
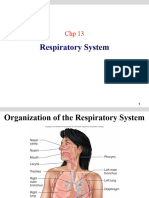
Respiratory System Disorders
Respiratory System Disorders
You might also like
- DDAL04 Expanded Dark Gifts Table OPTIONAL CONTENT PDFDocument3 pagesDDAL04 Expanded Dark Gifts Table OPTIONAL CONTENT PDFDavidHavokNo ratings yet
- Basic Care & Comfort Nclex RN UwDocument10 pagesBasic Care & Comfort Nclex RN Uwgwen scribd100% (1)
- Amboss ECGDocument13 pagesAmboss ECGAllysahNo ratings yet
- General Practitioner - Pulmonology MCQsDocument37 pagesGeneral Practitioner - Pulmonology MCQsAsif Newaz100% (7)
- Ventilatory Assistance - Fall 2021Document36 pagesVentilatory Assistance - Fall 2021j dog100% (1)
- Bio 215 Topic 7 RespiratoryDocument46 pagesBio 215 Topic 7 RespiratoryYara BeainiNo ratings yet
- Respiratory SystemDocument90 pagesRespiratory SystemMaria MargaritaNo ratings yet
- RESPIRATORY-SYSTEM pptx1137Document32 pagesRESPIRATORY-SYSTEM pptx1137Jerick Sevilla SearesNo ratings yet
- Dyspnea in Children - Wahyuni IndawatiDocument20 pagesDyspnea in Children - Wahyuni IndawatiTarmidi MidziNo ratings yet
- Acute Respiratory Fauilr - PDF CVS PART 4Document61 pagesAcute Respiratory Fauilr - PDF CVS PART 4LexNo ratings yet
- Chap07 RespiratoryDocument44 pagesChap07 RespiratoryShere AlmansuoriNo ratings yet
- Chapter 11 - Respiratory SystemsDocument122 pagesChapter 11 - Respiratory Systemsnokate konkoorNo ratings yet
- VENTILATIONDocument27 pagesVENTILATIONezeudunicholas16No ratings yet
- OxygenationDocument50 pagesOxygenationLulu MushiNo ratings yet
- L4 - Common Disorders of Respiratory SystemDocument29 pagesL4 - Common Disorders of Respiratory SystemRand ELABEDNo ratings yet
- NCM 118Responses-to-Altered-Ventilatory-FunctionDocument169 pagesNCM 118Responses-to-Altered-Ventilatory-FunctionAddah, Dhenaraiza H.No ratings yet
- Dr. Sunita Saxena - Breathing and Exchange of GassesDocument48 pagesDr. Sunita Saxena - Breathing and Exchange of GassesDivya AgarawalNo ratings yet
- 8respiratory SystemDocument49 pages8respiratory SystemJack OneNo ratings yet
- HANDOUTS Finals CH 15Document24 pagesHANDOUTS Finals CH 15hii385156No ratings yet
- Lecture 6 Respiratory System 2Document33 pagesLecture 6 Respiratory System 2hafiz patahNo ratings yet
- NCM 112 OXYGENATION - HandoutDocument9 pagesNCM 112 OXYGENATION - Handoutissaiahnicolle100% (1)
- Module 3 PDF 2024Document16 pagesModule 3 PDF 2024gagansshemdiNo ratings yet
- Respiration SystemDocument49 pagesRespiration Systemfebe_aldellaNo ratings yet
- A QuickGuide On COPD 2022 - 0Document6 pagesA QuickGuide On COPD 2022 - 0housesofthelyricNo ratings yet
- M8 - Investigations and Monitoring in The ICUDocument68 pagesM8 - Investigations and Monitoring in The ICUVishal KumarNo ratings yet
- Respiratory SystemDocument192 pagesRespiratory SystemQuolette Constante100% (1)
- NCMB312M1CU3Document16 pagesNCMB312M1CU3Georgia De OcampoNo ratings yet
- NCMB 312 M1 Cu3Document16 pagesNCMB 312 M1 Cu3Georgia De OcampoNo ratings yet
- Gas Exchange and Alveoli 2Document18 pagesGas Exchange and Alveoli 213obasuyioNo ratings yet
- Report Ncm103Document68 pagesReport Ncm103john_mesa_5No ratings yet
- Gaseous Exchange in MammalsDocument35 pagesGaseous Exchange in Mammalsmahanswarnima08No ratings yet
- Respiratory SystemDocument6 pagesRespiratory SystemCraigNo ratings yet
- Hypoxemic Respiratory FailureDocument70 pagesHypoxemic Respiratory FailureMohamed Rikarz Ahamed RikarzNo ratings yet
- Basic Respiratory Mechanics (DR Arif)Document36 pagesBasic Respiratory Mechanics (DR Arif)Rizqi Luqmanul HakimNo ratings yet
- Respiratory SystemDocument24 pagesRespiratory SystemArjunNo ratings yet
- Respiration NotesDocument4 pagesRespiration NotesJana AldourNo ratings yet
- CODPDocument34 pagesCODPNeeraja M SureshNo ratings yet
- A Level Gaseous Exchange Continued - 032759Document13 pagesA Level Gaseous Exchange Continued - 032759onyangaismail12No ratings yet
- Final PhysioDocument1,111 pagesFinal PhysioSana Savana Aman R100% (1)
- Respiratorio-Openstax Biology2e ch39Document43 pagesRespiratorio-Openstax Biology2e ch39ANo ratings yet
- Oxygen Therapy, Trach Care and SuctioningDocument44 pagesOxygen Therapy, Trach Care and SuctioningEmily Boehmer100% (1)
- Respiratory System PhysiologyDocument35 pagesRespiratory System PhysiologySherwan R Shal100% (2)
- Ventilasi PerfusiDocument44 pagesVentilasi PerfusiIdahrachman515100% (1)
- ARDS With PathophysiologyDocument79 pagesARDS With Pathophysiologymabec pagaduan95% (19)
- Ventilasi Pulmonal Dan Diffusi Gas PernafasanDocument18 pagesVentilasi Pulmonal Dan Diffusi Gas PernafasanRaudhah RamadiyantikaNo ratings yet
- Respiratory PhysiologyDocument98 pagesRespiratory PhysiologySurya SuryaNo ratings yet
- Vent TherapyDocument10 pagesVent TherapychuhuaNo ratings yet
- Respiratory System The ElderlyDocument37 pagesRespiratory System The ElderlyDanica FrancoNo ratings yet
- Oxygenation 1 PDFDocument4 pagesOxygenation 1 PDFAbdullah Al NomanNo ratings yet
- 4-1pulmonary DisordersDocument38 pages4-1pulmonary DisordersAbdallah AlasalNo ratings yet
- Chap 12 RespirationDocument48 pagesChap 12 RespirationFungai MuganhuNo ratings yet
- Presentation Topic: Causes of Ventilation PerfusionDocument9 pagesPresentation Topic: Causes of Ventilation PerfusionAbDul RaufNo ratings yet
- Oxygenation Part 1Document86 pagesOxygenation Part 1Shaira Mae Fangon De GuzmanNo ratings yet
- Ventilation Perfusion Ratio & Diffusion of GasesDocument28 pagesVentilation Perfusion Ratio & Diffusion of GasesRiyaNo ratings yet
- Disorder ofDocument207 pagesDisorder ofyewollolijfikreNo ratings yet
- Distress RespiratoriopdfDocument11 pagesDistress RespiratoriopdfDiana CarolinaNo ratings yet
- Notes of Human Physiology Class 11Document9 pagesNotes of Human Physiology Class 11ADWAITH LALU100% (1)
- Pulmonary VentilationDocument12 pagesPulmonary Ventilationtan shin meiNo ratings yet
- Respiratory System: The Second HalfDocument35 pagesRespiratory System: The Second HalfnicopiiNo ratings yet
- B.8 Situation - Care of Client With Problems in OxygenationDocument11 pagesB.8 Situation - Care of Client With Problems in OxygenationSOLEIL LOUISE LACSON MARBASNo ratings yet
- Fundamentals - CH 40: Oxygenation/Gas Exchange: Nloa Sfe B.8 Situation - Care of Client With Problems in OxygenationDocument20 pagesFundamentals - CH 40: Oxygenation/Gas Exchange: Nloa Sfe B.8 Situation - Care of Client With Problems in OxygenationSOLEIL LOUISE LACSON MARBASNo ratings yet
- ImrozDocument57 pagesImrozSyed Imroz KhanNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Internet Addiction: Kimberly S. YoungDocument14 pagesInternet Addiction: Kimberly S. YoungKairat ParpiyevNo ratings yet
- Stop Unsafe Sex: Impact On AIDS and Unwanted PregnancyDocument9 pagesStop Unsafe Sex: Impact On AIDS and Unwanted PregnancyTilahun MikiasNo ratings yet
- Pharmacological Activities of BioactiveDocument24 pagesPharmacological Activities of BioactiveDe'Uma Beiby SwettyNo ratings yet
- Album in CirrhosisDocument9 pagesAlbum in CirrhosisceciliaNo ratings yet
- 1 - Patient Evaluation, Diagnosis and Treatment PlanningDocument5 pages1 - Patient Evaluation, Diagnosis and Treatment PlanningMohammed100% (1)
- Wife Misses Intimacy: Tomorrow's HoroscopeDocument1 pageWife Misses Intimacy: Tomorrow's HoroscopeThe Delphos HeraldNo ratings yet
- Perth Sunday Times - Week 1 - 18/4/2010Document1 pagePerth Sunday Times - Week 1 - 18/4/2010John_Bishop_3317No ratings yet
- Journal-ATOPIC DERMATITISDocument16 pagesJournal-ATOPIC DERMATITISFourta LasoctoNo ratings yet
- Clinical Characteristics and Long Term Outcome of Taiwanese Children With Congenital HyperinsulinismDocument5 pagesClinical Characteristics and Long Term Outcome of Taiwanese Children With Congenital HyperinsulinismMer UtsavNo ratings yet
- USMLE Road Map ImmunologyDocument242 pagesUSMLE Road Map ImmunologyRomina RospigliosiNo ratings yet
- GM.007 Crossmatch Anti IgG Gel CardDocument10 pagesGM.007 Crossmatch Anti IgG Gel CardKarl GutierrezNo ratings yet
- Memmory Shit 1 2 1Document3 pagesMemmory Shit 1 2 1Cristian Radu100% (1)
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- How Alcohol Changes Your BodyDocument14 pagesHow Alcohol Changes Your BodyyuliNo ratings yet
- Causation and Prevention of Diseases: - Dr. Haryax PathakDocument12 pagesCausation and Prevention of Diseases: - Dr. Haryax PathakDr Ashish ManochaNo ratings yet
- InfidelityDocument5 pagesInfidelityDelya Blondya100% (1)
- Anti Nutritional FactorsDocument17 pagesAnti Nutritional FactorsMalvika Shah JainNo ratings yet
- Onychocryptosis - Decrypting The ControversiesDocument14 pagesOnychocryptosis - Decrypting The ControversiesVaneet RandNo ratings yet
- Acute CholecystitisDocument27 pagesAcute CholecystitisAleks MendozaNo ratings yet
- Countdown Mental Health Report 2030ƒDocument18 pagesCountdown Mental Health Report 2030ƒmaritasvNo ratings yet
- Levofloksasin Hemihidrat MsdsDocument6 pagesLevofloksasin Hemihidrat MsdsEsin KahramanNo ratings yet
- DCLRXLFHG PDFDocument144 pagesDCLRXLFHG PDFtoniledoNo ratings yet
- The Facilities Manager's Guide To M&E ComplianceDocument22 pagesThe Facilities Manager's Guide To M&E ComplianceTannice HemmingNo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) Virusshoaib chNo ratings yet
- Potential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsDocument18 pagesPotential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsSubhan Aristiadi RachmanNo ratings yet
- C S e Mains Old PaperDocument59 pagesC S e Mains Old PapermoolsinghNo ratings yet






















































































Download as ppt, pdf, or txt
You might also like
- DDAL04 Expanded Dark Gifts Table OPTIONAL CONTENT PDFDocument3 pagesDDAL04 Expanded Dark Gifts Table OPTIONAL CONTENT PDFDavidHavokNo ratings yet
- Basic Care & Comfort Nclex RN UwDocument10 pagesBasic Care & Comfort Nclex RN Uwgwen scribd100% (1)
- Amboss ECGDocument13 pagesAmboss ECGAllysahNo ratings yet
- General Practitioner - Pulmonology MCQsDocument37 pagesGeneral Practitioner - Pulmonology MCQsAsif Newaz100% (7)
- Ventilatory Assistance - Fall 2021Document36 pagesVentilatory Assistance - Fall 2021j dog100% (1)
- Bio 215 Topic 7 RespiratoryDocument46 pagesBio 215 Topic 7 RespiratoryYara BeainiNo ratings yet
- Respiratory SystemDocument90 pagesRespiratory SystemMaria MargaritaNo ratings yet
- RESPIRATORY-SYSTEM pptx1137Document32 pagesRESPIRATORY-SYSTEM pptx1137Jerick Sevilla SearesNo ratings yet
- Dyspnea in Children - Wahyuni IndawatiDocument20 pagesDyspnea in Children - Wahyuni IndawatiTarmidi MidziNo ratings yet
- Acute Respiratory Fauilr - PDF CVS PART 4Document61 pagesAcute Respiratory Fauilr - PDF CVS PART 4LexNo ratings yet
- Chap07 RespiratoryDocument44 pagesChap07 RespiratoryShere AlmansuoriNo ratings yet
- Chapter 11 - Respiratory SystemsDocument122 pagesChapter 11 - Respiratory Systemsnokate konkoorNo ratings yet
- VENTILATIONDocument27 pagesVENTILATIONezeudunicholas16No ratings yet
- OxygenationDocument50 pagesOxygenationLulu MushiNo ratings yet
- L4 - Common Disorders of Respiratory SystemDocument29 pagesL4 - Common Disorders of Respiratory SystemRand ELABEDNo ratings yet
- NCM 118Responses-to-Altered-Ventilatory-FunctionDocument169 pagesNCM 118Responses-to-Altered-Ventilatory-FunctionAddah, Dhenaraiza H.No ratings yet
- Dr. Sunita Saxena - Breathing and Exchange of GassesDocument48 pagesDr. Sunita Saxena - Breathing and Exchange of GassesDivya AgarawalNo ratings yet
- 8respiratory SystemDocument49 pages8respiratory SystemJack OneNo ratings yet
- HANDOUTS Finals CH 15Document24 pagesHANDOUTS Finals CH 15hii385156No ratings yet
- Lecture 6 Respiratory System 2Document33 pagesLecture 6 Respiratory System 2hafiz patahNo ratings yet
- NCM 112 OXYGENATION - HandoutDocument9 pagesNCM 112 OXYGENATION - Handoutissaiahnicolle100% (1)
- Module 3 PDF 2024Document16 pagesModule 3 PDF 2024gagansshemdiNo ratings yet
- Respiration SystemDocument49 pagesRespiration Systemfebe_aldellaNo ratings yet
- A QuickGuide On COPD 2022 - 0Document6 pagesA QuickGuide On COPD 2022 - 0housesofthelyricNo ratings yet
- M8 - Investigations and Monitoring in The ICUDocument68 pagesM8 - Investigations and Monitoring in The ICUVishal KumarNo ratings yet
- Respiratory SystemDocument192 pagesRespiratory SystemQuolette Constante100% (1)
- NCMB312M1CU3Document16 pagesNCMB312M1CU3Georgia De OcampoNo ratings yet
- NCMB 312 M1 Cu3Document16 pagesNCMB 312 M1 Cu3Georgia De OcampoNo ratings yet
- Gas Exchange and Alveoli 2Document18 pagesGas Exchange and Alveoli 213obasuyioNo ratings yet
- Report Ncm103Document68 pagesReport Ncm103john_mesa_5No ratings yet
- Gaseous Exchange in MammalsDocument35 pagesGaseous Exchange in Mammalsmahanswarnima08No ratings yet
- Respiratory SystemDocument6 pagesRespiratory SystemCraigNo ratings yet
- Hypoxemic Respiratory FailureDocument70 pagesHypoxemic Respiratory FailureMohamed Rikarz Ahamed RikarzNo ratings yet
- Basic Respiratory Mechanics (DR Arif)Document36 pagesBasic Respiratory Mechanics (DR Arif)Rizqi Luqmanul HakimNo ratings yet
- Respiratory SystemDocument24 pagesRespiratory SystemArjunNo ratings yet
- Respiration NotesDocument4 pagesRespiration NotesJana AldourNo ratings yet
- CODPDocument34 pagesCODPNeeraja M SureshNo ratings yet
- A Level Gaseous Exchange Continued - 032759Document13 pagesA Level Gaseous Exchange Continued - 032759onyangaismail12No ratings yet
- Final PhysioDocument1,111 pagesFinal PhysioSana Savana Aman R100% (1)
- Respiratorio-Openstax Biology2e ch39Document43 pagesRespiratorio-Openstax Biology2e ch39ANo ratings yet
- Oxygen Therapy, Trach Care and SuctioningDocument44 pagesOxygen Therapy, Trach Care and SuctioningEmily Boehmer100% (1)
- Respiratory System PhysiologyDocument35 pagesRespiratory System PhysiologySherwan R Shal100% (2)
- Ventilasi PerfusiDocument44 pagesVentilasi PerfusiIdahrachman515100% (1)
- ARDS With PathophysiologyDocument79 pagesARDS With Pathophysiologymabec pagaduan95% (19)
- Ventilasi Pulmonal Dan Diffusi Gas PernafasanDocument18 pagesVentilasi Pulmonal Dan Diffusi Gas PernafasanRaudhah RamadiyantikaNo ratings yet
- Respiratory PhysiologyDocument98 pagesRespiratory PhysiologySurya SuryaNo ratings yet
- Vent TherapyDocument10 pagesVent TherapychuhuaNo ratings yet
- Respiratory System The ElderlyDocument37 pagesRespiratory System The ElderlyDanica FrancoNo ratings yet
- Oxygenation 1 PDFDocument4 pagesOxygenation 1 PDFAbdullah Al NomanNo ratings yet
- 4-1pulmonary DisordersDocument38 pages4-1pulmonary DisordersAbdallah AlasalNo ratings yet
- Chap 12 RespirationDocument48 pagesChap 12 RespirationFungai MuganhuNo ratings yet
- Presentation Topic: Causes of Ventilation PerfusionDocument9 pagesPresentation Topic: Causes of Ventilation PerfusionAbDul RaufNo ratings yet
- Oxygenation Part 1Document86 pagesOxygenation Part 1Shaira Mae Fangon De GuzmanNo ratings yet
- Ventilation Perfusion Ratio & Diffusion of GasesDocument28 pagesVentilation Perfusion Ratio & Diffusion of GasesRiyaNo ratings yet
- Disorder ofDocument207 pagesDisorder ofyewollolijfikreNo ratings yet
- Distress RespiratoriopdfDocument11 pagesDistress RespiratoriopdfDiana CarolinaNo ratings yet
- Notes of Human Physiology Class 11Document9 pagesNotes of Human Physiology Class 11ADWAITH LALU100% (1)
- Pulmonary VentilationDocument12 pagesPulmonary Ventilationtan shin meiNo ratings yet
- Respiratory System: The Second HalfDocument35 pagesRespiratory System: The Second HalfnicopiiNo ratings yet
- B.8 Situation - Care of Client With Problems in OxygenationDocument11 pagesB.8 Situation - Care of Client With Problems in OxygenationSOLEIL LOUISE LACSON MARBASNo ratings yet
- Fundamentals - CH 40: Oxygenation/Gas Exchange: Nloa Sfe B.8 Situation - Care of Client With Problems in OxygenationDocument20 pagesFundamentals - CH 40: Oxygenation/Gas Exchange: Nloa Sfe B.8 Situation - Care of Client With Problems in OxygenationSOLEIL LOUISE LACSON MARBASNo ratings yet
- ImrozDocument57 pagesImrozSyed Imroz KhanNo ratings yet
- Pulmonary Function Tests in Clinical PracticeFrom EverandPulmonary Function Tests in Clinical PracticeAli AltalagRating: 5 out of 5 stars5/5 (1)
- Internet Addiction: Kimberly S. YoungDocument14 pagesInternet Addiction: Kimberly S. YoungKairat ParpiyevNo ratings yet
- Stop Unsafe Sex: Impact On AIDS and Unwanted PregnancyDocument9 pagesStop Unsafe Sex: Impact On AIDS and Unwanted PregnancyTilahun MikiasNo ratings yet
- Pharmacological Activities of BioactiveDocument24 pagesPharmacological Activities of BioactiveDe'Uma Beiby SwettyNo ratings yet
- Album in CirrhosisDocument9 pagesAlbum in CirrhosisceciliaNo ratings yet
- 1 - Patient Evaluation, Diagnosis and Treatment PlanningDocument5 pages1 - Patient Evaluation, Diagnosis and Treatment PlanningMohammed100% (1)
- Wife Misses Intimacy: Tomorrow's HoroscopeDocument1 pageWife Misses Intimacy: Tomorrow's HoroscopeThe Delphos HeraldNo ratings yet
- Perth Sunday Times - Week 1 - 18/4/2010Document1 pagePerth Sunday Times - Week 1 - 18/4/2010John_Bishop_3317No ratings yet
- Journal-ATOPIC DERMATITISDocument16 pagesJournal-ATOPIC DERMATITISFourta LasoctoNo ratings yet
- Clinical Characteristics and Long Term Outcome of Taiwanese Children With Congenital HyperinsulinismDocument5 pagesClinical Characteristics and Long Term Outcome of Taiwanese Children With Congenital HyperinsulinismMer UtsavNo ratings yet
- USMLE Road Map ImmunologyDocument242 pagesUSMLE Road Map ImmunologyRomina RospigliosiNo ratings yet
- GM.007 Crossmatch Anti IgG Gel CardDocument10 pagesGM.007 Crossmatch Anti IgG Gel CardKarl GutierrezNo ratings yet
- Memmory Shit 1 2 1Document3 pagesMemmory Shit 1 2 1Cristian Radu100% (1)
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- How Alcohol Changes Your BodyDocument14 pagesHow Alcohol Changes Your BodyyuliNo ratings yet
- Causation and Prevention of Diseases: - Dr. Haryax PathakDocument12 pagesCausation and Prevention of Diseases: - Dr. Haryax PathakDr Ashish ManochaNo ratings yet
- InfidelityDocument5 pagesInfidelityDelya Blondya100% (1)
- Anti Nutritional FactorsDocument17 pagesAnti Nutritional FactorsMalvika Shah JainNo ratings yet
- Onychocryptosis - Decrypting The ControversiesDocument14 pagesOnychocryptosis - Decrypting The ControversiesVaneet RandNo ratings yet
- Acute CholecystitisDocument27 pagesAcute CholecystitisAleks MendozaNo ratings yet
- Countdown Mental Health Report 2030ƒDocument18 pagesCountdown Mental Health Report 2030ƒmaritasvNo ratings yet
- Levofloksasin Hemihidrat MsdsDocument6 pagesLevofloksasin Hemihidrat MsdsEsin KahramanNo ratings yet
- DCLRXLFHG PDFDocument144 pagesDCLRXLFHG PDFtoniledoNo ratings yet
- The Facilities Manager's Guide To M&E ComplianceDocument22 pagesThe Facilities Manager's Guide To M&E ComplianceTannice HemmingNo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) Virusshoaib chNo ratings yet
- Potential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsDocument18 pagesPotential Application of Milk and Milk Products As Carrier For Herbs and NutraceuticalsSubhan Aristiadi RachmanNo ratings yet
- C S e Mains Old PaperDocument59 pagesC S e Mains Old PapermoolsinghNo ratings yet