Download as pptx, pdf, or txt
You might also like
- Syndromic Management of Sexually Transmitted InfectionsDocument76 pagesSyndromic Management of Sexually Transmitted Infectionsnamita100% (2)
- Case Incident OB MBADocument4 pagesCase Incident OB MBASahar Al-Jobury57% (7)
- Michelle Carter Appellant BriefDocument101 pagesMichelle Carter Appellant BriefAllison Manning100% (3)
- Presentation Abnormal PuerperiumDocument52 pagesPresentation Abnormal PuerperiumTesfaye AbebeNo ratings yet
- 2023.07.13 - Obstetrics S2. 02 - Puerperal InfectionDocument52 pages2023.07.13 - Obstetrics S2. 02 - Puerperal InfectionVignesh ThangavelNo ratings yet
- Obstetrics - Puerperal InfectionDocument4 pagesObstetrics - Puerperal InfectionJonathanNo ratings yet
- WNHS - OG.Infection Postnatal Infection Treatment (Diagnosis N Management)Document10 pagesWNHS - OG.Infection Postnatal Infection Treatment (Diagnosis N Management)shania indah chinekoNo ratings yet
- Infections of The Female Pelvis: Intrapartum, Postpartum, and Postabortal InfectionsDocument9 pagesInfections of The Female Pelvis: Intrapartum, Postpartum, and Postabortal Infectionsalepedro1234No ratings yet
- 2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesDocument59 pages2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesSaint Pauls ObgynNo ratings yet
- 2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesDocument59 pages2015 Clinical Practice Guidelines On Obstetric and Gynecologic Infectious DiseasesSaint Pauls ObgynNo ratings yet
- Uterine Infection Word DocumentDocument6 pagesUterine Infection Word Documentafreenbegum-0502No ratings yet
- Puerperium ComplicationsDocument28 pagesPuerperium ComplicationsyayayanizaNo ratings yet
- Postpartum Endometritis: - Infection of The Decidua (Ie, - Endomyometritis - ParametritisDocument18 pagesPostpartum Endometritis: - Infection of The Decidua (Ie, - Endomyometritis - ParametritisDeTe Gun Rap'er ConkK'exsNo ratings yet
- Slide 1 STIDocument50 pagesSlide 1 STIMatth N. ErejerNo ratings yet
- Puerperal InfectionsDocument53 pagesPuerperal InfectionsNeharika KumariNo ratings yet
- PUERPERAL INFECTION Ob 3 LacDocument7 pagesPUERPERAL INFECTION Ob 3 LacAlbert Francis BialaNo ratings yet
- Clinical Teaching 4PEUPERAL SEPSISDocument5 pagesClinical Teaching 4PEUPERAL SEPSISAjit M Prasad Prasad100% (1)
- 5.b.intrauterine InfectionDocument31 pages5.b.intrauterine InfectionPriyanka Dyah SetioriniNo ratings yet
- Puerperal Infections Group Report CMCR LectureDocument44 pagesPuerperal Infections Group Report CMCR LectureFERRER, JENNYFER S.No ratings yet
- Abnormal PuerperiumDocument23 pagesAbnormal Puerperiumseema pundirNo ratings yet
- Puerperal SepsisDocument45 pagesPuerperal SepsisKalo kajiNo ratings yet
- Puerperial PyrexiaDocument4 pagesPuerperial PyrexiaSyaira TanjidNo ratings yet
- Chorioamnionitis: Intra Amniotic Infection (Disease Study)Document7 pagesChorioamnionitis: Intra Amniotic Infection (Disease Study)Aprilyn ay-ayenNo ratings yet
- Puerperal SepsisDocument34 pagesPuerperal SepsisSanthosh.S.UNo ratings yet
- Intrauterine InfectionDocument17 pagesIntrauterine InfectionAndhika Aryandhie DwiputraNo ratings yet
- Definition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheDocument7 pagesDefinition-: Pelvic Inflammatory Disease (PID) Is A Sexually Transmitted Inflammatory Condition of TheanweshaNo ratings yet
- EndometritisDocument3 pagesEndometritisJazmin Venice Lasala0% (1)
- Abdominal Pain in Gynecology Non PregnantDocument34 pagesAbdominal Pain in Gynecology Non PregnantRyantino IrdanNo ratings yet
- Puerperal PyrexiaDocument4 pagesPuerperal PyrexiaLulano MbasuNo ratings yet
- EndometritisDocument6 pagesEndometritisandriansyah2110% (1)
- Jurnal Pubmed EndoDocument6 pagesJurnal Pubmed EndoSofyanNo ratings yet
- Idog 03 210Document7 pagesIdog 03 210jwmeadow2401No ratings yet
- 17 The Puerperium Noted PDFDocument39 pages17 The Puerperium Noted PDFmohammed farajiNo ratings yet
- Nursing Care of Clients With Reproductive Health ProblemsDocument100 pagesNursing Care of Clients With Reproductive Health ProblemsHassen ZabalaNo ratings yet
- PID PresentationDocument23 pagesPID Presentationakankiza.lucky83No ratings yet
- Puerpral SepsisDocument5 pagesPuerpral SepsisPriscilla Sarah PayneNo ratings yet
- Pelvic Inflammatory DiseaseDocument9 pagesPelvic Inflammatory DiseaseanweshaNo ratings yet
- Fever During and After ChildbirthDocument33 pagesFever During and After ChildbirthcafemedNo ratings yet
- Sexually Transmitted InfectionDocument11 pagesSexually Transmitted Infectionmark OrpillaNo ratings yet
- Urinary Tract Infections in Pregnancy: Jeffrey Pradeep RajDocument29 pagesUrinary Tract Infections in Pregnancy: Jeffrey Pradeep RajjeffreyprajNo ratings yet
- Post Partum Infections Obstet MedDocument5 pagesPost Partum Infections Obstet MedMutiaIlyasNo ratings yet
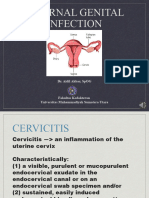
- Daring Aidil Akbar Internal Genital InfectionDocument29 pagesDaring Aidil Akbar Internal Genital InfectionrakaNo ratings yet
- Sumu PDFDocument30 pagesSumu PDFalokpalreshaNo ratings yet
- Puerperal FeverDocument19 pagesPuerperal FeverJosh Matthew RosalesNo ratings yet
- Post DeliveryDocument26 pagesPost DeliverySaid Said (ابو خالد)No ratings yet
- Pregnancy Complication: Department of Gynaecology and ObstetricsDocument40 pagesPregnancy Complication: Department of Gynaecology and ObstetricssanjivdasNo ratings yet
- Abnormal PuerperiumDocument21 pagesAbnormal PuerperiumNatukunda DianahNo ratings yet
- Chapter 44 STIDocument5 pagesChapter 44 STIRebeccaNo ratings yet
- 54.vaginal DischargeDocument40 pages54.vaginal DischargebenNo ratings yet
- Duh Tubuh Wanita, DR SAYU.,SpKK, WMDocument62 pagesDuh Tubuh Wanita, DR SAYU.,SpKK, WMdickypranataNo ratings yet
- OB - Puerperal ComplicationsDocument5 pagesOB - Puerperal ComplicationsDarren Mae MosadaNo ratings yet
- WOMAN WITH SEXUALLY TRANSMITTED INFECTION NewDocument86 pagesWOMAN WITH SEXUALLY TRANSMITTED INFECTION NewRaiden VizcondeNo ratings yet
- BY:-Shalini Joshi M.SC NURSING Ist Year S.C.O.N. DehradunDocument52 pagesBY:-Shalini Joshi M.SC NURSING Ist Year S.C.O.N. DehradunshravaniNo ratings yet
- Abnormalpuerperium 190328060723 1Document126 pagesAbnormalpuerperium 190328060723 1Preeti ChouhanNo ratings yet
- MCN II Puerperal Infection 1Document23 pagesMCN II Puerperal Infection 1Rafik LakhdarNo ratings yet
- Healthcare Associated Infections in The Nicu PowerpointDocument21 pagesHealthcare Associated Infections in The Nicu Powerpointapi-489132887No ratings yet
- Abnormalities of The PuerperiumDocument59 pagesAbnormalities of The PuerperiumVincent Maralit MaterialNo ratings yet
- Handouts of Complications of PostnatalDocument12 pagesHandouts of Complications of PostnatalAshish GuptaNo ratings yet
- Guide To Infection Control in The HospitalDocument9 pagesGuide To Infection Control in The HospitalJoanne Bernadette AguilarNo ratings yet
- Complications of Pelvic InfectionDocument16 pagesComplications of Pelvic InfectionFakhriNo ratings yet
- Report Card CommentsDocument13 pagesReport Card CommentsNatércia OliveiraNo ratings yet
- How To Get System Status, User Status and Long Text For An ObjectDocument13 pagesHow To Get System Status, User Status and Long Text For An ObjectPiedone64No ratings yet
- 2020 CustomerEducationPlaybookDocument16 pages2020 CustomerEducationPlaybookViniloNo ratings yet
- Of Mice and Men Chapter 1 Figurative Language Study GuideDocument4 pagesOf Mice and Men Chapter 1 Figurative Language Study GuideVictoria ScrivenNo ratings yet
- The Power of VisionDocument15 pagesThe Power of VisionJohn MuyimbaNo ratings yet
- Malvern - Aero S Dry DispersionDocument9 pagesMalvern - Aero S Dry Dispersionjashole jashole100% (1)
- Stoichiometric Tables: Batch System Stoichiometric TableDocument4 pagesStoichiometric Tables: Batch System Stoichiometric TableSKRNo ratings yet
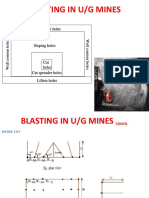
- Blasting in U/G Mines: Roof Contour Holes Roof Contour HolesDocument10 pagesBlasting in U/G Mines: Roof Contour Holes Roof Contour HolesSiddharth MukhillaNo ratings yet
- Neurons and Synapses: Essential Idea: Neurons Transmit The Message, Synapses Modulate The MessageDocument26 pagesNeurons and Synapses: Essential Idea: Neurons Transmit The Message, Synapses Modulate The MessageSeanLaiNo ratings yet
- Self Worth SpeechDocument1 pageSelf Worth SpeechAbigail Fritz GoloNo ratings yet
- Fin546 Article Review ZainoorDocument4 pagesFin546 Article Review ZainoorZAINOOR IKMAL MAISARAH MOHAMAD NOORNo ratings yet
- Semana 2Document1 pageSemana 2johanaNo ratings yet
- The Doctrine of The Hypostatic Union AffDocument28 pagesThe Doctrine of The Hypostatic Union AffMeland NenoNo ratings yet
- Describing Yourself and Others (Wa) : Kore 1. Kore は jitensha desu (This is a bike)Document5 pagesDescribing Yourself and Others (Wa) : Kore 1. Kore は jitensha desu (This is a bike)Peter Sin-KeoNo ratings yet
- Decision-Making in Foreign Policy PDFDocument10 pagesDecision-Making in Foreign Policy PDFvishal rajput100% (1)
- AMS Abstracts 2012Document283 pagesAMS Abstracts 2012kiutungpoonNo ratings yet
- Inspirations Fall 2013-11-04Document40 pagesInspirations Fall 2013-11-04karen_gn78786No ratings yet
- Skin Deep Tattoo Magazine - April 2014 UKDocument100 pagesSkin Deep Tattoo Magazine - April 2014 UKDaniel Ignacio Mena Palma0% (1)
- Distinguish Between Cash Flow and Fund Flow StatementDocument3 pagesDistinguish Between Cash Flow and Fund Flow StatementSachin GodseNo ratings yet
- Livingston County Eclipse GuideDocument4 pagesLivingston County Eclipse GuideThe Livingston County NewsNo ratings yet
- Siren Song Thesis StatementDocument7 pagesSiren Song Thesis StatementSherri Cost100% (2)
- Materi To TOEFL 01 NovemberDocument73 pagesMateri To TOEFL 01 Novembernamira ammarinNo ratings yet
- History: About Kotak Mahindra BankDocument15 pagesHistory: About Kotak Mahindra BankVishal PawarNo ratings yet
- Ind As 115 VS Ind As 18Document7 pagesInd As 115 VS Ind As 18Yogendrasinh RaoNo ratings yet
- Research JysonDocument19 pagesResearch JysonSimon ShikongoNo ratings yet
- Chapter 8 - Financial AnalysisDocument4 pagesChapter 8 - Financial AnalysisLưu Ngọc Tường ViNo ratings yet
- (Maa 3.5) Sin, Cos, Tan On The Unit Circle - Identities - SolutionsDocument6 pages(Maa 3.5) Sin, Cos, Tan On The Unit Circle - Identities - Solutionsrogchen666No ratings yet
- TLM 6006 (Logistics and Transportation Management) Assignment Ma Wah Wah Khaing TLM - 74 (Section B)Document4 pagesTLM 6006 (Logistics and Transportation Management) Assignment Ma Wah Wah Khaing TLM - 74 (Section B)Wah KhaingNo ratings yet