Download as ppt, pdf, or txt
You might also like
- Anesthesia Board Review Flashcards - QuizletDocument47 pagesAnesthesia Board Review Flashcards - QuizletDENTAL REVIEWER ONLY100% (1)
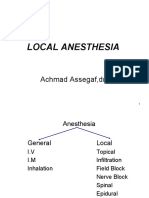
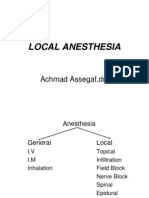
- Local Anesthesia: Achmad Assegaf, DR., SP - AnDocument48 pagesLocal Anesthesia: Achmad Assegaf, DR., SP - AnDesty ArianiNo ratings yet
- Anesthesia PharmacologyDocument41 pagesAnesthesia PharmacologyHassan.shehri88% (8)
- Anesthesia For Open Abdominal Aortic SurgeryDocument18 pagesAnesthesia For Open Abdominal Aortic SurgeryAurora TrifaNo ratings yet
- Local Anesthesia: Achmad Assegaf, DR., SP - AnDocument48 pagesLocal Anesthesia: Achmad Assegaf, DR., SP - AnDesty ArianiNo ratings yet
- 2021-9-7 Local AnestheticsDocument33 pages2021-9-7 Local AnestheticsNOT ZUXNo ratings yet
- Local Anesthetics and Nerve Blocks HannanDocument57 pagesLocal Anesthetics and Nerve Blocks Hannanpriya_edwinNo ratings yet
- Local Anesthetics and Nerve Blocks HannanDocument57 pagesLocal Anesthetics and Nerve Blocks Hannanpriya_edwinNo ratings yet
- Locac AnaestheticsDocument31 pagesLocac AnaestheticsfadhiliNo ratings yet
- Local Anesthesia in Large AnimalsDocument53 pagesLocal Anesthesia in Large AnimalsNot SayingNo ratings yet
- L.A 2015Document32 pagesL.A 2015Eisha BatoolNo ratings yet
- Local AnaesthesiaDocument35 pagesLocal Anaesthesiamealiella omar100% (1)
- Local Anesthetics 2019-2020 2nd YrDocument54 pagesLocal Anesthetics 2019-2020 2nd YrJolaine ValloNo ratings yet
- Local AnesthesiaDocument65 pagesLocal AnesthesiaAlex HoNo ratings yet
- Local Anesthetics in DentistryDocument25 pagesLocal Anesthetics in Dentistryiahim_ulizamNo ratings yet
- LOCAL ANAESTHESIA and Drugs and Mechanism of Action in DetailDocument19 pagesLOCAL ANAESTHESIA and Drugs and Mechanism of Action in DetailkhandarkarjayNo ratings yet
- Regional Anesthesia: Bagian Farmakologi Fakultas Kedokteran Universitas LampungDocument26 pagesRegional Anesthesia: Bagian Farmakologi Fakultas Kedokteran Universitas LampungKarimah Ihda Husna YainNo ratings yet
- Local Anaesthetic Agents (3) 2Document38 pagesLocal Anaesthetic Agents (3) 2MaleehaNo ratings yet
- Local AnaestheticsDocument42 pagesLocal Anaestheticsdiwakar4123sawNo ratings yet
- Local Anaesthetics: Mechanism of ActionDocument7 pagesLocal Anaesthetics: Mechanism of Actions.khan9211rediffmail.comNo ratings yet
- Local AnaestheticsDocument31 pagesLocal AnaestheticsNodi NodiNo ratings yet
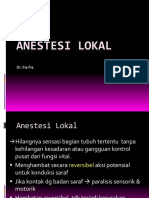
- Anestesi Lokal: Dr. Fia FiaDocument31 pagesAnestesi Lokal: Dr. Fia Fiaolga adhityaNo ratings yet
- Pharmacology of Local Anesthetics IDocument93 pagesPharmacology of Local Anesthetics IAlshaimaa AhmedNo ratings yet
- Local Anesthetic AgentDocument21 pagesLocal Anesthetic AgentSiti Fatimah IsmailNo ratings yet
- MalamedDocument8 pagesMalamedDr. DhDhNo ratings yet
- Local Anesthetics SabinDocument69 pagesLocal Anesthetics Sabinsabin7000No ratings yet
- LA Chap 3Document55 pagesLA Chap 3karan patelNo ratings yet
- Local AnestheticsDocument30 pagesLocal AnestheticsmaurinmarceoiaNo ratings yet
- Local Anesthetics 08 OctDocument35 pagesLocal Anesthetics 08 OctLawrence WanderiNo ratings yet
- Local AnestheticsDocument24 pagesLocal AnestheticsBismah SaeedNo ratings yet
- Local Anesthetic AgentsDocument42 pagesLocal Anesthetic AgentsyohannesNo ratings yet
- Pharmacology of Local AnestheticsDocument71 pagesPharmacology of Local AnestheticsMaha MohamedNo ratings yet
- Local AnaestheticsDocument52 pagesLocal AnaestheticsDustyNo ratings yet
- Local AnestheticsDocument45 pagesLocal AnestheticsAubrey Monette Padilla-ItchonNo ratings yet
- Local and Gen AnaestheticsDocument55 pagesLocal and Gen AnaestheticsH.M. PiashNo ratings yet
- Local Anaesthesia: Department of Anaesthesia University of Cape TownDocument0 pagesLocal Anaesthesia: Department of Anaesthesia University of Cape TownjuniorebindaNo ratings yet
- Anestesi RegionalDocument72 pagesAnestesi RegionalMarissa RusyaniNo ratings yet
- Local Anesthesia in Oral and Maxillofacial SurgeryDocument17 pagesLocal Anesthesia in Oral and Maxillofacial SurgeryChhan SambathNo ratings yet
- Local Anaesthetic AgentsDocument21 pagesLocal Anaesthetic AgentsSuresh KumarNo ratings yet
- Pediatric Exdontia - BDS YR 4Document75 pagesPediatric Exdontia - BDS YR 4Elamaaraeen MadhvanNo ratings yet
- Local Anesthetics (Pharmacology Lecture)Document4 pagesLocal Anesthetics (Pharmacology Lecture)Jay-r Villanueva100% (1)
- Anestesi Pada Operasi Mata by PikalDocument60 pagesAnestesi Pada Operasi Mata by PikalSyahpikal SahanaNo ratings yet
- Anesthetic SubstancesDocument12 pagesAnesthetic SubstancesNewPhoneWhoDisNo ratings yet
- Local Anesthesia in Dental and Nerve BlockDocument42 pagesLocal Anesthesia in Dental and Nerve BlockRahul SrivastavaNo ratings yet
- Local Anaesthetics Sum SheetDocument2 pagesLocal Anaesthetics Sum Sheetnzq7m6ph4dNo ratings yet
- Anaesthetic and Muscle Relaxant Agents: DR David N.MusyokaDocument43 pagesAnaesthetic and Muscle Relaxant Agents: DR David N.MusyokaIrene Zae MwandotoNo ratings yet
- Ans 7 Local Anaesthetic AgentDocument40 pagesAns 7 Local Anaesthetic Agentyounas63No ratings yet
- Local Anesthetics 1Document35 pagesLocal Anesthetics 1DONI HERIANTONo ratings yet
- Local Anesthetics: By, DR Ashwani V PG1 YearDocument29 pagesLocal Anesthetics: By, DR Ashwani V PG1 YearAshwani V ShekharNo ratings yet
- Anesthesiology 3Document27 pagesAnesthesiology 3Ayesha JamshaidNo ratings yet
- Ocular AnesthesiaDocument61 pagesOcular AnesthesiaAdarsh Keshari100% (1)
- TVP-2023-0506 Local Anesthetic AgentsDocument7 pagesTVP-2023-0506 Local Anesthetic AgentsvetthamilNo ratings yet
- Local Anaesthetics: For BdsDocument47 pagesLocal Anaesthetics: For BdsDr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Cocaine Corneal Sloughing: Low Potency (Short DOA)Document4 pagesCocaine Corneal Sloughing: Low Potency (Short DOA)Thulasi tootsieNo ratings yet
- Anesthetic Agents Ga/La: Rabindra AdhikaryDocument40 pagesAnesthetic Agents Ga/La: Rabindra AdhikaryAnaliza Kitongan LantayanNo ratings yet
- Local Anaesthetics PPT by Dr. Chandkiran YadavDocument81 pagesLocal Anaesthetics PPT by Dr. Chandkiran YadavPawan Jain82% (17)
- Chapter 4 LaDocument4 pagesChapter 4 LaDindin Lou MendozaNo ratings yet
- Local AnestheticsDocument93 pagesLocal Anestheticsgeetika100% (1)
- Anestesi Regional: M. Dwi SatriyantoDocument60 pagesAnestesi Regional: M. Dwi SatriyantoviyolaazzahraNo ratings yet
- Local Anaesthetic2007 1Document37 pagesLocal Anaesthetic2007 1bh8gm22t7nNo ratings yet
- Rle NotesDocument7 pagesRle NotesLorens Troy SoltisNo ratings yet
- Regional AnesthesiaDocument4 pagesRegional AnesthesiaRisha Ethel G. BerondoNo ratings yet
- 9 The Post Anesthesia Care UnitDocument77 pages9 The Post Anesthesia Care Unitsanjivdas100% (1)
- Jurnal Anestesi Lidokain ToksisitasDocument11 pagesJurnal Anestesi Lidokain ToksisitasAlda AdeliaNo ratings yet
- Boddeda Geetha SindhujaDocument13 pagesBoddeda Geetha SindhujaKarel de KlerkNo ratings yet
- Epidural and Combined Spinal-Epidural Anesthesia Techniques - UpToDateDocument54 pagesEpidural and Combined Spinal-Epidural Anesthesia Techniques - UpToDateHugo Robles Gómez100% (1)
- Local Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryDocument8 pagesLocal Anesthesia and Anxiolytic Techniques For Oculoplastic SurgeryFrancisco Javier Rodriguez MolinaNo ratings yet
- Local AnestheticsDocument38 pagesLocal Anestheticsakanksha singhNo ratings yet
- Anesth ThesisDocument11 pagesAnesth ThesisAkshay HariNo ratings yet
- Anesthesia For The Patient With Preeclampsia - UpToDateDocument31 pagesAnesthesia For The Patient With Preeclampsia - UpToDateJazivi AlejoNo ratings yet
- Surgical TechniqueDocument52 pagesSurgical TechniqueKutub SikderNo ratings yet
- KSPAN Recognition and Treatment of Local Anesthetic Systemic ToxicityDocument39 pagesKSPAN Recognition and Treatment of Local Anesthetic Systemic ToxicityAli AftabNo ratings yet
- Anaesthesia in Endodontics: Eirini Fragouli, Georgios Dechouniotis, Maria GeorgopoulouDocument14 pagesAnaesthesia in Endodontics: Eirini Fragouli, Georgios Dechouniotis, Maria GeorgopoulouShriya ShahuNo ratings yet
- Drug Study For HELLP SyndromeDocument19 pagesDrug Study For HELLP SyndromeRosemarie CarpioNo ratings yet
- Applied Head and Neck Anatomy For The Facial Cosmetic SurgeonDocument245 pagesApplied Head and Neck Anatomy For The Facial Cosmetic SurgeonDaniel Emilev0% (1)
- Postoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - IdDocument23 pagesPostoperative Analgesia in Modified Radical Mastectomy Patients After Instillation of Bupivacaine Through Surgical Drains-1.en - Idsatria divaNo ratings yet
- Surgical SkillsDocument47 pagesSurgical SkillsSamah SuhailNo ratings yet
- 2006, Vol.19, Issues 2, Ocular Anesthesia PDFDocument156 pages2006, Vol.19, Issues 2, Ocular Anesthesia PDFalvyandaniNo ratings yet
- Hyperbaric Versus Plain Bupivacaine For Spinal.20Document9 pagesHyperbaric Versus Plain Bupivacaine For Spinal.20Della Elvina RoeslandNo ratings yet
- US - Article - 1col - Peri-Op - June22Document12 pagesUS - Article - 1col - Peri-Op - June22Odett NuñezNo ratings yet
- Drugs in Dentistry: D.A. Haas, DDS, PHD, FRCDCDocument9 pagesDrugs in Dentistry: D.A. Haas, DDS, PHD, FRCDCahmed_awad_360% (1)
- Local Anesthetic Systemic ToxicityDocument1 pageLocal Anesthetic Systemic Toxicitylaurad.benavidesNo ratings yet
- Epidural Anesthesia (OB)Document3 pagesEpidural Anesthesia (OB)zooNo ratings yet
- Medical Emergencies in The Dental OfficeDocument23 pagesMedical Emergencies in The Dental Officeতৌহিদ তপুNo ratings yet
- 10 1002@vms3 218Document17 pages10 1002@vms3 218Adriana PalmaNo ratings yet
- Fvets 04 00068Document12 pagesFvets 04 00068Didit HarysNo ratings yet
- Full Kit InfoDocument193 pagesFull Kit Inforamachari100% (1)
- Acog 2019-Obstetric Analgesia and AnesthesiaDocument18 pagesAcog 2019-Obstetric Analgesia and AnesthesiaPamela Rojas CossioNo ratings yet