Download as ppt, pdf, or txt
You might also like
- Plab 2 MaterialDocument24 pagesPlab 2 MaterialradugaNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- Altered Mental Status CMR1Document63 pagesAltered Mental Status CMR1Angeline HernandezNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- Cushings, Addisons and Acromegaly: DR J Storrow FY2Document38 pagesCushings, Addisons and Acromegaly: DR J Storrow FY2abdalkhalidNo ratings yet
- Introduction & Gen Management of Toxic ConditionsDocument12 pagesIntroduction & Gen Management of Toxic Conditionsblue sapphireNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- NCMB316 Rle 2-10-7addison's DiseaseDocument4 pagesNCMB316 Rle 2-10-7addison's DiseaseMaica LectanaNo ratings yet
- Causes of Diffuse Hyperpigmentation EndocrinopathiesDocument9 pagesCauses of Diffuse Hyperpigmentation EndocrinopathiesAbdul QuyyumNo ratings yet
- 632 Ijar-5063Document6 pages632 Ijar-5063Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- EBM - 5. Adrenal DisordersDocument101 pagesEBM - 5. Adrenal DisordersBRI KUNo ratings yet
- Cushing TH 4Document13 pagesCushing TH 4syaymaNo ratings yet
- Tutorial 10 CorticosteroidsDocument16 pagesTutorial 10 CorticosteroidsToqa ElmansouryNo ratings yet
- Addison DiseaseDocument23 pagesAddison DiseaseKompari EvansNo ratings yet
- Cushings SyndromeDocument2 pagesCushings SyndromeCourtney HammonsNo ratings yet
- Medical Emergencies in Rehabilitation MedicineDocument24 pagesMedical Emergencies in Rehabilitation MedicineAzza El Awar100% (1)
- NCMB316 Week 7: Course Unit 6Document5 pagesNCMB316 Week 7: Course Unit 6Armand Bong SantiagoNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument5 pagesAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaNo ratings yet
- Cushing's SyndromeDocument5 pagesCushing's SyndromesummerduskNo ratings yet
- Adrenal and Pitutary Disoreders Adigrat LecDocument144 pagesAdrenal and Pitutary Disoreders Adigrat Lecbereket gashuNo ratings yet
- Clinicalworksheet 5Document6 pagesClinicalworksheet 5MoniqueNo ratings yet
- Lecture: Adrenal DisordersDocument78 pagesLecture: Adrenal DisordersOchendo KingxNo ratings yet
- 2005 H Diagnostic Si TratamentDocument9 pages2005 H Diagnostic Si TratamentCaulfield DariaNo ratings yet
- What Is CushingDocument10 pagesWhat Is CushingkuroroexileNo ratings yet
- Endocrinology 101 150Document29 pagesEndocrinology 101 150Ahmed El AlfyNo ratings yet
- Endocrine SystemDocument59 pagesEndocrine Systemayesharajput5110No ratings yet
- Reye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkaraDocument7 pagesReye'S Syndrome: Mrs. Smitha.M Associate Professor Vijaya College of Nursing KottarakkarakrishnasreeNo ratings yet
- Adrenal Gland Diseades L 7band 8Document31 pagesAdrenal Gland Diseades L 7band 8lanasalah.mNo ratings yet
- Poison 1Document24 pagesPoison 1Scott LarsonNo ratings yet
- Shaina Dionisia Palacol Candice Guillermo Gelzan RoldanDocument55 pagesShaina Dionisia Palacol Candice Guillermo Gelzan RoldanEdelrose LapitanNo ratings yet
- FMcase 8Document12 pagesFMcase 8Ryan Townsend100% (1)
- 6.28.10 Barnes Adrenal InsufficiencyDocument19 pages6.28.10 Barnes Adrenal InsufficiencySami OmerNo ratings yet
- 20 Endocrine Disease and AnaesthesiaDocument0 pages20 Endocrine Disease and AnaesthesiajuniorebindaNo ratings yet
- Progressive Muscle Weakness: More There Than Meets The Eye: Im Board ReviewDocument7 pagesProgressive Muscle Weakness: More There Than Meets The Eye: Im Board Reviewbdalcin5512No ratings yet
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocument24 pagesAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalNo ratings yet
- Endocrinology NotesDocument12 pagesEndocrinology Notesrandiey john abelleraNo ratings yet
- Preassignment Work-Careplan #2Document30 pagesPreassignment Work-Careplan #2djbhetaNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Points MRCP 2Document6 pagesPoints MRCP 2safi abroNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- Endocrine Disorders and DrugsDocument149 pagesEndocrine Disorders and DrugsJaypee Fabros Edra100% (1)
- Endocrine and Metabolic Disease RevisionDocument3 pagesEndocrine and Metabolic Disease RevisionAmanda MurphyNo ratings yet
- CushingDocument3 pagesCushingaiki parkNo ratings yet
- Endocrine SystemDocument11 pagesEndocrine Systemmaglangitjoannamarie1920No ratings yet
- CushingDocument4 pagesCushingavinash dhameriyaNo ratings yet
- Adrenal Diseases: Types Aetiology Diagnosis Complications TreatmentDocument29 pagesAdrenal Diseases: Types Aetiology Diagnosis Complications Treatmentgani7222No ratings yet
- Type 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsDocument6 pagesType 1 Diabetes Mellitus Clinical Presentation - History, Physical Examination, ComplicationsTrifosa Ika Septiana EryaniNo ratings yet
- Adrenal InsufficiencyDocument25 pagesAdrenal InsufficiencyMustafa Salam M.NooriNo ratings yet
- Cushing's SyndromeDocument35 pagesCushing's SyndromeShankara Pillai100% (3)
- Cushing Syndrome: M.Sc. (N) 1 YearDocument30 pagesCushing Syndrome: M.Sc. (N) 1 YearRanjana SharmaNo ratings yet
- Adrenal Gland DisordersDocument79 pagesAdrenal Gland DisordersMohamed BamashmoosNo ratings yet
- Addison's DseDocument9 pagesAddison's DseKath RubioNo ratings yet
- Department of Internal Medicine Ii and Phthysiatry: - Rajkumar Subasaravanan Subgroup "12"Document36 pagesDepartment of Internal Medicine Ii and Phthysiatry: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Adrenocortical HyperfunctionDocument132 pagesAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Cushing SyndromeDocument5 pagesCushing Syndromearif mahammad bhuniyaNo ratings yet
- REPORTDocument13 pagesREPORTEarlou MagbanuaNo ratings yet
- Hyper-cortisolism (Cushing Syndrome), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-cortisolism (Cushing Syndrome), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Chronic Disease Management for Small AnimalsFrom EverandChronic Disease Management for Small AnimalsW. Dunbar GramNo ratings yet
- CreamsDocument17 pagesCreamsSolomonNo ratings yet
- The Best Things To Do in Binghamton NYDocument4 pagesThe Best Things To Do in Binghamton NYShashank SangwanNo ratings yet
- Activated Carbon From BambooDocument19 pagesActivated Carbon From BambooErik WeeksNo ratings yet
- Spot LightDocument216 pagesSpot LightCristopherZartaNo ratings yet
- Annex 3 - 5-Revised EMFDocument3 pagesAnnex 3 - 5-Revised EMFVholts Villa VitugNo ratings yet
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- Singapore Math Worksheets Grade 3 MeasurementDocument8 pagesSingapore Math Worksheets Grade 3 MeasurementKungfu Math100% (1)
- Chapter - 10: Reaching The Age of AdolescenceDocument11 pagesChapter - 10: Reaching The Age of AdolescenceDestroy YtNo ratings yet
- Unit IV-Alternative Laboratory ExerciseDocument11 pagesUnit IV-Alternative Laboratory ExerciseFloralde RyanNo ratings yet
- Pentavitin - DSMDocument3 pagesPentavitin - DSMRnD Roi SuryaNo ratings yet
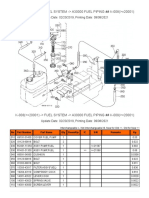
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Analette Manual Service Rev. D 2-6-08Document149 pagesAnalette Manual Service Rev. D 2-6-08RosanaCriolloNo ratings yet
- Seal Gas FlowDocument2 pagesSeal Gas FlowoluwasolNo ratings yet
- Review of WAG Field ExperienceDocument10 pagesReview of WAG Field ExperienceJavier E. Guerrero ArrietaNo ratings yet
- Timing Protection in AUTOSAR ISO 26262Document10 pagesTiming Protection in AUTOSAR ISO 26262Joseph KymmNo ratings yet
- SDM-v1 0Document32 pagesSDM-v1 0Franz NussmannNo ratings yet
- 59 Why Nuts and Bolts Come Loose V1Document2 pages59 Why Nuts and Bolts Come Loose V1civicbladeNo ratings yet
- JuvenilleDocument5 pagesJuvenilleelviemjmontemayorNo ratings yet
- Domestic ViolenceDocument17 pagesDomestic ViolenceKhairul IdzwanNo ratings yet
- Gordon's Functional HealthDocument2 pagesGordon's Functional HealthReina ArabelleNo ratings yet
- Ctu (Zuuu) PDFDocument45 pagesCtu (Zuuu) PDFchang woo yunNo ratings yet
- OutbreakWksht UpdatedMay18 ADocument3 pagesOutbreakWksht UpdatedMay18 ASatya DwiparthaNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)
- Barrel Firing - Paul WandlessDocument9 pagesBarrel Firing - Paul WandlessStefan Van Cleemput0% (1)
- Leister Plastic-Welding BR Plastic-Fabrication EN PDFDocument48 pagesLeister Plastic-Welding BR Plastic-Fabrication EN PDFDuong DoanNo ratings yet
- 10 Transport in Plants Neet Biology Model Question PaperDocument5 pages10 Transport in Plants Neet Biology Model Question PaperJosephNo ratings yet
- 2022 Tucson Plug in Hybrid Emergency Response Quick Reference GuideDocument2 pages2022 Tucson Plug in Hybrid Emergency Response Quick Reference GuideForum PompieriiNo ratings yet
- Master Circular 16 Compassionate GroundDocument13 pagesMaster Circular 16 Compassionate GroundSHANMUGA VADIVEL SUNDARARAJANNo ratings yet
- DRRR2324 Q4 DRRDocument7 pagesDRRR2324 Q4 DRRh4gtg7n55gNo ratings yet
- Chemistry Ibdp Exam Syle QuestionsDocument37 pagesChemistry Ibdp Exam Syle QuestionsGEORGE MATTHEWNo ratings yet