Download as ppt, pdf, or txt
You might also like
- Quick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamDocument19 pagesQuick Review/Pearl Sheet: These Are in Random Order To Help You Prepare For You NBME ExamWyoXPat100% (12)
- Nitration of Benzoic Acid To Produce Methyl 3-Nitrobenzoate: PH C CH O (O) Phcooh HNO H SO Cooh CH OH H SO CoochDocument2 pagesNitration of Benzoic Acid To Produce Methyl 3-Nitrobenzoate: PH C CH O (O) Phcooh HNO H SO Cooh CH OH H SO CoochAleem AhmedNo ratings yet
- Urban Land Use - Community-Based PlanningDocument316 pagesUrban Land Use - Community-Based PlanningAnonymous 5poler100% (1)
- EC2 GuidanceDocument32 pagesEC2 GuidanceVenkadesh Periathambi50% (4)
- Unit 2 Section 2.1 Earth Inside and OutDocument5 pagesUnit 2 Section 2.1 Earth Inside and OutMercedes Muñoz GarcíaNo ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Aplastic Anemia: Review of Etiology and TreatmentDocument7 pagesAplastic Anemia: Review of Etiology and TreatmentCleber MaiaNo ratings yet
- Case Study Output Aplastic AnemiaDocument7 pagesCase Study Output Aplastic AnemiaColeen Angelique MontenegroNo ratings yet
- Aplastic Anemia, 2008Document10 pagesAplastic Anemia, 2008j.doe.hex_87No ratings yet
- Aplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRDocument42 pagesAplastic Anemia - An Overview: DR Aniruddh Shrivastava Guided By: DR S.H. Talib SIRdoctoranswerit_84161No ratings yet
- Aplastic AnemiaDocument5 pagesAplastic Anemiascremo_xtremeNo ratings yet
- Bone Marrow Hypoplasia 2023Document34 pagesBone Marrow Hypoplasia 2023Dafne LunaNo ratings yet
- Bone Marrow Hypoplasia 2022Document34 pagesBone Marrow Hypoplasia 2022Jose Angel Cobian GaliciaNo ratings yet
- Bone Marrow Failure VoiceoverDocument18 pagesBone Marrow Failure Voiceoverياسر كوثر هانيNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Bone Marrow FailureDocument4 pagesBone Marrow Failuremedicomauro2No ratings yet
- Aplastic Anemia (Dr. Kadek)Document41 pagesAplastic Anemia (Dr. Kadek)galuh dharmapatniNo ratings yet
- Sisay Berane 083 PancytopeniaDocument23 pagesSisay Berane 083 PancytopeniaRas Siko SafoNo ratings yet
- Hematological Clinical HistoryDocument7 pagesHematological Clinical HistoryScribdTranslationsNo ratings yet
- Aplastic Anemia: BY-Dr. Abhishek Singh Asstt. Professor Deptt. of MedicineDocument20 pagesAplastic Anemia: BY-Dr. Abhishek Singh Asstt. Professor Deptt. of MedicineChandra EkaNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Aplastic AnemiaDocument6 pagesAplastic AnemiaChukwu Henry ParadiseNo ratings yet
- غير معروف Acute Leukemia-7 (Muhadharaty)Document78 pagesغير معروف Acute Leukemia-7 (Muhadharaty)aliabumrfghNo ratings yet
- Aa by AbdifatahDocument57 pagesAa by AbdifatahAbdifatah AhmedNo ratings yet
- Normocytic AnemiaDocument16 pagesNormocytic AnemiaPaula ArayaNo ratings yet
- Aplastic Anemia Is A NormocyticDocument17 pagesAplastic Anemia Is A NormocyticAfrio ArismanNo ratings yet
- Bleeding DisordersDocument14 pagesBleeding Disordersahmedsalih1888No ratings yet
- MRCPass Notes For MRCP 1 - HEMATOLOGYDocument9 pagesMRCPass Notes For MRCP 1 - HEMATOLOGYsabdali100% (1)
- Aplastic AnemiaDocument26 pagesAplastic AnemiaIrina Moldovan100% (1)
- DIBDDocument11 pagesDIBDKabirNo ratings yet
- Erythrocyte Life Cycle: PathophysiologyDocument15 pagesErythrocyte Life Cycle: PathophysiologyYeniNo ratings yet
- Approach To Patient With Cytopenias: H. Atilla Özkan, MDDocument48 pagesApproach To Patient With Cytopenias: H. Atilla Özkan, MDYabetsNo ratings yet
- Assignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-KeelaniDocument6 pagesAssignment 1 Pathology Aplastic Anemia: Supervisor: DR - Ramez Al-Keelaniameer mousaNo ratings yet
- Aplastic AnemiaDocument11 pagesAplastic Anemiaquidditch07No ratings yet
- AnemiaDocument51 pagesAnemiaAravind A SNo ratings yet
- INTRO in AnemiaDocument3 pagesINTRO in AnemiaJeraiza Mendoza-LizarondoNo ratings yet
- Osler-Weber-Rendu Disease - StatPearls - NCBI BookshelfDocument4 pagesOsler-Weber-Rendu Disease - StatPearls - NCBI BookshelfanaNo ratings yet
- Bone Marrow Failure and Severe Aplastic Anemia Revision 1.1Document3 pagesBone Marrow Failure and Severe Aplastic Anemia Revision 1.1Rasha Al MousaNo ratings yet
- Non-Pharmacological Measures: PacemakerDocument11 pagesNon-Pharmacological Measures: PacemakerAlmendra Olenka LSNo ratings yet
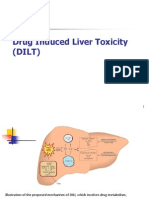
- Drug Induced Liver Toxicity (DILD)Document39 pagesDrug Induced Liver Toxicity (DILD)Surya Pratama100% (1)
- What Is Aplastic Anemia?Document23 pagesWhat Is Aplastic Anemia?Ayi SuwarayiNo ratings yet
- Sickle Cell PresentationDocument4 pagesSickle Cell PresentationJoan ChoiNo ratings yet
- Universidad Privada San Juan Bautista: Escuela de Medicina HumanaDocument6 pagesUniversidad Privada San Juan Bautista: Escuela de Medicina HumanaKarolLeylaNo ratings yet
- Aplastic Anemia and HomoeopathyDocument3 pagesAplastic Anemia and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (1)
- HemophiliaDocument62 pagesHemophiliamuhirwa Samuel100% (1)
- Jurnal: Lila Esi Mustika, Amkg NIK: PK2013050Document11 pagesJurnal: Lila Esi Mustika, Amkg NIK: PK2013050lilaNo ratings yet
- Aplastic Anemia: A Case Study OnDocument10 pagesAplastic Anemia: A Case Study OnVidge GrospeNo ratings yet
- Case 1Document7 pagesCase 1secretNo ratings yet
- Aplastic AnemiaDocument6 pagesAplastic AnemiaJoezer Gumangan VeranoNo ratings yet
- Disorders of BloodDocument3 pagesDisorders of BloodCondurache Ilie-AndreiNo ratings yet
- Aplastic Anemia ThesisDocument7 pagesAplastic Anemia Thesiscandicehimwarren100% (2)
- The Spleen: Schwartz's Principles of Surgery 11th EdDocument54 pagesThe Spleen: Schwartz's Principles of Surgery 11th EdaddelinsNo ratings yet
- Chapter 49Document6 pagesChapter 49Melissa Aina Mohd YusofNo ratings yet
- 2009 Pearl SheetDocument19 pages2009 Pearl Sheetmikez100% (1)
- Hematology Topics 16-20Document20 pagesHematology Topics 16-20Angelo Jude CobachaNo ratings yet
- Anemia: Differential DiagnosisDocument7 pagesAnemia: Differential DiagnosisZaman MigozaradNo ratings yet
- Blood DisordersDocument8 pagesBlood DisordersDeevashwer Rathee100% (1)
- Usmle World Step 2 NotesDocument241 pagesUsmle World Step 2 NotesAdnan MallickNo ratings yet
- The Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaFrom EverandThe Complete Guide on Anemia: Learn Anemia Symptoms, Anemia Causes, and Anemia Treatments. Anemia types covered in full details: Iron-deficiency, Microcytic, Autoimmune Hemolytic, Sideroblastic, and Normocytic AnemiaRating: 3.5 out of 5 stars3.5/5 (10)
- Draft Part 1. Choose The Best Single Answer (BSA) by Encircling Its Corresponding LetterDocument11 pagesDraft Part 1. Choose The Best Single Answer (BSA) by Encircling Its Corresponding LetterKhadar mohamedNo ratings yet
- New Pediatric Guideline Hargeisa Group Hospital by DR NelsonDocument54 pagesNew Pediatric Guideline Hargeisa Group Hospital by DR NelsonKhadar mohamedNo ratings yet
- Cardiology ExamDocument9 pagesCardiology ExamKhadar mohamedNo ratings yet
- EMQs in SurgeryDocument25 pagesEMQs in Surgerynob2011nob100% (2)
- Virology MCQDocument8 pagesVirology MCQKhadar mohamedNo ratings yet
- Steroid Dysregulation and Stomatodynia (Burning Mouth Syndrome)Document9 pagesSteroid Dysregulation and Stomatodynia (Burning Mouth Syndrome)EnzoNo ratings yet
- FirexDocument8 pagesFirexSE KongNo ratings yet
- Lab 5 ImineDocument10 pagesLab 5 ImineCheng FuNo ratings yet
- Note On NMHPDocument23 pagesNote On NMHPDeepak MalhotraNo ratings yet
- The Bio-Terror Bible - Exposing The Coming Bio-Terror PandemicDocument2,903 pagesThe Bio-Terror Bible - Exposing The Coming Bio-Terror Pandemicspy7777777guyNo ratings yet
- Project ReportDocument60 pagesProject ReportPrashant Bankar33% (6)
- 2023 Neurology ABCC Article ListDocument12 pages2023 Neurology ABCC Article Listlakshminivas PingaliNo ratings yet
- CBSE Class 12 Biology Question Paper 2020 Set 2Document6 pagesCBSE Class 12 Biology Question Paper 2020 Set 2Rajendra SolankiNo ratings yet
- Furuno Installation ManualDocument35 pagesFuruno Installation ManualZakaria Chowdhury71% (7)
- Agriculture Reporting: 1st Place - Joshua Kato, New VisionDocument1 pageAgriculture Reporting: 1st Place - Joshua Kato, New VisionAfrican Centre for Media ExcellenceNo ratings yet
- Electrical Safety HAE EM EPS GDCC ES PDFDocument17 pagesElectrical Safety HAE EM EPS GDCC ES PDFkhleifat_613891No ratings yet
- Preventive MaintenanceDocument26 pagesPreventive MaintenanceVijai KaladadNo ratings yet
- Rescission of Insurance ContractsDocument12 pagesRescission of Insurance ContractsCari Mangalindan MacaalayNo ratings yet
- Different Types of BuffetDocument6 pagesDifferent Types of BuffetShitij MarkanNo ratings yet
- Company Profile - PretechDocument26 pagesCompany Profile - PretechanandivmNo ratings yet
- Lesson 3Document21 pagesLesson 3Carylle Shayne MarcellanaNo ratings yet
- Unit 1: Overview of The Strategic Planning ProcessDocument11 pagesUnit 1: Overview of The Strategic Planning ProcessAmeng GosimNo ratings yet
- EFFECTS OF MORINGA OLEIFERA LEAF MEAL (MOLM) ON GROWTH AND LAYING PERFORMANCE, AND CARCASS CHARACTERISTICS OF 4-WEEKS-OLD JAPANESE QUAILS (Coturnix Coturnix Japonica)Document7 pagesEFFECTS OF MORINGA OLEIFERA LEAF MEAL (MOLM) ON GROWTH AND LAYING PERFORMANCE, AND CARCASS CHARACTERISTICS OF 4-WEEKS-OLD JAPANESE QUAILS (Coturnix Coturnix Japonica)Victor BenanteNo ratings yet
- Pain Management ServiceDocument4 pagesPain Management ServiceTaeng GoNo ratings yet
- Axial Piston Closed Circuit Pumps: Series 42Document76 pagesAxial Piston Closed Circuit Pumps: Series 42Евгений ГубаревNo ratings yet
- Standard Specs 11 STD Spec For PSV Rev0Document14 pagesStandard Specs 11 STD Spec For PSV Rev0sumit kumarNo ratings yet
- Sugar Production in Uttar Pradesh Over The Last 10 YearsDocument3 pagesSugar Production in Uttar Pradesh Over The Last 10 YearsAryan KediaNo ratings yet
- The Gujarat ModelDocument15 pagesThe Gujarat ModelThakur_rvsNo ratings yet
- 4-Point Action Plan by Esperanza and Brian CabralDocument6 pages4-Point Action Plan by Esperanza and Brian CabralRapplerNo ratings yet
- Hansen 2008Document30 pagesHansen 2008Jacobo CeballosNo ratings yet
- Playground Antonyms PDFDocument2 pagesPlayground Antonyms PDFChayne RodilNo ratings yet