Download as ppt, pdf, or txt
You might also like
- Code Stroke AlgorithmDocument1 pageCode Stroke AlgorithmZharifah Fauziyyah NafisahNo ratings yet
- AclsDocument20 pagesAclsqueennita69100% (4)
- Early Treatment With High-Potency Statins in Patients With Acute Coronary Syndrome-An Example of Personalized MedicineDocument5 pagesEarly Treatment With High-Potency Statins in Patients With Acute Coronary Syndrome-An Example of Personalized MedicineFebrylia Tasya PongsitammuNo ratings yet
- Gibson - Pre Pci Statin Therapy ShortDocument23 pagesGibson - Pre Pci Statin Therapy Shortryma bouldjedjNo ratings yet
- Pharma Mar Smart Fund Short ThesisDocument24 pagesPharma Mar Smart Fund Short Thesisjulia skripka-serry20% (5)
- Rhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Document10 pagesRhythm QRS Duration Atrial Rate QT Interval Ventricular Rate QRS Axis (Compute)Luis PadillaNo ratings yet
- Acs CCS 2021 KLDocument52 pagesAcs CCS 2021 KLPitchya WangmeesriNo ratings yet
- Follow UpDocument3 pagesFollow UpNur AmirahNo ratings yet
- Critical Care Trauma Centre Deep Venous Thrombosis Prophylaxis Preprinted OrdersDocument1 pageCritical Care Trauma Centre Deep Venous Thrombosis Prophylaxis Preprinted OrdersrisnayektiNo ratings yet
- STEMI Thrombolysis Protocol STElevation MIDocument6 pagesSTEMI Thrombolysis Protocol STElevation MISurya AtmajaNo ratings yet
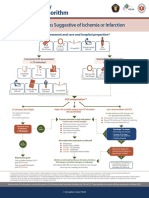
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Randomized Trial of Atorvastatin For Reduction of Myocardial Damage During Coronary InterventionDocument5 pagesRandomized Trial of Atorvastatin For Reduction of Myocardial Damage During Coronary InterventionHarunNo ratings yet
- 08D. Stroke Physician CT Imaging Checklist v12 FinalDocument3 pages08D. Stroke Physician CT Imaging Checklist v12 FinalJuan Carlos Rivera AristizabalNo ratings yet
- Blockade R A SDocument20 pagesBlockade R A SAlaa KhazalehNo ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- Sin Titulo 3Document1 pageSin Titulo 3Sandra Milena Ospina HernandezNo ratings yet
- Perioperative Anticoagulation Bridging Guideline PostedDocument6 pagesPerioperative Anticoagulation Bridging Guideline PostedNuc Alexandru100% (1)
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
- Laboratory Blood Request FormDocument2 pagesLaboratory Blood Request FormIsaac AgbemafleNo ratings yet
- CCU 2017 AntiplateletDocument22 pagesCCU 2017 AntiplateletDhinie NovianiNo ratings yet
- Advances in Acute Stroke Management: Maj Arti Sawhney Moderator: WG CDR Salil GuptaDocument34 pagesAdvances in Acute Stroke Management: Maj Arti Sawhney Moderator: WG CDR Salil Guptagauravbatta99No ratings yet
- 0739 Kapadia Tricuspid RepairDocument48 pages0739 Kapadia Tricuspid Repairhbasrawala110No ratings yet
- TrialsDocument12 pagesTrialsRaaj SharmaNo ratings yet
- High Yield Internal Medicine Shelf Review 2Document25 pagesHigh Yield Internal Medicine Shelf Review 2zoozsuhai2No ratings yet
- Acute Stroke ProtocolDocument3 pagesAcute Stroke ProtocolKarissaNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- Penatalaksanaan Awal Sindrom Koroner Akut: Dr. Arfianamin NST, Mked (Card), SPJP, Aifo-KDocument19 pagesPenatalaksanaan Awal Sindrom Koroner Akut: Dr. Arfianamin NST, Mked (Card), SPJP, Aifo-KDan Gatot OrthopedockNo ratings yet
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
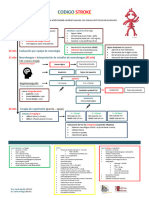
- Codigo Stroke 2Document1 pageCodigo Stroke 2Gabriela RuizNo ratings yet
- Facilitated Pci Vs Rescue Pci - DR Dolly MathewDocument51 pagesFacilitated Pci Vs Rescue Pci - DR Dolly MathewJose JacobNo ratings yet
- 2.3 Cập nhật chẩn đoán và điều trị suy tim-14-11-2021 - .pptx 2Document1 page2.3 Cập nhật chẩn đoán và điều trị suy tim-14-11-2021 - .pptx 2tranlekieutrinh166No ratings yet
- Activase Rt-PA (Acute Ischemic Stroke)Document11 pagesActivase Rt-PA (Acute Ischemic Stroke)bishoy.youssef.cpiNo ratings yet
- 10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHADocument32 pages10.1 New Era in DVT Management Single Drug Approach J Nugroho MD FIHAEmdan SengadjiNo ratings yet
- WECOC - Management of NSTEMI and Invasive StrategyDocument42 pagesWECOC - Management of NSTEMI and Invasive StrategyAdiyanto DidietNo ratings yet
- VTE Prophylaxis GuidelinesDocument1 pageVTE Prophylaxis GuidelinesSylvia Ruth Alisa Nababan100% (1)
- Stroke Hiperakut (Dr. Dedi Sutia, SP.N (K), FINA, MARS)Document35 pagesStroke Hiperakut (Dr. Dedi Sutia, SP.N (K), FINA, MARS)Sitti Fatwan NisakNo ratings yet
- TTTDocument1 pageTTTFatima Zahra ChraaNo ratings yet
- Duty Rabu 13 10 21 Post Pra MRDocument91 pagesDuty Rabu 13 10 21 Post Pra MRAmrina RosyadaNo ratings yet
- Acute Ischemic Stroke: Section Cerebrovascular DiseaseDocument4 pagesAcute Ischemic Stroke: Section Cerebrovascular DiseasenashihunamienNo ratings yet
- Olmos. Secuencia Novartis 2023 H12ODocument36 pagesOlmos. Secuencia Novartis 2023 H12ODavid OlmosNo ratings yet
- Expanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDocument29 pagesExpanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDr. RajibNo ratings yet
- NSTEMIDocument29 pagesNSTEMIGeanina Creanga100% (1)
- Wform.3A Lembar Pengumpul Data PpraDocument4 pagesWform.3A Lembar Pengumpul Data PpraIput SyarhilNo ratings yet
- Phác Đồ 1 Giờ Trong Chẩn Đoán Và Điều Trị Nhồi Máu Cơ Tim CấpDocument14 pagesPhác Đồ 1 Giờ Trong Chẩn Đoán Và Điều Trị Nhồi Máu Cơ Tim CấpTieu Ngoc LyNo ratings yet
- POMR ResponsiDocument7 pagesPOMR ResponsiAcha TuhepalyNo ratings yet
- TWILIGHTDocument24 pagesTWILIGHTRodrigo MartinNo ratings yet
- MR 4 AprilDocument11 pagesMR 4 AprilAriella maydenNo ratings yet
- Erina Nur Mahmudah-Typhoid FeverDocument3 pagesErina Nur Mahmudah-Typhoid FeverSemestaNo ratings yet
- UNC ED Code Stroke Pathway 9 2016 FINALDocument2 pagesUNC ED Code Stroke Pathway 9 2016 FINALJackNo ratings yet
- Chest Pain Notes USMLE Step 3Document3 pagesChest Pain Notes USMLE Step 3kisria100% (1)
- Kegawatdaruratan JantungDocument44 pagesKegawatdaruratan JantungMeiniaNo ratings yet
- Table 1: Intial Evaluation On Arrival To ER For All PatientsDocument1 pageTable 1: Intial Evaluation On Arrival To ER For All PatientsHetoshima KeiNo ratings yet
- IACVC2 MateriDocument28 pagesIACVC2 MaterililiNo ratings yet
- 9002m Krystal Mrtx849 Krasg12c MutationDocument8 pages9002m Krystal Mrtx849 Krasg12c MutationRahulNo ratings yet
- Activase (Alteplase) in Acute Ischemic Stroke: Frequently Asked Questions AboutDocument16 pagesActivase (Alteplase) in Acute Ischemic Stroke: Frequently Asked Questions AboutHappiness ProjectNo ratings yet
- (Contemporary Cardiology) James E. Tcheng - Primary Angioplasty in Acute Myocardial Infarction-Humana Press (2002)Document194 pages(Contemporary Cardiology) James E. Tcheng - Primary Angioplasty in Acute Myocardial Infarction-Humana Press (2002)Michael HartNo ratings yet
- Chest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsDocument16 pagesChest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsJose AnaconaNo ratings yet
- Stable Angina PectorisDocument11 pagesStable Angina Pectorismarco_bawNo ratings yet
- Atrioventricular Septal DefectDocument3 pagesAtrioventricular Septal DefectManishta Menaka DhuromsinghNo ratings yet
- Dengue Associated Acute Kidney Infection...Document9 pagesDengue Associated Acute Kidney Infection...Mono KoromoNo ratings yet
- Coronary AngiographyDocument71 pagesCoronary AngiographyEileen del Rosario100% (2)
- EcgDocument86 pagesEcgHidayatul ゆきNo ratings yet
- Hypertension in Geriatrics 2010Document51 pagesHypertension in Geriatrics 2010Andre HawkNo ratings yet
- Angiography PDFDocument1 pageAngiography PDFanon_720827871No ratings yet
- ECG InterpretationDocument81 pagesECG InterpretationRidyah Ning Tyas100% (2)
- Aortic RegurgitationDocument19 pagesAortic RegurgitationsunilgenextNo ratings yet
- ICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular HypertrophyDocument5 pagesICRJ-Validation of Cornell Product As A Method of Assessing Left Ventricular Hypertrophysamir raflaNo ratings yet
- Huszar's Basic Dysrhythmias and Acute Coronary Syndromes: Interpretation and Management Text & Pocket Guide Package - Ebook Keith WesleyDocument54 pagesHuszar's Basic Dysrhythmias and Acute Coronary Syndromes: Interpretation and Management Text & Pocket Guide Package - Ebook Keith Wesleyrichard.knapp379100% (3)
- Acute Coronary Syndrome: Patsadee Nachom MDDocument58 pagesAcute Coronary Syndrome: Patsadee Nachom MDRachapon OngwibunwongNo ratings yet
- Cathet Cardio Intervent - 2022 - Rempakos - An Algorithmic Approach To Balloon Undilatable Coronary LesionsDocument9 pagesCathet Cardio Intervent - 2022 - Rempakos - An Algorithmic Approach To Balloon Undilatable Coronary LesionsVimal NishadNo ratings yet
- ICM Triple CCTs - Resp Medicine and GIM v1.0Document11 pagesICM Triple CCTs - Resp Medicine and GIM v1.0Achyut KanungoNo ratings yet
- 9 Cardiology Case Scenarios EditedDocument9 pages9 Cardiology Case Scenarios EditedQusai IbraheemNo ratings yet
- Osce PDFDocument51 pagesOsce PDFAlfonso PeñarroyaNo ratings yet
- Unstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowDocument27 pagesUnstable Angina: DR Abdul Mateen Ansari, MD Professor and HOD General Medicine, Cimsh, LucknowCyntia KhairaniNo ratings yet
- Curs 9 Myocarditis CardiomyopathyDocument41 pagesCurs 9 Myocarditis CardiomyopathyIliescu DenisaNo ratings yet
- KDIGO GD Membranous NephropathyDocument1 pageKDIGO GD Membranous NephropathyF AudreyNo ratings yet
- Insuficienta Renala Acuta, Leziunea Acuta RenalaDocument40 pagesInsuficienta Renala Acuta, Leziunea Acuta RenalaLeoveanu MirelNo ratings yet
- Yoga Yuniadi - Wide QRS Complex Tachycardia - BaruDocument59 pagesYoga Yuniadi - Wide QRS Complex Tachycardia - BaruZulhelmiNo ratings yet
- DefibrillatorDocument44 pagesDefibrillatorDipika JangpangiNo ratings yet
- Uptodte TSVDocument215 pagesUptodte TSVcrilala23No ratings yet
- Applying To The AmcDocument101 pagesApplying To The AmcJayagopi KadarasenNo ratings yet
- Congenital Heart DefectsDocument19 pagesCongenital Heart DefectsNader Smadi67% (3)
- 1.1 Scope of ServicesDocument6 pages1.1 Scope of ServicesSwati BajpaiNo ratings yet
- Ventricular Septal Defect VSD FactsheetDocument3 pagesVentricular Septal Defect VSD FactsheetArgolekso RatriNo ratings yet