Download as ppt, pdf, or txt
You might also like
- Tratado de PsiquiatriaDocument31 pagesTratado de Psiquiatriafisiojim33% (6)
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Common Psychiatric TermsDocument6 pagesCommon Psychiatric TermsKatrina Heart Rauto AvilaNo ratings yet
- About The Measure Domain MeasureDocument3 pagesAbout The Measure Domain MeasureMaríaA.SerranoNo ratings yet
- AdhdDocument5 pagesAdhdAndreea VanăNo ratings yet
- Manual For The Cognitive Therapy Rating Scale For Children and AdolescentsDocument22 pagesManual For The Cognitive Therapy Rating Scale For Children and AdolescentsAlberto EstradaNo ratings yet
- Psychopharmacology 1Document7 pagesPsychopharmacology 1RajP01No ratings yet
- Psychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDocument80 pagesPsychiatric Agents: By: Paula Rose Mae Cuario Evita Lalaine Del Mundo Dennis Ragudo Sheena ZarsueloDennis RagudoNo ratings yet
- Overview of Psychotropic DrugsDocument7 pagesOverview of Psychotropic Drugsnad101No ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- AntipsychoticsDocument10 pagesAntipsychoticswawing16No ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDocument6 pagesAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord Verazon100% (1)
- Sudden Onset (Within 2 Weeks) of at Least One of TheDocument2 pagesSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaNo ratings yet
- Schizophrenia: Signs and SymptomsDocument38 pagesSchizophrenia: Signs and SymptomsRatu Nurul Fadhilah100% (1)
- Introduction To NeuropharmacologyDocument6 pagesIntroduction To Neuropharmacologyammarhafez78100% (1)
- SchizophreniaDocument22 pagesSchizophrenianabeelNo ratings yet
- Antipsychotic Drugs - Wafa Bin ShamlanDocument8 pagesAntipsychotic Drugs - Wafa Bin ShamlanSara AbdoNo ratings yet
- Short Guide To Psychiatric DrugsDocument17 pagesShort Guide To Psychiatric Drugsjaume1010No ratings yet
- Psych Ch. 5 NotesDocument7 pagesPsych Ch. 5 NotesHaylle ThomasNo ratings yet
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- Atypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateDocument16 pagesAtypical Antidepressants - Pharmacology, Administration, and Side Effects - UpToDateMelissandreNo ratings yet
- Psycho Pharmacology - FinalDocument145 pagesPsycho Pharmacology - FinalKane CruzNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Psychotropic Medication ReviewDocument7 pagesPsychotropic Medication ReviewAakash Shah100% (2)
- Pharmacotherapy in PschiatryDocument8 pagesPharmacotherapy in PschiatryygfhdgNo ratings yet
- Anti PsychoticsDocument34 pagesAnti Psychotics88AKKNo ratings yet
- PsychopharmacologyDocument148 pagesPsychopharmacologyAsther Mantua100% (2)
- Shortened REM Latency and Increased REM: Previous AttemptDocument19 pagesShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenNo ratings yet
- Psychotropic Drugs.Document15 pagesPsychotropic Drugs.Xiaoqing SongNo ratings yet
- Antidepressants and AntipsychoticsDocument50 pagesAntidepressants and AntipsychoticsPintu Bhushan MitraNo ratings yet
- Psychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Document28 pagesPsychiatry Notes Psychiatry Notes: Medicine (Queen Mary University of London) Medicine (Queen Mary University of London)Noman ButtNo ratings yet
- Pharmacology in PsychiatryDocument33 pagesPharmacology in PsychiatryKatrina PonceNo ratings yet
- AntipsychoticsDocument4 pagesAntipsychoticsRana MuhammadNo ratings yet
- DSM-IV Criteria MnemonicsDocument4 pagesDSM-IV Criteria Mnemonicsleonyap100% (2)
- Study Guide Test 1Document11 pagesStudy Guide Test 1jwasylow13No ratings yet
- Dementia: Diagnosis and TreatmentDocument53 pagesDementia: Diagnosis and Treatmentakashdeep050% (1)
- 10 Cognitive DisordersDocument16 pages10 Cognitive DisordersFarrah MaeNo ratings yet
- Pharmacology - (5) Psychotic DrugsDocument8 pagesPharmacology - (5) Psychotic DrugsSamantha DiegoNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- Psych Ch. 7 Notes (Tutor)Document5 pagesPsych Ch. 7 Notes (Tutor)Haylle ThomasNo ratings yet
- Preferentially Block Uptake of 5-HT Preferentially Block Uptake of NADocument3 pagesPreferentially Block Uptake of 5-HT Preferentially Block Uptake of NAThư Phạm100% (1)
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Document3 pagesHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNo ratings yet
- Anti PsychoticDocument1 pageAnti PsychoticbeautyNo ratings yet
- Psych Meds 2Document2 pagesPsych Meds 2Cole SchaferNo ratings yet
- Pharmacology (1) - 104-122Document19 pagesPharmacology (1) - 104-122Dental LecturesMMQNo ratings yet
- B2B Psychopharmacology 2015Document128 pagesB2B Psychopharmacology 2015Soleil DaddouNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Medication Conversion ChartDocument2 pagesMedication Conversion ChartIlinca mirnoviciNo ratings yet
- Practical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryDocument29 pagesPractical Psychopharmacology in Children and Adolescents: Anoop Vermani MD Fellow, Child and Adolescent PsychiatryShahinaz ShamsNo ratings yet
- B /G C U I R: Anti-PsychoticsDocument2 pagesB /G C U I R: Anti-PsychoticsErsy Sakti ilhamNo ratings yet
- Specific Drug Olanzapine (Classification IndicationDocument14 pagesSpecific Drug Olanzapine (Classification IndicationRIZZA JANE VELASCONo ratings yet
- Psychiatric Medications in Pregnancy and LactationDocument27 pagesPsychiatric Medications in Pregnancy and LactationSunija SelvamNo ratings yet
- Anidepressant Drugs: Pratik KhanalDocument37 pagesAnidepressant Drugs: Pratik KhanalPratik Khanal100% (1)
- Psychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthDocument72 pagesPsychotropic Medications: Dale Sanderson, PA-C Physician Assistant Seattle Mental HealthMichael Urrutia100% (2)
- Drug List Psych Optho NeuroDocument22 pagesDrug List Psych Optho NeuroAshley BarrileNo ratings yet
- 504 - Pediatric Psychopharmacology - General PrinciplesDocument54 pages504 - Pediatric Psychopharmacology - General PrinciplesAlvaro HuidobroNo ratings yet
- ANTIPSYCHOTICSDocument25 pagesANTIPSYCHOTICSCheetahboi Shopee100% (4)
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
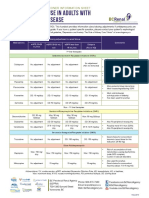
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- PsychopharmacologyDocument50 pagesPsychopharmacologyapi-3703352No ratings yet
- Antidepressant Therapy AlgorithmDocument12 pagesAntidepressant Therapy AlgorithmZubair Mahmood KamalNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (2)
- Nicotine Related DisordersDocument74 pagesNicotine Related DisordersKuldeep singhNo ratings yet
- Novel Systemic Treatments For Brain Metastases From Lung CancerDocument17 pagesNovel Systemic Treatments For Brain Metastases From Lung CancerOslo SaputraNo ratings yet
- 2 PB PDFDocument6 pages2 PB PDFOslo SaputraNo ratings yet
- We Therell 2009Document10 pagesWe Therell 2009Oslo SaputraNo ratings yet
- Neurological Disorders Report WebsiteDocument11 pagesNeurological Disorders Report WebsiteOslo SaputraNo ratings yet
- Pe 2 3 36Document6 pagesPe 2 3 36Oslo SaputraNo ratings yet
- 13 08 EMDR Carolina House Durham Handouts 1Document13 pages13 08 EMDR Carolina House Durham Handouts 1Oslo SaputraNo ratings yet
- 2 Shapiro F 2012 EMDR Therapy 2Document3 pages2 Shapiro F 2012 EMDR Therapy 2Oslo SaputraNo ratings yet
- Finkelstein DissertationDocument362 pagesFinkelstein DissertationOslo SaputraNo ratings yet
- Cliques in Cms High Schools and The Consequences Final PaperDocument8 pagesCliques in Cms High Schools and The Consequences Final Paperapi-441877801No ratings yet
- Responding To Ten Common Delirium Misconceptions With Best Evidence: An Educational Review For CliniciansDocument7 pagesResponding To Ten Common Delirium Misconceptions With Best Evidence: An Educational Review For CliniciansdkdkdsNo ratings yet
- Psychotomimetic DrugsDocument372 pagesPsychotomimetic DrugsDenise Wladyka Cortis100% (2)
- Psychotherapy. Theory, Research and Practice - E. GendlinDocument12 pagesPsychotherapy. Theory, Research and Practice - E. GendlinCamilo IgnacioNo ratings yet
- Cause and Effect of Depression in TeenagersDocument12 pagesCause and Effect of Depression in TeenagersAfreen ZahraNo ratings yet
- 06-01 SHAMDASANI - SW and CG Jung Mediumship, Psychiatry and Serial Exemplarity PDFDocument15 pages06-01 SHAMDASANI - SW and CG Jung Mediumship, Psychiatry and Serial Exemplarity PDFLívia BarbosaNo ratings yet
- The Assessment Interview in Clinical NeuropsychologyDocument33 pagesThe Assessment Interview in Clinical NeuropsychologyNohora Johanna Rondón100% (1)
- 122 Lecture 1 Milieu TherapyDocument7 pages122 Lecture 1 Milieu TherapyDENNIS N. MUÑOZNo ratings yet
- Mental Health NursingDocument28 pagesMental Health NursingSanthosh.S.U100% (3)
- Phobias Phobias PhobiasDocument2 pagesPhobias Phobias PhobiasMhae ShahNo ratings yet
- I. General ObjectiveDocument5 pagesI. General ObjectiveMr. BQNo ratings yet
- Mindfulness Coloring ActivityDocument12 pagesMindfulness Coloring Activityapi-504640248No ratings yet
- Petersen Et Al 1993 PDFDocument14 pagesPetersen Et Al 1993 PDFAnjali YadavNo ratings yet
- Application of Cognitive Behavioral Theories To Interpersonal Practice PDFDocument17 pagesApplication of Cognitive Behavioral Theories To Interpersonal Practice PDFK Indumathy GanesanNo ratings yet
- Managing The Side Effects of Psychotropic Medications 2Nd Edition Joseph F Goldberg Carrie L Ernst Online Ebook Texxtbook Full Chapter PDFDocument69 pagesManaging The Side Effects of Psychotropic Medications 2Nd Edition Joseph F Goldberg Carrie L Ernst Online Ebook Texxtbook Full Chapter PDFcatherine.nobles446100% (9)
- Delhi PsychiatryDocument7 pagesDelhi PsychiatryPrarthana SagarNo ratings yet
- Mental Healthcare Act 2017Document29 pagesMental Healthcare Act 2017amit1109No ratings yet
- Treatment ModalitiesDocument79 pagesTreatment ModalitiesShelly Mae AciertoNo ratings yet
- When The Patient's Symptoms Match The Following Criteria Documented in The DSM-IV, The Diagnosis of GAD Is ConfirmedDocument30 pagesWhen The Patient's Symptoms Match The Following Criteria Documented in The DSM-IV, The Diagnosis of GAD Is ConfirmedDivine Burlas AzarconNo ratings yet
- Hagi Tudose RezumatDocument2 pagesHagi Tudose RezumatMIRCEA100% (1)
- Group Art TherapyDocument15 pagesGroup Art TherapyClau Pedraza100% (1)
- Crosby Jesse M Acceptance and Commitment Therapy For 2016Document33 pagesCrosby Jesse M Acceptance and Commitment Therapy For 2016Sergio De PanfilisNo ratings yet
- Case StudyDocument5 pagesCase StudyDerby Febriani Sultany100% (1)
- A Story of Triumph Over Manic DepressionDocument4 pagesA Story of Triumph Over Manic DepressionclaroblancoNo ratings yet
- Violence, Older Adults, and Serious Mental IllnessDocument10 pagesViolence, Older Adults, and Serious Mental IllnessJosé Manuel SalasNo ratings yet
- O Esmeralda - Dias Carlos Amaral - Melanie Klein S Concept of Counter-Transference - ARTICOLDocument3 pagesO Esmeralda - Dias Carlos Amaral - Melanie Klein S Concept of Counter-Transference - ARTICOLRaluca MariaNo ratings yet