Download as ppt, pdf, or txt
You might also like
- Exam 2 Study Guide-2Document5 pagesExam 2 Study Guide-2Enoch SuhNo ratings yet
- The Menace of MRSADocument51 pagesThe Menace of MRSArsborromeoNo ratings yet
- Jurnal Mikro 1Document6 pagesJurnal Mikro 1Elang SudewaNo ratings yet
- Emerging InfectionDocument49 pagesEmerging InfectionTaufan LutfiNo ratings yet
- Wound Infections and MRSA: Marvin J. Bittner MDDocument93 pagesWound Infections and MRSA: Marvin J. Bittner MDOsama HassanNo ratings yet
- Antibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Document25 pagesAntibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Anggara DwiputraNo ratings yet
- 3 Common Infectious Problems in PediatricsDocument102 pages3 Common Infectious Problems in PediatricsRajeshNo ratings yet
- Imunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionDocument90 pagesImunisasi Pada Kesehatan Masyarakat Di Indonesia Dan Pelaksanaan Safe InjectionPuji Arifianti RamadhanyNo ratings yet
- Where Do We Stand On Periprosthetic Joint InfectionDocument71 pagesWhere Do We Stand On Periprosthetic Joint InfectionneareastspineNo ratings yet
- Teh 2014Document4 pagesTeh 2014Mario ChristopherNo ratings yet
- The Importance of AdherenceDocument28 pagesThe Importance of AdherenceVijay LaptopNo ratings yet
- Antibiotic Resistant Pathogens: Impact and ControlDocument98 pagesAntibiotic Resistant Pathogens: Impact and ControlNur ElidaNo ratings yet
- GeptodacinDocument6 pagesGeptodacinRubí YeverinoNo ratings yet
- Shorter Treatment Duration For Selected Patients With Multidrug-Resistant TuberculosisDocument4 pagesShorter Treatment Duration For Selected Patients With Multidrug-Resistant Tuberculosispooja thanekarNo ratings yet
- NAP (Harry P.) PDFDocument29 pagesNAP (Harry P.) PDFaldyNo ratings yet
- Antibiotic Optimization in CIAIDocument33 pagesAntibiotic Optimization in CIAIAditya Pradana KNo ratings yet
- Prevention Strategy of Infectious Diseases For Health Care WorkersDocument31 pagesPrevention Strategy of Infectious Diseases For Health Care WorkersarinNo ratings yet
- Linezolida NovoDocument6 pagesLinezolida NovoGabriel EstevesNo ratings yet
- 2015-2016 Annual Report of Immunization Status Texas Department of State Health Services Immunization BranchDocument3 pages2015-2016 Annual Report of Immunization Status Texas Department of State Health Services Immunization BranchStephen YoungNo ratings yet
- Vicenzoni Et Al. - 2000 - Sensitivity To Rifaximin of Strains of Staphylococcus Aureus Isolated From 1997 To 1999 - Comparison Between Years and Calculation of The Correlated MICDocument5 pagesVicenzoni Et Al. - 2000 - Sensitivity To Rifaximin of Strains of Staphylococcus Aureus Isolated From 1997 To 1999 - Comparison Between Years and Calculation of The Correlated MICmktexportNo ratings yet
- Hicc For Nursing Excellence-Smh Sept 2018Document25 pagesHicc For Nursing Excellence-Smh Sept 2018RakshaNo ratings yet
- Candidiasis in HIVDocument34 pagesCandidiasis in HIVRafif Abdurrahman WijisaksonoNo ratings yet
- Malaysia: Tuberculosis ProfileDocument1 pageMalaysia: Tuberculosis ProfileUp ApNo ratings yet
- T. Schaberg, K. Rebhan, H. LodeDocument5 pagesT. Schaberg, K. Rebhan, H. LodeErika ArnitaNo ratings yet
- AMS - Collateral DamageDocument29 pagesAMS - Collateral DamageShajahan SideequeNo ratings yet
- RSA的診斷、治療與醫院感染管制Document83 pagesRSA的診斷、治療與醫院感染管制李英誠No ratings yet
- A Population-Based Study of First and Second-Line Drug-Resistant Tuberculosis in A High-Burden Area of The Mexico/United States BorderDocument7 pagesA Population-Based Study of First and Second-Line Drug-Resistant Tuberculosis in A High-Burden Area of The Mexico/United States BordercyclonzNo ratings yet
- Lessons From The Coronavirus Disease 2019 Pandemic: Will Virtual Patient Management Reshape Uro-Oncology in Germany?Document5 pagesLessons From The Coronavirus Disease 2019 Pandemic: Will Virtual Patient Management Reshape Uro-Oncology in Germany?Ion CorbuNo ratings yet
- These Highly Resistant Organisms Deserve Special Attention in Healthcare Facilities CDCDocument12 pagesThese Highly Resistant Organisms Deserve Special Attention in Healthcare Facilities CDCdianNo ratings yet
- Comment: The Lancet Oncology, Jianbo Tian and Colleagues IncludedDocument3 pagesComment: The Lancet Oncology, Jianbo Tian and Colleagues Includedkayegi8666No ratings yet
- The Clinical Relevance of Microbiology Specimens in Head and Neck Space Infections of Odontogenic OriginDocument3 pagesThe Clinical Relevance of Microbiology Specimens in Head and Neck Space Infections of Odontogenic OriginkaarlaamendezNo ratings yet
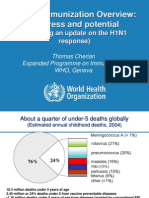
- Global Immunization Overview: Progress and PotentialDocument36 pagesGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNo ratings yet
- BM 2.3 Murti AndriastutiDocument27 pagesBM 2.3 Murti AndriastutiAbdullah ShiddiqNo ratings yet
- Diekema2019 PDFDocument31 pagesDiekema2019 PDFPurbosari KusumaNo ratings yet
- CCO Cytokine TX in MM ExpressPointsDocument18 pagesCCO Cytokine TX in MM ExpressPointsveaceslav coscodanNo ratings yet
- Impact of Empiric Antibiotics For Methicillin-Resistant Staphylococcus Aureus (MRSA) Infection and Associated Clostridioides Difficile Infection (CDI) Risk - Secondary Analysis of The CLEAR TrialDocument4 pagesImpact of Empiric Antibiotics For Methicillin-Resistant Staphylococcus Aureus (MRSA) Infection and Associated Clostridioides Difficile Infection (CDI) Risk - Secondary Analysis of The CLEAR TrialLee Foo WengNo ratings yet
- 98668Document6 pages98668SyedFaridAliNo ratings yet
- Measures of Morbidity 2022Document50 pagesMeasures of Morbidity 2022Kanwal KhanNo ratings yet
- Approaches To Febrile Neutropenia 2011 IDSA-ECIL GuidelinesDocument24 pagesApproaches To Febrile Neutropenia 2011 IDSA-ECIL GuidelinesHusein AssagafNo ratings yet
- Community Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasDocument48 pagesCommunity Acquired Mrsa: Pisespong Patamasucon, M.D. Pediatric Infectious Disease UNSOM - Las VegasRashed NazzalNo ratings yet
- Principles of Treating Infectious Illnesses in Critical Care: Focus On Antibiotic Resistance and ChoiceDocument65 pagesPrinciples of Treating Infectious Illnesses in Critical Care: Focus On Antibiotic Resistance and ChoiceIan OrwaNo ratings yet
- Tuberculosis: Etiology, Epidemiology, Pathogenesis, Clinical ManifestationDocument34 pagesTuberculosis: Etiology, Epidemiology, Pathogenesis, Clinical ManifestationGEORGENo ratings yet
- Central LinesDocument19 pagesCentral LinesJosef TrapaniNo ratings yet
- 04.Dose ที่เหมาะสมของ fosfomycin ใน CREDocument14 pages04.Dose ที่เหมาะสมของ fosfomycin ใน CRENattawat TeerawattanapongNo ratings yet
- Reporte Tuberculosis Venezuela 2018Document1 pageReporte Tuberculosis Venezuela 2018marco.boy2202No ratings yet
- Bacteriological Profile and Antibiogram of Surgical Site Infection at A Tertiary Care Hospital, Aurangabad, MaharashtraDocument13 pagesBacteriological Profile and Antibiogram of Surgical Site Infection at A Tertiary Care Hospital, Aurangabad, MaharashtraIJAR JOURNALNo ratings yet
- ER BC Clin Endpoints FULLDECKDocument47 pagesER BC Clin Endpoints FULLDECKmaleticjNo ratings yet
- Global Dan Nasional Problem AMR 2019Document36 pagesGlobal Dan Nasional Problem AMR 2019DewiNo ratings yet
- Ijmlr231702 PDFDocument7 pagesIjmlr231702 PDFsandeep raiNo ratings yet
- Determinants of Vancomycin Use in Adult Intensive Care Units in 41 United States HospitalsDocument7 pagesDeterminants of Vancomycin Use in Adult Intensive Care Units in 41 United States HospitalsGayan KarunanandaNo ratings yet
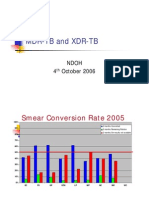
- MDR-TB and XDR-TB: Ndoh 4 October 2006Document40 pagesMDR-TB and XDR-TB: Ndoh 4 October 2006Eta Calvin ObenNo ratings yet
- Hepatitis A and Hepatitis A VaccineDocument31 pagesHepatitis A and Hepatitis A VaccinedydinNo ratings yet
- 1 s2.0 S0954611121000974 MainDocument4 pages1 s2.0 S0954611121000974 MainRuanPabloNo ratings yet
- VCU 2022 Neurosurgery Research Day TalkDocument21 pagesVCU 2022 Neurosurgery Research Day TalkAndrew CarasNo ratings yet
- Silver StudyDocument8 pagesSilver Studyapi-261829418No ratings yet
- WHO - HQ - Reports G2 PROD EXT TBCountryProfileDocument1 pageWHO - HQ - Reports G2 PROD EXT TBCountryProfileAngelo Santos EstrellaNo ratings yet
- MDRO Management: Infection Control Committee TeamDocument32 pagesMDRO Management: Infection Control Committee TeammaeNo ratings yet
- Aac 01818-17Document17 pagesAac 01818-17teranrobleswaltergabrielNo ratings yet
- Infection Control Webinar 16022010Document88 pagesInfection Control Webinar 16022010shyamchepurNo ratings yet
- Measles FM S 05072013Document42 pagesMeasles FM S 05072013Suhazeli AbdullahNo ratings yet
- Therapy Response Imaging in OncologyFrom EverandTherapy Response Imaging in OncologyMizuki NishinoNo ratings yet
- Algoritma LGIB and UGIB 2016Document18 pagesAlgoritma LGIB and UGIB 2016Dermawan SolehNo ratings yet
- Update On Invasive Fungal Infections Management in A Emergence of Anti Fungal Resistance EraDocument57 pagesUpdate On Invasive Fungal Infections Management in A Emergence of Anti Fungal Resistance EraDermawan SolehNo ratings yet
- Pra PPDSDocument10 pagesPra PPDSDermawan SolehNo ratings yet
- Estimation of PO2 and FiO2Document1 pageEstimation of PO2 and FiO2Dermawan SolehNo ratings yet
- CAP GuideDocument2 pagesCAP GuideDermawan SolehNo ratings yet
- Gram Pozitive CocciDocument47 pagesGram Pozitive CocciJedjdjdjdjdhjdNo ratings yet
- Bacteremia - StatPearls - NCBI Bookshelf EnglishDocument5 pagesBacteremia - StatPearls - NCBI Bookshelf EnglishKhalda Sausan AzharNo ratings yet
- Author Anthony W Chow, MD, FRCPC, FACP Section Editor Stephen B Calderwood, MD Deputy Editor Allyson Bloom, MDDocument16 pagesAuthor Anthony W Chow, MD, FRCPC, FACP Section Editor Stephen B Calderwood, MD Deputy Editor Allyson Bloom, MDSiska HarapanNo ratings yet
- SHC Antimicrobial Prophylaxis in Surgery RecommendationsDocument3 pagesSHC Antimicrobial Prophylaxis in Surgery RecommendationsCatherine MorrisNo ratings yet
- Nosocomial PneumoniaDocument37 pagesNosocomial PneumoniaWinson ChitraNo ratings yet
- MRSA Pre-ScreeningDocument17 pagesMRSA Pre-ScreeningAziz Khan JadoonNo ratings yet
- PN ChromogenicMediaDocument12 pagesPN ChromogenicMediaNguyen Ngoc ThachNo ratings yet
- Biosynthesis, Characterization and Antibacterial Activity of Silver and Gold Nanoparticles From The Leaf and Bark Extracts of Zanthoxylum CapenseDocument101 pagesBiosynthesis, Characterization and Antibacterial Activity of Silver and Gold Nanoparticles From The Leaf and Bark Extracts of Zanthoxylum CapenseBira AdrianaNo ratings yet
- UPDATED Ayaan ALL CHAPTERDocument87 pagesUPDATED Ayaan ALL CHAPTERAadan CabduqaadirNo ratings yet
- AM CladDocument5 pagesAM CladJob ANo ratings yet
- Nle 3Document6 pagesNle 3Aijem RyanNo ratings yet
- Microbiology Flowchart Dr. NikitaDocument2 pagesMicrobiology Flowchart Dr. NikitaKshitij Singh RajputNo ratings yet
- InfectionDocument96 pagesInfectionBassem Georguos LabibNo ratings yet
- Bacteria ChartsDocument11 pagesBacteria ChartsFlowerNo ratings yet
- Dissertation On Ventilator Associated PneumoniaDocument6 pagesDissertation On Ventilator Associated PneumoniaInstantPaperWriterSingapore100% (1)
- Mrsa Thesis PDFDocument5 pagesMrsa Thesis PDFjenwilsongrandrapids100% (1)
- Surgical Antibiotic Prophylaxis Neurosurgery Adult and Paediatric PatientsDocument6 pagesSurgical Antibiotic Prophylaxis Neurosurgery Adult and Paediatric PatientsPraveen PadalaNo ratings yet
- British Journal of Biomedical Science Allicin Vs MRSADocument4 pagesBritish Journal of Biomedical Science Allicin Vs MRSAdolpretNo ratings yet
- Antimicrobial Susceptibility Testing PDFDocument19 pagesAntimicrobial Susceptibility Testing PDFdatitoxNo ratings yet
- Antibiotic Sensitivity Test and DrugDocument3 pagesAntibiotic Sensitivity Test and DrugRajeshNo ratings yet
- Atopic Dermatitis: Skin-Directed Management: Clinical ReportDocument12 pagesAtopic Dermatitis: Skin-Directed Management: Clinical ReportDenia Haritsa AprilianiNo ratings yet
- The Role of The Public Toilet Pathogen Transmitter PDFDocument16 pagesThe Role of The Public Toilet Pathogen Transmitter PDFNaresh ThakurNo ratings yet
- Antimicrobial Drugs: Prof DR Thamer Mutlag JasimDocument51 pagesAntimicrobial Drugs: Prof DR Thamer Mutlag JasimFlorinda PllanaNo ratings yet
- Assessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2Document45 pagesAssessment of Antibiotic Utilization in Sepsis Order Sets Initiated in The Emergency Department Draft 2api-652562554No ratings yet
- 2023 Update On Sepsis and Septic Shock in Adult Patients: Management in The Emergency DepartmentDocument24 pages2023 Update On Sepsis and Septic Shock in Adult Patients: Management in The Emergency DepartmentDanilo RetanaNo ratings yet
- Staphylococcus Aureus Biofilms Interfere With Macrophage AntimicrDocument175 pagesStaphylococcus Aureus Biofilms Interfere With Macrophage AntimicrshalusinhaNo ratings yet
- Microban PDFDocument56 pagesMicroban PDFCydelta FixsNo ratings yet
- Cipla Product ListDocument33 pagesCipla Product ListSumit Singhania100% (2)
- Nursing Care For Patient With HIV AIDSDocument28 pagesNursing Care For Patient With HIV AIDSDessyana Paulus100% (1)