Download as pptx, pdf, or txt
You might also like
- Tracheostomy Care Checklist 1Document2 pagesTracheostomy Care Checklist 1Nicholas Tagle100% (2)
- Exchange Transfusion SheetDocument2 pagesExchange Transfusion SheetWilda Awlia100% (1)
- Comprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFDocument530 pagesComprehensive Cardiovascular Medicine in The Primary Care Setting-Humana Press (2018) PDFHaribabu ArumugamNo ratings yet
- Pharmacology HandoutDocument5 pagesPharmacology HandoutMark Elben Teodoro100% (1)
- Fractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyasDocument90 pagesFractures of Forearm: Oktya Veny Simbolon Pattiyah Prehandini AyuningtyaspattiyahNo ratings yet
- Distal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Document40 pagesDistal Phalanx (45%) - Metacarpal (30%) - Proximal Phalanx (15%) - Middle Phalanx (10%)Dabessa MosissaNo ratings yet
- U04 Fxs of Humeral ShaftDocument88 pagesU04 Fxs of Humeral Shaftadrian_mogosNo ratings yet
- Forearm Fracture 1 BismillahDocument17 pagesForearm Fracture 1 Bismillahamel015No ratings yet
- Radial Fractures: Anthony Safi MEDIII Orthopedic Surgery RotationDocument22 pagesRadial Fractures: Anthony Safi MEDIII Orthopedic Surgery RotationAnthony safiNo ratings yet
- Fracture Shaft Humerus - 030014Document60 pagesFracture Shaft Humerus - 030014MohammedShahidNo ratings yet
- Humeral Shaft FractureDocument82 pagesHumeral Shaft FractureYoga AninditaNo ratings yet
- Upload Scribd 4Document7 pagesUpload Scribd 4Yoga AninditaNo ratings yet
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDocument57 pagesElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediNo ratings yet
- Fractures of The Humeral ShaftDocument25 pagesFractures of The Humeral ShaftMuhammad IqbalNo ratings yet
- Distal Radius FracturesDocument92 pagesDistal Radius FracturesAmel VnairNo ratings yet
- Injuries Around The ShoulderDocument81 pagesInjuries Around The ShoulderMisoNo ratings yet
- Tibia ProximalDocument51 pagesTibia Proximalchenth3r3No ratings yet
- Orthopedics and Surgery of The Hand and WristDocument157 pagesOrthopedics and Surgery of The Hand and Wristhemasunder903No ratings yet
- Distal Radial Injury: Department of Orthopaedics SGH Didactic LectureDocument52 pagesDistal Radial Injury: Department of Orthopaedics SGH Didactic Lecturedrscribd1No ratings yet
- Fracture Tibia & Fibula-1Document111 pagesFracture Tibia & Fibula-1Usaid SulaimanNo ratings yet
- Blue Writing Is What I Added To These Notes: RadiographyDocument46 pagesBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Injury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Document51 pagesInjury Around The Elbow: Mohamad Afiq Izzuddin 1001336000 Group 3Star CruiseNo ratings yet
- Fraktur Distal Humeri: Fracture ElbowDocument11 pagesFraktur Distal Humeri: Fracture ElbowDimas PrasetyoNo ratings yet
- 4 150512145223 Lva1 App6891Document40 pages4 150512145223 Lva1 App6891Rizky HandayaniNo ratings yet
- Femoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanDocument77 pagesFemoral Supracondylar Fractures: Prepared by Dr. Ramzy Sh. ShikhanRamzi ShukriNo ratings yet
- Hip FracturesDocument74 pagesHip FracturesMina SamirNo ratings yet
- 09.20-09.35 - DR - Dr.heri Suroto - When To OperateDocument80 pages09.20-09.35 - DR - Dr.heri Suroto - When To OperateJoseph WilsonNo ratings yet
- Forearm 150721101353 Lva1 App6891Document24 pagesForearm 150721101353 Lva1 App6891didiNo ratings yet
- Nursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDocument25 pagesNursing Management: Musculoskeletal Trauma and Orthopedic SurgeryDeannahTampusNo ratings yet
- ORP - Handout - English - Malleolar FracturesDocument15 pagesORP - Handout - English - Malleolar Fracturesadrian1989No ratings yet
- Patellar Fracture 1Document39 pagesPatellar Fracture 1Syafiq ShahbudinNo ratings yet
- Pembimbing: Dr. Husnul Fuad Albar, SpotDocument52 pagesPembimbing: Dr. Husnul Fuad Albar, Spotjananeesieadass916No ratings yet
- Fractures of Radius and Ulnar Shaft: Dima HabanjarDocument56 pagesFractures of Radius and Ulnar Shaft: Dima HabanjarDima HabanjarNo ratings yet
- Case Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1Document11 pagesCase Study of "Subtrochanteric Femur": Prepared By: John Ress A. Escobal Group 1J.r. MercadoNo ratings yet
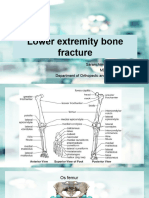
- Lower Extremity Bone Fracture Lecture 3Document88 pagesLower Extremity Bone Fracture Lecture 3Tselmeg TselmegNo ratings yet
- Distal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemDocument48 pagesDistal Humerus Fracture: Presentor:Dr Balaji Vinayaka Mission Kirubananda Variyar Medical College. SalemNicholas DelaliNo ratings yet
- Fraktur Radius UlnaDocument39 pagesFraktur Radius UlnaNur Awaliya FatimahNo ratings yet
- Proximal Humeral Fracture Repair and RehabilitationDocument8 pagesProximal Humeral Fracture Repair and RehabilitationAnonymous UClts4nYNo ratings yet
- Knee Tibia & Ankle InjuriesDocument88 pagesKnee Tibia & Ankle InjuriesNasser AlQadhibNo ratings yet
- Distal Radius and UlnaDocument40 pagesDistal Radius and UlnaDia CembranoNo ratings yet
- Fractures and Dislocations of The Mid-Foot Including Lisfranc InjuriesDocument67 pagesFractures and Dislocations of The Mid-Foot Including Lisfranc Injuriesmaria_meNo ratings yet
- Elbow and Shoulder Dislocation InjuriesDocument42 pagesElbow and Shoulder Dislocation InjuriesWizz Háķìm ĻêşòwNo ratings yet
- Clavicle AC SC JointsDocument97 pagesClavicle AC SC Jointsdr.maulanahutabaratNo ratings yet
- 2.supracondylar Humerus FracturesDocument26 pages2.supracondylar Humerus FracturesDabessa MosissaNo ratings yet
- Fracture of Distal HumerusDocument44 pagesFracture of Distal HumerusRamin MaharjanNo ratings yet
- Coronoid FractureDocument38 pagesCoronoid FractureRamin MaharjanNo ratings yet
- U10-Distal Radius FracturesDocument121 pagesU10-Distal Radius Fracturesrajasekhar ANo ratings yet
- Distal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurDocument76 pagesDistal End Humerus Fractures: BY:-Dr. Anshu Sharma Guide:-Dr.A.K. MathurToàn Đặng Phan VĩnhNo ratings yet
- Destal End RadiusDocument76 pagesDestal End Radiusahmed dabourNo ratings yet
- Fractures HFHDocument74 pagesFractures HFHEmmanuel Papa AcquahNo ratings yet
- Musculoskeletal Trauma Cases in Lower Extremities and Its ManagementDocument41 pagesMusculoskeletal Trauma Cases in Lower Extremities and Its ManagementAli AbdullahNo ratings yet
- Fracture It FemurDocument50 pagesFracture It FemurSonal RaikwarNo ratings yet
- Distal Radius FracturesDocument68 pagesDistal Radius Fracturescalvin_c_wangNo ratings yet
- Calcaneus Fracture: Randy SusantoDocument32 pagesCalcaneus Fracture: Randy SusantoRandy SusantoNo ratings yet
- Fractures of The Upper Limb: Dr. Salman AbbasiDocument60 pagesFractures of The Upper Limb: Dr. Salman AbbasiSeimal MahmoodNo ratings yet
- Upper Extremity TraumaDocument50 pagesUpper Extremity Traumaoppongeric388No ratings yet
- Colles FractureDocument32 pagesColles FractureAndi KurniawanNo ratings yet
- Scaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FractureDocument61 pagesScaphoid Fracture, Bennett'S Fracture, Metacarpels, Phalanges FracturesenthilNo ratings yet
- (Peserta) Bedah 2 - Mantap Februari 2017Document211 pages(Peserta) Bedah 2 - Mantap Februari 2017karno0% (1)
- Scaphoid FractureDocument77 pagesScaphoid FractureTanuGarg100% (1)
- Humerus Shaft FracturesDocument60 pagesHumerus Shaft Fracturesoppongeric388No ratings yet
- Fractures of The Shaft of Radius and UlnaDocument54 pagesFractures of The Shaft of Radius and Ulnadrakkashmiri100% (1)
- Shoulder InjuriesDocument33 pagesShoulder InjuriesWizz Háķìm ĻêşòwNo ratings yet
- Reduction, Relocation and Splinting in Emergency Room (RASER)From EverandReduction, Relocation and Splinting in Emergency Room (RASER)No ratings yet
- Date and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcomeDocument8 pagesDate and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcometrizzlecNo ratings yet
- Guidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresDocument21 pagesGuidelines For Data Collection On The American Nurses Association's National Quality Forum Endorsed MeasuresMaria Fudji HastutiNo ratings yet
- Breathe Light To Breathe Right - PDF RoomDocument58 pagesBreathe Light To Breathe Right - PDF Roomfabricio100% (3)
- Reasearch Aloe Vera As A Hand SanitizerDocument4 pagesReasearch Aloe Vera As A Hand SanitizerRosenda ColumnaNo ratings yet
- N A - D (Nsaid) : Onsteroidal NTI Inflammatory Rugs SDocument43 pagesN A - D (Nsaid) : Onsteroidal NTI Inflammatory Rugs STes B FourieNo ratings yet
- Fsoc 05 540478Document5 pagesFsoc 05 540478tryan693No ratings yet
- Acute Fatty Liver of Pregnancy - V2.1 - GL780Document5 pagesAcute Fatty Liver of Pregnancy - V2.1 - GL780Ade PurnaNo ratings yet
- Nursing Practice QuestionsDocument22 pagesNursing Practice QuestionsMonique RapleyNo ratings yet
- Pitfalls On NephrometryDocument1 pagePitfalls On NephrometryGaltieri OtavioNo ratings yet
- Department of Pharmacy-Online Class Routine-Spring 2021 Duration of Class: 1.5 HRDocument4 pagesDepartment of Pharmacy-Online Class Routine-Spring 2021 Duration of Class: 1.5 HRSahria RahmanNo ratings yet
- Medical Billing TrainingDocument11 pagesMedical Billing TrainingHarry Canaba100% (1)
- RNTCPDocument30 pagesRNTCPDeepa SharmaNo ratings yet
- EM Case Write UpDocument11 pagesEM Case Write UpRaihana Rafi100% (2)
- International Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobDocument5 pagesInternational Journal of Women's Dermatology: Mohsen Baghchechi, Jeffery Dunn, Navin Jaipaul, Sharon E. JacobR JNo ratings yet
- Common Drugs in Pet PracticeDocument2 pagesCommon Drugs in Pet Practiceshahbaz zafarNo ratings yet
- Results of Cancer Treatment at DarfDocument4 pagesResults of Cancer Treatment at DarfWashington AmericaNo ratings yet
- Immunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacuteDocument10 pagesImmunopathology of Vesicular Cutaneous Lupus Erythematosus in The Rough Collie and Shetland Sheepdog - A Canine Homologue of SubacutejenNo ratings yet
- EBM and EconomicsDocument14 pagesEBM and EconomicsSofyan HarahapNo ratings yet
- Inst Branchwise Mds 301022Document15 pagesInst Branchwise Mds 301022White WolfNo ratings yet
- Unit 4 Heath TopicDocument32 pagesUnit 4 Heath Topicralph allan bibatNo ratings yet
- UrologyDocument29 pagesUrologyAnonymous MtKJkerbpU100% (1)
- Drug Information Services 1Document8 pagesDrug Information Services 1Rashmi RajNo ratings yet
- Amang Rodriguez (Armmc)Document9 pagesAmang Rodriguez (Armmc)Ralph AlbertoNo ratings yet
- CertificateDocument1 pageCertificatesnehal shelakeNo ratings yet
- (NCP) Deficient Fluid Volume - HypovolemiaDocument3 pages(NCP) Deficient Fluid Volume - HypovolemiaMacaRonie PepeRownie del Rio100% (4)
- Abbreviated Mental Test Score - WikipediaDocument4 pagesAbbreviated Mental Test Score - WikipediaFrancisco DionicioNo ratings yet