IAgafioNo ratings yet
- 3-HMP and Glucuronic Acid PathwaysDocument40 pages3-HMP and Glucuronic Acid Pathwayslou765500No ratings yet
- MBS 330-MEDICAL BIOCHEMISTRY II (Term 1 DEFERRED TEST) - CBU-SOM BASIC MEDICAL SCIENCESDocument18 pagesMBS 330-MEDICAL BIOCHEMISTRY II (Term 1 DEFERRED TEST) - CBU-SOM BASIC MEDICAL SCIENCESlucky mbaselaNo ratings yet
- GluconeogenesisDocument12 pagesGluconeogenesisRith Hengmeng (Study Smart)No ratings yet
- BSC Sem VI Nuc Aid MetabDocument24 pagesBSC Sem VI Nuc Aid Metabstarboigaming08No ratings yet
- Carbohydrate Metab 2Document65 pagesCarbohydrate Metab 2Ma-anJaneDiamosNo ratings yet
- Gluco Neo GenesisDocument36 pagesGluco Neo GenesisAmalia DarwisNo ratings yet
- Gluconeogenesis : Molecular Biochemistry IDocument36 pagesGluconeogenesis : Molecular Biochemistry Inazrin_syafiq_3No ratings yet
- Part (II) Nitrogenous Molecules MetabolismDocument10 pagesPart (II) Nitrogenous Molecules MetabolismFlorangNo ratings yet
- Biochemistry FADocument48 pagesBiochemistry FAJaankiNo ratings yet
- Lecture # 7 Pentose Phosphate PathwayDocument44 pagesLecture # 7 Pentose Phosphate PathwayDesy AnggrainiNo ratings yet
- Research Biochem G6PDHDocument5 pagesResearch Biochem G6PDHJohn Whel MararacNo ratings yet
- Nucleotide and CHO Metabolism ActivityDocument3 pagesNucleotide and CHO Metabolism ActivityJanson SarmientoNo ratings yet
- Clinical Microscopy Urine Screening For Metabolic DisordersDocument5 pagesClinical Microscopy Urine Screening For Metabolic DisordersGlazel TulaganNo ratings yet
- Glycolytic Pathways and Red Cell MetabolismDocument6 pagesGlycolytic Pathways and Red Cell Metabolismcaroline vaughanNo ratings yet
- Lecture 7 Pentosephosphate PathwayDocument35 pagesLecture 7 Pentosephosphate PathwayHawaid AhmadNo ratings yet
- Aminoacid MetabolismDocument25 pagesAminoacid MetabolismMischief ManagerNo ratings yet
- MetabolismDocument11 pagesMetabolismMituSamadderNo ratings yet
- Glucose 6 Phosphate Dehydrogenase DeficiencyDocument29 pagesGlucose 6 Phosphate Dehydrogenase Deficiencypurplelavender12No ratings yet
- Glycolysis: Shekhar Chandra Yadav Lecturer Dept. of BiochemistryDocument25 pagesGlycolysis: Shekhar Chandra Yadav Lecturer Dept. of BiochemistryTULSI SHARMANo ratings yet
- Gout and FructoseDocument18 pagesGout and Fructoseabusroor2008No ratings yet
- Neonatal JaundiceDocument7 pagesNeonatal JaundiceGawri AbeyNo ratings yet
- Metabolism of Nucleotides BDSDocument18 pagesMetabolism of Nucleotides BDSzeusmarvolodomNo ratings yet
- Bs VitaminsDocument9 pagesBs Vitaminsrin_ndNo ratings yet
- First Bimonthly OralsDocument21 pagesFirst Bimonthly OralsKimberly Ann LeoragNo ratings yet
- HMP Shuntg6pdDocument6 pagesHMP Shuntg6pdKausik SenNo ratings yet
- Glycolysis Regulation: 1 Dr. Suheir EreqatDocument22 pagesGlycolysis Regulation: 1 Dr. Suheir EreqatIbrahim BarhamNo ratings yet
- Acetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Document17 pagesAcetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Keerthy VenthenNo ratings yet
- PharmacogeneticsDocument36 pagesPharmacogeneticsAmy YuenNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Hexose Monophosphate ShuntDocument38 pagesHexose Monophosphate ShuntJohn Raniel IsidroNo ratings yet
- Pentose Phosphate Pathway: Generation of NADPH and PentosesDocument23 pagesPentose Phosphate Pathway: Generation of NADPH and PentosesV sNo ratings yet
- Calcium & Phosphate MetabolismDocument36 pagesCalcium & Phosphate MetabolismMustafa KhandgawiNo ratings yet
- Vii. Urine Screening For Metabolic DisordersDocument4 pagesVii. Urine Screening For Metabolic DisordersDee GeeNo ratings yet
- Nucleotide Metabolism PPDocument65 pagesNucleotide Metabolism PPCLEMENTNo ratings yet
- Fast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoFrom EverandFast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoNo ratings yet
- TYROXIN HYPERTIROIDISM BaruDocument57 pagesTYROXIN HYPERTIROIDISM BaruHikma PrajawatiNo ratings yet
- Disorder in Purines MetabolismDocument18 pagesDisorder in Purines MetabolismHikma PrajawatiNo ratings yet
- Antropologi Kesehatan IDocument20 pagesAntropologi Kesehatan IHikma PrajawatiNo ratings yet
- 9 Writing Scientific Manuscripts PresentationDocument30 pages9 Writing Scientific Manuscripts PresentationHikma PrajawatiNo ratings yet
- How Do I Study EffectivelyDocument6 pagesHow Do I Study EffectivelyHikma PrajawatiNo ratings yet
- Lta AskebDocument116 pagesLta AskebDiana NoviantiNo ratings yet
- Cancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORDocument7 pagesCancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORvk_204veticoNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- PRESENTASIDocument25 pagesPRESENTASIEko andryNo ratings yet
- Actualizacion Niveles de Autorizacion Pbs Agosto 2020Document27 pagesActualizacion Niveles de Autorizacion Pbs Agosto 2020Alexandra RodríguezNo ratings yet
- Pacemaker SyndromeDocument24 pagesPacemaker SyndromeAbraham PaulNo ratings yet
- Emcrit Airway Checklist 2013 02 05 PDFDocument3 pagesEmcrit Airway Checklist 2013 02 05 PDFspamvarunNo ratings yet
- ARTÍCULO 10 - Application of Nanomedicine and Mesenchymal Stem Cells in Burn InjuriesDocument13 pagesARTÍCULO 10 - Application of Nanomedicine and Mesenchymal Stem Cells in Burn InjuriesPaula RNo ratings yet
- SNAPPE-II Score For Neonatal Acute Physiology WithDocument3 pagesSNAPPE-II Score For Neonatal Acute Physiology WithwennyNo ratings yet
- AHNS Series - Do You Know Your Guidelines? Lip CancerDocument5 pagesAHNS Series - Do You Know Your Guidelines? Lip CancerMdacNo ratings yet
- Chemistry: Critical: (HH) (Ii)Document3 pagesChemistry: Critical: (HH) (Ii)Ahsen NaveedNo ratings yet
- 4B CervixDocument87 pages4B CervixrubenNo ratings yet
- Im Residency FlowchartDocument1 pageIm Residency FlowchartF Badruzzama BegumNo ratings yet
- Mallory Brearey-Resume 2021 1Document2 pagesMallory Brearey-Resume 2021 1api-507675724No ratings yet
- Anatomy of Waldeyer'S Ring (Pharyngeal Lymphatic Tonsillar Ring)Document14 pagesAnatomy of Waldeyer'S Ring (Pharyngeal Lymphatic Tonsillar Ring)Francia ToledanoNo ratings yet
- Coonrad Morrey ElbowDocument2 pagesCoonrad Morrey Elbowgcif88No ratings yet
- Cerebral HemorrhageDocument2 pagesCerebral HemorrhageGian TejadaNo ratings yet
- February 7, 2020 Strathmore TimesDocument16 pagesFebruary 7, 2020 Strathmore TimesStrathmore TimesNo ratings yet
- 6 Minute English The Wonder of BloodDocument4 pages6 Minute English The Wonder of BloodReza ShirmarzNo ratings yet
- DKA ManagementDocument7 pagesDKA ManagementbababrijeshNo ratings yet
- Adverse Reactions To DiureticsDocument8 pagesAdverse Reactions To DiureticsDimas RizkyNo ratings yet
- 01 121 127Document7 pages01 121 12726nazilarenoatNo ratings yet
- Essentials of Nursing Leadership and Management 6th Edition Weiss Test Bank DownloadDocument4 pagesEssentials of Nursing Leadership and Management 6th Edition Weiss Test Bank Downloademmanuelmabelnjt7nn100% (34)
- Journal Pone 0070032 s001 PDFDocument105 pagesJournal Pone 0070032 s001 PDFSuyanto YantoNo ratings yet
- Chapter One Introduction To Pathology Chapter One Introduction To PathologyDocument26 pagesChapter One Introduction To Pathology Chapter One Introduction To PathologySivanarayana JayavaramNo ratings yet
- Mtap-Semr1-Week 2-Diabetes and Glucose MonitoringDocument9 pagesMtap-Semr1-Week 2-Diabetes and Glucose MonitoringJessoliver GalvezNo ratings yet
- Ventilators Zisline - MV200, MV300Document7 pagesVentilators Zisline - MV200, MV300d.kostrov15mtNo ratings yet
- Hall Technique, Stepwise Excavation, Partial Caries Removal TechniqueDocument4 pagesHall Technique, Stepwise Excavation, Partial Caries Removal TechniqueImbador LiesiesNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- Disease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sDocument84 pagesDisease Deficient Enzyme Cardinal Clinical Features Glycogen Structure Von Gierke'sclubstar100% (4)
- First Aid Assess-Answer SheetDocument9 pagesFirst Aid Assess-Answer Sheettsrattan8116No ratings yet
- Disorder in Purines MetabolismDocument18 pagesDisorder in Purines MetabolismHikma PrajawatiNo ratings yet
- Degradation of PurineDocument36 pagesDegradation of PurineShrey SundriyalNo ratings yet
- Degradation of Purine PDFDocument36 pagesDegradation of Purine PDFShrey SundriyalNo ratings yet
- Gout and Purine Degradation: Arun.SDocument7 pagesGout and Purine Degradation: Arun.SarunNo ratings yet
- 2021 CHO Metabolism 1Document48 pages2021 CHO Metabolism 1xb2k9gzkc9No ratings yet
- DR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)Document20 pagesDR Okunowo Wahab Introductory Molecular Biology Lecture Note I (Nucleotides Metabolism)modelprof100% (2)
- (3.19) CarbosMetab (PPP, Other Sugars & GAGs)Document74 pages(3.19) CarbosMetab (PPP, Other Sugars & GAGs)pamelaNo ratings yet
- Biochem QuestionsDocument15 pagesBiochem QuestionsSamantha SerraoNo ratings yet
- Lactate PhysiologyDocument5 pagesLactate PhysiologyLee June LyngNo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine MetabolismUbaid AhmedNo ratings yet
- Uric PDFDocument28 pagesUric PDFNgân TrươngNo ratings yet
- PBL1Document2 pagesPBL1ni'New BaobaoNo ratings yet
- BP U9e Metabolism of Nucleic AcidsDocument49 pagesBP U9e Metabolism of Nucleic AcidsChristian Angelo AgbunagNo ratings yet
- ATP Production AEROBIC Metabolism: ST STDocument11 pagesATP Production AEROBIC Metabolism: ST STSiir Pwnsalot100% (1)
- GlycolysisDocument72 pagesGlycolysisaldrinramirez20No ratings yet
- 2.2 Pentose and Uronic PathwayDocument28 pages2.2 Pentose and Uronic PathwayYared gebremedhinNo ratings yet
- Salvage Path Nucleotide BiosynthesisDocument20 pagesSalvage Path Nucleotide BiosynthesisBrian Adoka OmdangNo ratings yet
- Disorders of Purine and Pyrimidine MetabolismDocument17 pagesDisorders of Purine and Pyrimidine Metabolismtanmay mehtaNo ratings yet
- Disorders of Purine Nucleotide MetabolismDocument3 pagesDisorders of Purine Nucleotide MetabolismPraiseNo ratings yet
- Purine MetabolismDocument30 pagesPurine MetabolismSamarTharwatNo ratings yet
- Week 2Document48 pagesWeek 2beltranayzellheartNo ratings yet
- Lesson 5 Q4Document72 pagesLesson 5 Q4Joshua DurogaNo ratings yet
- Metabolism of Nucleoproteins Part IDocument50 pagesMetabolism of Nucleoproteins Part IAgafioNo ratings yet
- 3-HMP and Glucuronic Acid PathwaysDocument40 pages3-HMP and Glucuronic Acid Pathwayslou765500No ratings yet
- MBS 330-MEDICAL BIOCHEMISTRY II (Term 1 DEFERRED TEST) - CBU-SOM BASIC MEDICAL SCIENCESDocument18 pagesMBS 330-MEDICAL BIOCHEMISTRY II (Term 1 DEFERRED TEST) - CBU-SOM BASIC MEDICAL SCIENCESlucky mbaselaNo ratings yet
- GluconeogenesisDocument12 pagesGluconeogenesisRith Hengmeng (Study Smart)No ratings yet
- BSC Sem VI Nuc Aid MetabDocument24 pagesBSC Sem VI Nuc Aid Metabstarboigaming08No ratings yet
- Carbohydrate Metab 2Document65 pagesCarbohydrate Metab 2Ma-anJaneDiamosNo ratings yet
- Gluco Neo GenesisDocument36 pagesGluco Neo GenesisAmalia DarwisNo ratings yet
- Gluconeogenesis : Molecular Biochemistry IDocument36 pagesGluconeogenesis : Molecular Biochemistry Inazrin_syafiq_3No ratings yet
- Part (II) Nitrogenous Molecules MetabolismDocument10 pagesPart (II) Nitrogenous Molecules MetabolismFlorangNo ratings yet
- Biochemistry FADocument48 pagesBiochemistry FAJaankiNo ratings yet
- Lecture # 7 Pentose Phosphate PathwayDocument44 pagesLecture # 7 Pentose Phosphate PathwayDesy AnggrainiNo ratings yet
- Research Biochem G6PDHDocument5 pagesResearch Biochem G6PDHJohn Whel MararacNo ratings yet
- Nucleotide and CHO Metabolism ActivityDocument3 pagesNucleotide and CHO Metabolism ActivityJanson SarmientoNo ratings yet
- Clinical Microscopy Urine Screening For Metabolic DisordersDocument5 pagesClinical Microscopy Urine Screening For Metabolic DisordersGlazel TulaganNo ratings yet
- Glycolytic Pathways and Red Cell MetabolismDocument6 pagesGlycolytic Pathways and Red Cell Metabolismcaroline vaughanNo ratings yet
- Lecture 7 Pentosephosphate PathwayDocument35 pagesLecture 7 Pentosephosphate PathwayHawaid AhmadNo ratings yet
- Aminoacid MetabolismDocument25 pagesAminoacid MetabolismMischief ManagerNo ratings yet
- MetabolismDocument11 pagesMetabolismMituSamadderNo ratings yet
- Glucose 6 Phosphate Dehydrogenase DeficiencyDocument29 pagesGlucose 6 Phosphate Dehydrogenase Deficiencypurplelavender12No ratings yet
- Glycolysis: Shekhar Chandra Yadav Lecturer Dept. of BiochemistryDocument25 pagesGlycolysis: Shekhar Chandra Yadav Lecturer Dept. of BiochemistryTULSI SHARMANo ratings yet
- Gout and FructoseDocument18 pagesGout and Fructoseabusroor2008No ratings yet
- Neonatal JaundiceDocument7 pagesNeonatal JaundiceGawri AbeyNo ratings yet
- Metabolism of Nucleotides BDSDocument18 pagesMetabolism of Nucleotides BDSzeusmarvolodomNo ratings yet
- Bs VitaminsDocument9 pagesBs Vitaminsrin_ndNo ratings yet
- First Bimonthly OralsDocument21 pagesFirst Bimonthly OralsKimberly Ann LeoragNo ratings yet
- HMP Shuntg6pdDocument6 pagesHMP Shuntg6pdKausik SenNo ratings yet
- Glycolysis Regulation: 1 Dr. Suheir EreqatDocument22 pagesGlycolysis Regulation: 1 Dr. Suheir EreqatIbrahim BarhamNo ratings yet
- Acetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Document17 pagesAcetaminophen Overview: Acetyl-Para-Aminophenol (APAP)Keerthy VenthenNo ratings yet
- PharmacogeneticsDocument36 pagesPharmacogeneticsAmy YuenNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Hexose Monophosphate ShuntDocument38 pagesHexose Monophosphate ShuntJohn Raniel IsidroNo ratings yet
- Pentose Phosphate Pathway: Generation of NADPH and PentosesDocument23 pagesPentose Phosphate Pathway: Generation of NADPH and PentosesV sNo ratings yet
- Calcium & Phosphate MetabolismDocument36 pagesCalcium & Phosphate MetabolismMustafa KhandgawiNo ratings yet
- Vii. Urine Screening For Metabolic DisordersDocument4 pagesVii. Urine Screening For Metabolic DisordersDee GeeNo ratings yet
- Nucleotide Metabolism PPDocument65 pagesNucleotide Metabolism PPCLEMENTNo ratings yet
- Fast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoFrom EverandFast Facts: Deficit di piruvato chinasi per pazienti e sostenitori: Una rara malattia genetica che colpisce I globuli rossi Informazioni + assunzione del controllo = migliore risultatoNo ratings yet
- TYROXIN HYPERTIROIDISM BaruDocument57 pagesTYROXIN HYPERTIROIDISM BaruHikma PrajawatiNo ratings yet
- Disorder in Purines MetabolismDocument18 pagesDisorder in Purines MetabolismHikma PrajawatiNo ratings yet
- Antropologi Kesehatan IDocument20 pagesAntropologi Kesehatan IHikma PrajawatiNo ratings yet
- 9 Writing Scientific Manuscripts PresentationDocument30 pages9 Writing Scientific Manuscripts PresentationHikma PrajawatiNo ratings yet
- How Do I Study EffectivelyDocument6 pagesHow Do I Study EffectivelyHikma PrajawatiNo ratings yet
- Lta AskebDocument116 pagesLta AskebDiana NoviantiNo ratings yet
- Cancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORDocument7 pagesCancer Stem Cells CD44 CD24 ESA CANINE MAMMARY TUMORvk_204veticoNo ratings yet
- Ekg PJKDocument113 pagesEkg PJKdevipuspaNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- PRESENTASIDocument25 pagesPRESENTASIEko andryNo ratings yet
- Actualizacion Niveles de Autorizacion Pbs Agosto 2020Document27 pagesActualizacion Niveles de Autorizacion Pbs Agosto 2020Alexandra RodríguezNo ratings yet
- Pacemaker SyndromeDocument24 pagesPacemaker SyndromeAbraham PaulNo ratings yet
- Emcrit Airway Checklist 2013 02 05 PDFDocument3 pagesEmcrit Airway Checklist 2013 02 05 PDFspamvarunNo ratings yet
- ARTÍCULO 10 - Application of Nanomedicine and Mesenchymal Stem Cells in Burn InjuriesDocument13 pagesARTÍCULO 10 - Application of Nanomedicine and Mesenchymal Stem Cells in Burn InjuriesPaula RNo ratings yet
- SNAPPE-II Score For Neonatal Acute Physiology WithDocument3 pagesSNAPPE-II Score For Neonatal Acute Physiology WithwennyNo ratings yet
- AHNS Series - Do You Know Your Guidelines? Lip CancerDocument5 pagesAHNS Series - Do You Know Your Guidelines? Lip CancerMdacNo ratings yet
- Chemistry: Critical: (HH) (Ii)Document3 pagesChemistry: Critical: (HH) (Ii)Ahsen NaveedNo ratings yet
- 4B CervixDocument87 pages4B CervixrubenNo ratings yet
- Im Residency FlowchartDocument1 pageIm Residency FlowchartF Badruzzama BegumNo ratings yet
- Mallory Brearey-Resume 2021 1Document2 pagesMallory Brearey-Resume 2021 1api-507675724No ratings yet
- Anatomy of Waldeyer'S Ring (Pharyngeal Lymphatic Tonsillar Ring)Document14 pagesAnatomy of Waldeyer'S Ring (Pharyngeal Lymphatic Tonsillar Ring)Francia ToledanoNo ratings yet
- Coonrad Morrey ElbowDocument2 pagesCoonrad Morrey Elbowgcif88No ratings yet
- Cerebral HemorrhageDocument2 pagesCerebral HemorrhageGian TejadaNo ratings yet
- February 7, 2020 Strathmore TimesDocument16 pagesFebruary 7, 2020 Strathmore TimesStrathmore TimesNo ratings yet
- 6 Minute English The Wonder of BloodDocument4 pages6 Minute English The Wonder of BloodReza ShirmarzNo ratings yet
- DKA ManagementDocument7 pagesDKA ManagementbababrijeshNo ratings yet
- Adverse Reactions To DiureticsDocument8 pagesAdverse Reactions To DiureticsDimas RizkyNo ratings yet
- 01 121 127Document7 pages01 121 12726nazilarenoatNo ratings yet
- Essentials of Nursing Leadership and Management 6th Edition Weiss Test Bank DownloadDocument4 pagesEssentials of Nursing Leadership and Management 6th Edition Weiss Test Bank Downloademmanuelmabelnjt7nn100% (34)
- Journal Pone 0070032 s001 PDFDocument105 pagesJournal Pone 0070032 s001 PDFSuyanto YantoNo ratings yet
- Chapter One Introduction To Pathology Chapter One Introduction To PathologyDocument26 pagesChapter One Introduction To Pathology Chapter One Introduction To PathologySivanarayana JayavaramNo ratings yet
- Mtap-Semr1-Week 2-Diabetes and Glucose MonitoringDocument9 pagesMtap-Semr1-Week 2-Diabetes and Glucose MonitoringJessoliver GalvezNo ratings yet
- Ventilators Zisline - MV200, MV300Document7 pagesVentilators Zisline - MV200, MV300d.kostrov15mtNo ratings yet
- Hall Technique, Stepwise Excavation, Partial Caries Removal TechniqueDocument4 pagesHall Technique, Stepwise Excavation, Partial Caries Removal TechniqueImbador LiesiesNo ratings yet