
Stress Ulcer
Stress Ulcer
You might also like
- Urology MCQsDocument13 pagesUrology MCQsRahmah Shah Bahai83% (6)
- (Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingDocument27 pages(Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingamalNo ratings yet
- Peptic UlcerDocument36 pagesPeptic Ulcersable1804No ratings yet
- Presentation FucoidanDocument42 pagesPresentation FucoidanTaufik Akbar Faried LubisNo ratings yet
- Stomach PathologyDocument123 pagesStomach PathologyDoc On CallNo ratings yet
- Acute Gastric Mucosal LesionDocument19 pagesAcute Gastric Mucosal LesionadystiNo ratings yet
- Peptic Ulcer A Review On Etiology and PathogenesisDocument5 pagesPeptic Ulcer A Review On Etiology and PathogenesisEsti Suryani Haro MuntheNo ratings yet
- Peptic Ulcer Disease m1Document60 pagesPeptic Ulcer Disease m1frankozed1No ratings yet
- Pediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapDocument10 pagesPediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapvgmanjunathNo ratings yet
- 01 Ijms 228 22Document8 pages01 Ijms 228 22BRNSS Publication Hub InfoNo ratings yet
- Pros Tag Land Ins, NSAIDs, and Gastric Mucosal ProtectionDocument20 pagesPros Tag Land Ins, NSAIDs, and Gastric Mucosal ProtectionLeo LopesNo ratings yet
- Gastritis: Palangka Raya University Faculty of MedicineDocument32 pagesGastritis: Palangka Raya University Faculty of MedicineAnonymNo ratings yet
- A Patient With Caustic Ingestion Injury: Brinna Anindita Budi WidodoDocument27 pagesA Patient With Caustic Ingestion Injury: Brinna Anindita Budi WidodoBrinna Anindita SatriaNo ratings yet
- Inv Eusebi RevDocument9 pagesInv Eusebi Revfernandadexiree.melendezNo ratings yet
- PSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionDocument7 pagesPSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionMichael TobilobaNo ratings yet
- Peptic Ulcer PDFDocument9 pagesPeptic Ulcer PDFNurarsyiNo ratings yet
- Peptic Ulcer PDFDocument9 pagesPeptic Ulcer PDFJahanvi aundhiyaNo ratings yet
- Antibiotic in CDDocument11 pagesAntibiotic in CDYaseerNo ratings yet
- Digestion GM Eng 2020Document49 pagesDigestion GM Eng 2020snowrose2609No ratings yet
- Clinical Manifestations, Causes and Management Strategies of Peptic Ulcer DiseaseDocument9 pagesClinical Manifestations, Causes and Management Strategies of Peptic Ulcer DiseaseAmanda SaphiraNo ratings yet
- The gut microbiota in IBDDocument10 pagesThe gut microbiota in IBDhomer1794No ratings yet
- Etiology of Peptic Ulcer DiseaseDocument4 pagesEtiology of Peptic Ulcer Diseaseshufi100% (1)
- Pepti C Ul Cer Dis Ea SeDocument36 pagesPepti C Ul Cer Dis Ea Segerald_ichigoNo ratings yet
- Gastritis: Ns. M. Ali Hamid, M. Kes., CWCCADocument86 pagesGastritis: Ns. M. Ali Hamid, M. Kes., CWCCAindri damayantiNo ratings yet
- Gastroenterology Clinics PDFDocument211 pagesGastroenterology Clinics PDFjackNo ratings yet
- Probiotic Use For Necrotizing Enterocolitis in The Newborn: Is It Effective?Document16 pagesProbiotic Use For Necrotizing Enterocolitis in The Newborn: Is It Effective?Cyd WardNo ratings yet
- Molecules 28 06811Document35 pagesMolecules 28 06811Nejc KovačNo ratings yet
- Gastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanDocument8 pagesGastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanMaikka IlaganNo ratings yet
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDocument82 pagesGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- P. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Document308 pagesP. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Anonymous 1EQutBNo ratings yet
- Peptic Ulcer DiseaseDocument36 pagesPeptic Ulcer DiseasenkpthapanNo ratings yet
- Pathogenesis of PD Yr2 2007 B&WDocument65 pagesPathogenesis of PD Yr2 2007 B&WPurwana NasirNo ratings yet
- Reviews: Immunity, Microbiota and Kidney DiseaseDocument12 pagesReviews: Immunity, Microbiota and Kidney DiseaseEss liNo ratings yet
- The Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringDocument5 pagesThe Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringMariaNo ratings yet
- BronkiektasisDocument25 pagesBronkiektasisgowindamijayaNo ratings yet
- Tonolini2013Acute Nonsteroidal Anti-Inflammatory Drug-Induced ColitisDocument4 pagesTonolini2013Acute Nonsteroidal Anti-Inflammatory Drug-Induced ColitisKito TongHuiNo ratings yet
- BBLR 2Document8 pagesBBLR 2Riza ShihabudinNo ratings yet
- Kuliah Modul Gi 2013Document155 pagesKuliah Modul Gi 2013ck dwnNo ratings yet
- Harrisons Principles of Internal Medicine, 19th EditionDocument22 pagesHarrisons Principles of Internal Medicine, 19th EditionTALBIYAH SABDAH RIZAN TAUPIQ -No ratings yet
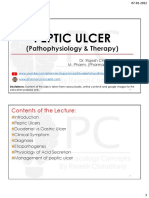
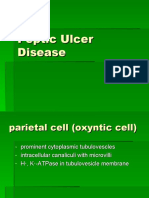
- Peptic Ulcer Disease: J. Rashma 2015 BATCHDocument16 pagesPeptic Ulcer Disease: J. Rashma 2015 BATCHRashma JosephNo ratings yet
- 10 Peptic Ulcer IntroDocument7 pages10 Peptic Ulcer Introb_rahman2k39603No ratings yet
- Peptic Ulcer DiseaseDocument16 pagesPeptic Ulcer DiseaseRashma JosephNo ratings yet
- Unit 3 Gastrointestinal Disorders P2 Peptic UlcerDocument43 pagesUnit 3 Gastrointestinal Disorders P2 Peptic UlcerShashidharan MenonNo ratings yet
- Ibd GDDocument15 pagesIbd GDAndi SusiloNo ratings yet
- Intestinal Microbiota UCDocument11 pagesIntestinal Microbiota UCreadalotbutnowisdomyetNo ratings yet
- Hpy 1Document2 pagesHpy 1Neil AlviarNo ratings yet
- OWC Part16Document29 pagesOWC Part16Boby FaesalNo ratings yet
- Petunjuk Praktikum Git 2015Document79 pagesPetunjuk Praktikum Git 2015KharisulNo ratings yet
- Pathophysiology of PUDDocument8 pagesPathophysiology of PUDmngyuNo ratings yet
- Journal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithDocument14 pagesJournal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithShakeel AhmedNo ratings yet
- Diagnosis and Management of Benign Gastric and Duodenal DiseaseDocument16 pagesDiagnosis and Management of Benign Gastric and Duodenal DiseaseMaría Lourdes Rodríguez ZavalaNo ratings yet
- 2021 Gut Microbiome PsoDocument4 pages2021 Gut Microbiome PsoDianaNo ratings yet
- JCM 12 04442Document17 pagesJCM 12 04442lata.pauccaraNo ratings yet
- Kunyit and GasterDocument7 pagesKunyit and GasterulilNo ratings yet
- Lect - Peptic Ulcer - 211020 - 182113Document38 pagesLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelNo ratings yet
- GIT OSPE Pathology - Final-2 PDFDocument29 pagesGIT OSPE Pathology - Final-2 PDFafaq alismailiNo ratings yet
- Acne e Nutrição 2Document9 pagesAcne e Nutrição 2BeNo ratings yet
- GastritisDocument64 pagesGastritisaparna shamaNo ratings yet
- Inflammatory Bowel Disease: Translating Basic Science into Clinical PracticeFrom EverandInflammatory Bowel Disease: Translating Basic Science into Clinical PracticeNo ratings yet
- Sulfur Cures 2000Document34 pagesSulfur Cures 2000ocoxodoNo ratings yet
- Bladder Diverticulum and SepsisDocument4 pagesBladder Diverticulum and SepsisInternational Medical PublisherNo ratings yet
- HONK by AijazDocument40 pagesHONK by AijazMuhammad Imran AlamNo ratings yet
- Final ReflectionDocument4 pagesFinal Reflectionapi-314231777No ratings yet
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 pagesHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Dialysis Drugs 2010Document8 pagesDialysis Drugs 2010Pradhani Fakhira DhaneswariNo ratings yet
- General Consent For Treatment Form Oct 2016Document2 pagesGeneral Consent For Treatment Form Oct 2016Dewi Ratna SariNo ratings yet
- CirrhosisDocument10 pagesCirrhosisJénny AnnNo ratings yet
- Abdominal AssessmentDocument2 pagesAbdominal AssessmentJan Jamison ZuluetaNo ratings yet
- ReseachDocument3 pagesReseachWen TingNo ratings yet
- Turner SyndromeDocument4 pagesTurner SyndromeKylalerrsssNo ratings yet
- Ear MoppingDocument18 pagesEar MoppingSarah Eddiah0% (1)
- IV InsertionDocument1 pageIV InsertionCherisse Delos SantosNo ratings yet
- MaritimeFloatingStaff ClaimForHospitalisationTreatmentDocument3 pagesMaritimeFloatingStaff ClaimForHospitalisationTreatmentSidhartha MishraNo ratings yet
- Cyclophosphamide For Injection, USPDocument2 pagesCyclophosphamide For Injection, USPemilia candraNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care Planssairej06100% (3)
- Macapaz, EBR SBARDocument2 pagesMacapaz, EBR SBARpius troy macapazNo ratings yet
- Introduction To Computer in DentistryDocument5 pagesIntroduction To Computer in Dentistry4gen_3No ratings yet
- Marte, Zara (MR#102155742) Printed by VILLACIS, MARILOU (1000042364)Document7 pagesMarte, Zara (MR#102155742) Printed by VILLACIS, MARILOU (1000042364)roxdigitalNo ratings yet
- Case Study For Peri-Appendiceal AbcessDocument79 pagesCase Study For Peri-Appendiceal Abcessmarife100% (5)
- HyperthyroidismDocument54 pagesHyperthyroidismAsiah JelitaNo ratings yet
- Course Task 7 NCMA 111Document1 pageCourse Task 7 NCMA 111Marian TorresNo ratings yet
- Glaucoma 2003Document24 pagesGlaucoma 2003Aryu-hanafiey BoyzzsNo ratings yet
- Major Bioethical PrinciplesDocument44 pagesMajor Bioethical PrinciplesDr. Liza Manalo50% (2)
- Nosocomial Infections in NewbornsDocument10 pagesNosocomial Infections in NewbornsAntony Rose AbyNo ratings yet
- Health Care Delivery Models and Nursing Practice 2Document6 pagesHealth Care Delivery Models and Nursing Practice 2DennisNo ratings yet
- Bobath ArticleDocument8 pagesBobath ArticleChristopher Chew Dian MingNo ratings yet
- International Journal of Recent Scientific ResearchDocument5 pagesInternational Journal of Recent Scientific ResearchifahInayahNo ratings yet






















































































Download as ppt, pdf, or txt
You might also like
- Urology MCQsDocument13 pagesUrology MCQsRahmah Shah Bahai83% (6)
- (Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingDocument27 pages(Such As Digestive Enzymes, Acid and Bile) : How The Stomach and Intestine Avaoid BeeingamalNo ratings yet
- Peptic UlcerDocument36 pagesPeptic Ulcersable1804No ratings yet
- Presentation FucoidanDocument42 pagesPresentation FucoidanTaufik Akbar Faried LubisNo ratings yet
- Stomach PathologyDocument123 pagesStomach PathologyDoc On CallNo ratings yet
- Acute Gastric Mucosal LesionDocument19 pagesAcute Gastric Mucosal LesionadystiNo ratings yet
- Peptic Ulcer A Review On Etiology and PathogenesisDocument5 pagesPeptic Ulcer A Review On Etiology and PathogenesisEsti Suryani Haro MuntheNo ratings yet
- Peptic Ulcer Disease m1Document60 pagesPeptic Ulcer Disease m1frankozed1No ratings yet
- Pediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapDocument10 pagesPediatric Gastritis, Gastropathy, and Peptic Ulcer Disease: Education GapvgmanjunathNo ratings yet
- 01 Ijms 228 22Document8 pages01 Ijms 228 22BRNSS Publication Hub InfoNo ratings yet
- Pros Tag Land Ins, NSAIDs, and Gastric Mucosal ProtectionDocument20 pagesPros Tag Land Ins, NSAIDs, and Gastric Mucosal ProtectionLeo LopesNo ratings yet
- Gastritis: Palangka Raya University Faculty of MedicineDocument32 pagesGastritis: Palangka Raya University Faculty of MedicineAnonymNo ratings yet
- A Patient With Caustic Ingestion Injury: Brinna Anindita Budi WidodoDocument27 pagesA Patient With Caustic Ingestion Injury: Brinna Anindita Budi WidodoBrinna Anindita SatriaNo ratings yet
- Inv Eusebi RevDocument9 pagesInv Eusebi Revfernandadexiree.melendezNo ratings yet
- PSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionDocument7 pagesPSG 252 Lecture 4 Peptic Ulcer and Gastro ProtectionMichael TobilobaNo ratings yet
- Peptic Ulcer PDFDocument9 pagesPeptic Ulcer PDFNurarsyiNo ratings yet
- Peptic Ulcer PDFDocument9 pagesPeptic Ulcer PDFJahanvi aundhiyaNo ratings yet
- Antibiotic in CDDocument11 pagesAntibiotic in CDYaseerNo ratings yet
- Digestion GM Eng 2020Document49 pagesDigestion GM Eng 2020snowrose2609No ratings yet
- Clinical Manifestations, Causes and Management Strategies of Peptic Ulcer DiseaseDocument9 pagesClinical Manifestations, Causes and Management Strategies of Peptic Ulcer DiseaseAmanda SaphiraNo ratings yet
- The gut microbiota in IBDDocument10 pagesThe gut microbiota in IBDhomer1794No ratings yet
- Etiology of Peptic Ulcer DiseaseDocument4 pagesEtiology of Peptic Ulcer Diseaseshufi100% (1)
- Pepti C Ul Cer Dis Ea SeDocument36 pagesPepti C Ul Cer Dis Ea Segerald_ichigoNo ratings yet
- Gastritis: Ns. M. Ali Hamid, M. Kes., CWCCADocument86 pagesGastritis: Ns. M. Ali Hamid, M. Kes., CWCCAindri damayantiNo ratings yet
- Gastroenterology Clinics PDFDocument211 pagesGastroenterology Clinics PDFjackNo ratings yet
- Probiotic Use For Necrotizing Enterocolitis in The Newborn: Is It Effective?Document16 pagesProbiotic Use For Necrotizing Enterocolitis in The Newborn: Is It Effective?Cyd WardNo ratings yet
- Molecules 28 06811Document35 pagesMolecules 28 06811Nejc KovačNo ratings yet
- Gastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanDocument8 pagesGastrointestinal Disorders in Children Part Ii: Dra. Ruby Ann PunongbayanMaikka IlaganNo ratings yet
- Gastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDDocument82 pagesGastritis: Department of Gastroenterology General Hospital of Ningxia Medical University Si Cen MDAvi Themessy100% (1)
- P. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Document308 pagesP. Tonino - Gastritis and Gastric Cancer - New Insights in Gastroprot., Diag.,Trtmts (2011, Intech)Anonymous 1EQutBNo ratings yet
- Peptic Ulcer DiseaseDocument36 pagesPeptic Ulcer DiseasenkpthapanNo ratings yet
- Pathogenesis of PD Yr2 2007 B&WDocument65 pagesPathogenesis of PD Yr2 2007 B&WPurwana NasirNo ratings yet
- Reviews: Immunity, Microbiota and Kidney DiseaseDocument12 pagesReviews: Immunity, Microbiota and Kidney DiseaseEss liNo ratings yet
- The Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringDocument5 pagesThe Gut Microbiota Tumorigenesis and Liver Diseases 2017 EngineeringMariaNo ratings yet
- BronkiektasisDocument25 pagesBronkiektasisgowindamijayaNo ratings yet
- Tonolini2013Acute Nonsteroidal Anti-Inflammatory Drug-Induced ColitisDocument4 pagesTonolini2013Acute Nonsteroidal Anti-Inflammatory Drug-Induced ColitisKito TongHuiNo ratings yet
- BBLR 2Document8 pagesBBLR 2Riza ShihabudinNo ratings yet
- Kuliah Modul Gi 2013Document155 pagesKuliah Modul Gi 2013ck dwnNo ratings yet
- Harrisons Principles of Internal Medicine, 19th EditionDocument22 pagesHarrisons Principles of Internal Medicine, 19th EditionTALBIYAH SABDAH RIZAN TAUPIQ -No ratings yet
- Peptic Ulcer Disease: J. Rashma 2015 BATCHDocument16 pagesPeptic Ulcer Disease: J. Rashma 2015 BATCHRashma JosephNo ratings yet
- 10 Peptic Ulcer IntroDocument7 pages10 Peptic Ulcer Introb_rahman2k39603No ratings yet
- Peptic Ulcer DiseaseDocument16 pagesPeptic Ulcer DiseaseRashma JosephNo ratings yet
- Unit 3 Gastrointestinal Disorders P2 Peptic UlcerDocument43 pagesUnit 3 Gastrointestinal Disorders P2 Peptic UlcerShashidharan MenonNo ratings yet
- Ibd GDDocument15 pagesIbd GDAndi SusiloNo ratings yet
- Intestinal Microbiota UCDocument11 pagesIntestinal Microbiota UCreadalotbutnowisdomyetNo ratings yet
- Hpy 1Document2 pagesHpy 1Neil AlviarNo ratings yet
- OWC Part16Document29 pagesOWC Part16Boby FaesalNo ratings yet
- Petunjuk Praktikum Git 2015Document79 pagesPetunjuk Praktikum Git 2015KharisulNo ratings yet
- Pathophysiology of PUDDocument8 pagesPathophysiology of PUDmngyuNo ratings yet
- Journal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithDocument14 pagesJournal of Periodontology - 2021 - Lu - Effect of Adjunctive Systemic Antibiotics On Microbial Populations Compared WithShakeel AhmedNo ratings yet
- Diagnosis and Management of Benign Gastric and Duodenal DiseaseDocument16 pagesDiagnosis and Management of Benign Gastric and Duodenal DiseaseMaría Lourdes Rodríguez ZavalaNo ratings yet
- 2021 Gut Microbiome PsoDocument4 pages2021 Gut Microbiome PsoDianaNo ratings yet
- JCM 12 04442Document17 pagesJCM 12 04442lata.pauccaraNo ratings yet
- Kunyit and GasterDocument7 pagesKunyit and GasterulilNo ratings yet
- Lect - Peptic Ulcer - 211020 - 182113Document38 pagesLect - Peptic Ulcer - 211020 - 182113Puranjay ChandelNo ratings yet
- GIT OSPE Pathology - Final-2 PDFDocument29 pagesGIT OSPE Pathology - Final-2 PDFafaq alismailiNo ratings yet
- Acne e Nutrição 2Document9 pagesAcne e Nutrição 2BeNo ratings yet
- GastritisDocument64 pagesGastritisaparna shamaNo ratings yet
- Inflammatory Bowel Disease: Translating Basic Science into Clinical PracticeFrom EverandInflammatory Bowel Disease: Translating Basic Science into Clinical PracticeNo ratings yet
- Sulfur Cures 2000Document34 pagesSulfur Cures 2000ocoxodoNo ratings yet
- Bladder Diverticulum and SepsisDocument4 pagesBladder Diverticulum and SepsisInternational Medical PublisherNo ratings yet
- HONK by AijazDocument40 pagesHONK by AijazMuhammad Imran AlamNo ratings yet
- Final ReflectionDocument4 pagesFinal Reflectionapi-314231777No ratings yet
- HOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDDocument61 pagesHOSPITAL ASSOCIATED Infections Overcoming Emerging Challenge by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- Dialysis Drugs 2010Document8 pagesDialysis Drugs 2010Pradhani Fakhira DhaneswariNo ratings yet
- General Consent For Treatment Form Oct 2016Document2 pagesGeneral Consent For Treatment Form Oct 2016Dewi Ratna SariNo ratings yet
- CirrhosisDocument10 pagesCirrhosisJénny AnnNo ratings yet
- Abdominal AssessmentDocument2 pagesAbdominal AssessmentJan Jamison ZuluetaNo ratings yet
- ReseachDocument3 pagesReseachWen TingNo ratings yet
- Turner SyndromeDocument4 pagesTurner SyndromeKylalerrsssNo ratings yet
- Ear MoppingDocument18 pagesEar MoppingSarah Eddiah0% (1)
- IV InsertionDocument1 pageIV InsertionCherisse Delos SantosNo ratings yet
- MaritimeFloatingStaff ClaimForHospitalisationTreatmentDocument3 pagesMaritimeFloatingStaff ClaimForHospitalisationTreatmentSidhartha MishraNo ratings yet
- Cyclophosphamide For Injection, USPDocument2 pagesCyclophosphamide For Injection, USPemilia candraNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care Planssairej06100% (3)
- Macapaz, EBR SBARDocument2 pagesMacapaz, EBR SBARpius troy macapazNo ratings yet
- Introduction To Computer in DentistryDocument5 pagesIntroduction To Computer in Dentistry4gen_3No ratings yet
- Marte, Zara (MR#102155742) Printed by VILLACIS, MARILOU (1000042364)Document7 pagesMarte, Zara (MR#102155742) Printed by VILLACIS, MARILOU (1000042364)roxdigitalNo ratings yet
- Case Study For Peri-Appendiceal AbcessDocument79 pagesCase Study For Peri-Appendiceal Abcessmarife100% (5)
- HyperthyroidismDocument54 pagesHyperthyroidismAsiah JelitaNo ratings yet
- Course Task 7 NCMA 111Document1 pageCourse Task 7 NCMA 111Marian TorresNo ratings yet
- Glaucoma 2003Document24 pagesGlaucoma 2003Aryu-hanafiey BoyzzsNo ratings yet
- Major Bioethical PrinciplesDocument44 pagesMajor Bioethical PrinciplesDr. Liza Manalo50% (2)
- Nosocomial Infections in NewbornsDocument10 pagesNosocomial Infections in NewbornsAntony Rose AbyNo ratings yet
- Health Care Delivery Models and Nursing Practice 2Document6 pagesHealth Care Delivery Models and Nursing Practice 2DennisNo ratings yet
- Bobath ArticleDocument8 pagesBobath ArticleChristopher Chew Dian MingNo ratings yet
- International Journal of Recent Scientific ResearchDocument5 pagesInternational Journal of Recent Scientific ResearchifahInayahNo ratings yet