Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cognitive Psychology Connecting Mind Research and Everyday Experience Goldstein 4th Edition Test BankDocument24 pagesCognitive Psychology Connecting Mind Research and Everyday Experience Goldstein 4th Edition Test BankNancyGarciakprq98% (48)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Anatomy and Physiology of BloodDocument9 pagesAnatomy and Physiology of BloodLharra Cagulada-PostranoNo ratings yet
- Milk Hygiene 4 (1) .PPT Revised April 2016Document92 pagesMilk Hygiene 4 (1) .PPT Revised April 2016ashley-keaneNo ratings yet
- Integumentary SystemDocument24 pagesIntegumentary SystemlloydNo ratings yet
- New England Journal of Medicine Volume 383 Issue 19 2020 (Doi 10.1056 - NEJMra1915327) Ropper, Allan H. Ashina, Messoud - MigraineDocument11 pagesNew England Journal of Medicine Volume 383 Issue 19 2020 (Doi 10.1056 - NEJMra1915327) Ropper, Allan H. Ashina, Messoud - MigraineMarija Sekretarjova100% (1)
- Exercise For Set For The KidneysDocument5 pagesExercise For Set For The KidneysRaja GuruNo ratings yet
- Guidelines For Writing Learning ObjectivesDocument1 pageGuidelines For Writing Learning Objectivesashley-keaneNo ratings yet
- ECG PracticeDocument12 pagesECG Practiceashley-keaneNo ratings yet
- Inhaled Anesthetics Part 1Document30 pagesInhaled Anesthetics Part 1ashley-keaneNo ratings yet
- CBL Anatomy of Vertebral ColumnDocument6 pagesCBL Anatomy of Vertebral Columnashley-keaneNo ratings yet
- Sexual Reproduction in Humans - Gamete Transfer and FertilisationDocument15 pagesSexual Reproduction in Humans - Gamete Transfer and Fertilisationashley-keaneNo ratings yet
- Final ProjectDocument58 pagesFinal ProjectAnonymous UyGHBJUNo ratings yet
- What Is A Cell? Describe The Functions of OrganellesDocument18 pagesWhat Is A Cell? Describe The Functions of Organellestdukes546No ratings yet
- Properties of The Plasma ProcoagulantsDocument4 pagesProperties of The Plasma ProcoagulantsBabylene MamauagNo ratings yet
- Anatomy Study Question Chp3Document10 pagesAnatomy Study Question Chp3Hema JothyNo ratings yet
- The Effect of Herings Law On Different Ptosis RepaDocument8 pagesThe Effect of Herings Law On Different Ptosis RepaPutra TridiyogaNo ratings yet
- HPLC Column Selection GuideDocument2 pagesHPLC Column Selection GuideMilena SegatoNo ratings yet
- Biological Correlates of Reiki Touch HealingDocument7 pagesBiological Correlates of Reiki Touch HealinglapastorinhaNo ratings yet
- Extrapyramidal Disorders, OedemaDocument104 pagesExtrapyramidal Disorders, OedemaAyman RehmanNo ratings yet
- Termografia: Uma Ferramenta de Auxílio No Diagnóstico Fisioterapêutico - Revisão de LiteraturaDocument21 pagesTermografia: Uma Ferramenta de Auxílio No Diagnóstico Fisioterapêutico - Revisão de Literaturabrunotaciano8628No ratings yet
- Biology Esei STPM 2017@ 2018Document43 pagesBiology Esei STPM 2017@ 2018Wei Yuen100% (1)
- Food Chemistry: Zhao Li, Ken Scott, Yacine Hemar, Huoming Zhang, Don OtterDocument7 pagesFood Chemistry: Zhao Li, Ken Scott, Yacine Hemar, Huoming Zhang, Don OtterAlexander VillaNo ratings yet
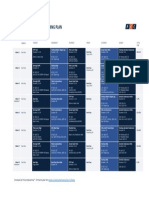
- 8 Weeks Gran Fondo OverivewDocument1 page8 Weeks Gran Fondo OverivewBorkoArsovicNo ratings yet
- Oxygen Hemoglobin Dissociation Curves PDFDocument2 pagesOxygen Hemoglobin Dissociation Curves PDFAnderson LondoñoNo ratings yet
- Lipids Function and StructureDocument58 pagesLipids Function and StructureTeddy K KunongNo ratings yet
- Adenosine DeaminaseDocument15 pagesAdenosine DeaminasemahirahNo ratings yet
- Carlini 2003Document12 pagesCarlini 2003ditaNo ratings yet
- The Plant Cell Wall: Growth and DevelopmentDocument29 pagesThe Plant Cell Wall: Growth and DevelopmentbeneNo ratings yet
- Kumar - Robbins and Cotran Pathological Basis of Disease 8eDocument3 pagesKumar - Robbins and Cotran Pathological Basis of Disease 8eKamila Anna Jakubowicz67% (3)
- Exercise 10 13Document5 pagesExercise 10 13Virlin Rose MahinayNo ratings yet
- 10 SSI Bundle 'Use CATS To Prevent SSI'Document53 pages10 SSI Bundle 'Use CATS To Prevent SSI'KPJConference100% (2)
- Ecg PresentationDocument27 pagesEcg Presentationanish3189No ratings yet
- Chapter 20 - MolluscaGastropoda CompressedDocument27 pagesChapter 20 - MolluscaGastropoda Compressedaulia rahmahNo ratings yet
- Burns & EscharotomyDocument36 pagesBurns & Escharotomyhatem alsrour100% (2)
- APCH1 - Single Chain Antibody For Vaccine TargetingDocument6 pagesAPCH1 - Single Chain Antibody For Vaccine TargetingAgustín OstachukNo ratings yet
- Tarka 12 Yoga and NeuroscienceDocument123 pagesTarka 12 Yoga and NeuroscienceEloNo ratings yet